Racial and Ethnic Disparities in Access to and Utilization of Care among Insured Adults
Executive Summary
Through its coverage expansions, the Affordable Care Act (ACA) provides an opportunity to reduce longstanding disparities in health insurance coverage for people of color, which may contribute to improvements in their access to and utilization of care. However, many factors beyond health insurance influence individuals’ ability to obtain care. As such, one key question is the extent to which people of color may continue to experience disparities in access to and utilization of care even after ACA implementation. To provide greater insight into this question, this analysis examines differences in access to and utilization of care for Black and Hispanic adults compared to White adults among those who are uninsured, enrolled in Medicaid, and privately insured. It is based on data from the 2014 Kaiser Survey of Low-Income Americans.
The findings show that, consistent with other research, both Medicaid and private coverage are associated with improvements in access to and utilization of care compared to being uninsured, and these differences generally hold true for White, Black, and Hispanic adults. However, privately insured Black and Hispanic adults fare worse than privately insured White adults along several measures of access to and utilization of care and have less confidence in their ability to afford medical costs. Fewer differences are seen between Blacks and Hispanics compared to Whites among uninsured adults and Medicaid enrollees, and where there are differences, Blacks and Hispanics fare better relative to Whites in most cases (Table 1).
| ES Table 1: Differences in How Black and Hispanic Adults Fare Relative to Whites with Same Coverage Type for Selected Measures of Access, Utilization, and Financial Confidence | ||||||
| Uninsured | Medicaid Enrollees | Privately Insured | ||||
| Black compared to White | Hispanic compared to White | Black compared to White | Hispanic compared to White | Black compared to White | Hispanic compared to White | |
| Access to Care | ||||||
| Usual Source of Care | Worse | Worse | ||||
| Regular Provider | Worse | Worse | ||||
| Postponing/Going without Care | Better | Better | ||||
| Postponing/Going without Care Due to Cost | Better | Better | Better | |||
| Utilization of Care | ||||||
| Use of Medical Services | Worse | |||||
| Use of Preventive Services | Better | Worse | ||||
| Confidence in Ability to Afford Medical Costs | ||||||
| Usual Medical Costs | Worse | Worse | Worse | |||
| Major Medical Costs | Worse | Worse | Worse | |||
Among uninsured adults, Hispanics are less likely than Whites to delay or forgo care and more likely to receive preventive care. Black uninsured adults also are less likely than White uninsured adults to delay or forgo care due to cost. These differences may reflect uninsured Hispanics greater reliance on clinics for care relative to Whites, since clinics often have outreach and supportive services to connect patients to care. They also may reflect cultural differences in perceived need for care.
Among Medicaid enrollees, Hispanic adults are less likely than White adults to delay or forgo care, although no significant differences are observed among the share delaying or going without care due to cost. Hispanic adults have less confidence than White adults in their ability to afford usual and major medical costs. The small number of disparities observed among Medicaid enrollees may reflect the program’s role serving diverse and vulnerable low-income populations. Medicaid provides supportive services that can help connect individuals to care, such as transportation and case management. Moreover, Medicaid managed care plans and providers have significant experience serving diverse populations and may provide services designed to address their specific needs.
More differences are seen among privately insured adults, particularly for Hispanics compared to Whites. Among privately insured adults, Blacks and Hispanics are less likely than Whites to have a usual source of care and a regular provider, and less likely to have confidence in the ability to afford usual and major medical costs. In addition, Hispanics are less likely than Whites to use medical services or receive preventive care. While these differences may, in part, reflect the fact that Black and Hispanic privately insured adults have lower incomes than their White counterparts, the findings also suggest that other factors beyond cost are a substantial barrier to care.
Overall, the findings suggest that gains in health coverage under the ACA will lead to improvements in access to care and utilization for White, Black, and Hispanic adults. They also highlight the importance of increased attention to addressing racial and ethnic disparities in access to and utilization of care among privately insured adults, particularly as the privately insured population becomes more diverse as a result of greater enrollment of people of color into private plans through the ACA Marketplaces. Continued efforts by insurers and providers to target the specific linguistic, cultural, and social and environmental needs of these groups will be important to achieving greater equity in access to and utilization of care. Such efforts may build on lessons learned from successful strategies in Medicaid, given the program’s longstanding experience serving a diverse population.
Issue Brief
INTRODUCTION
People of color have historically had higher uninsured rates, experienced more barriers to care, and received poorer quality care compared to Whites, all contributing to worse health outcomes.1 ,2 The ACA health coverage expansions offer an opportunity to reduce the longstanding disparities in coverage among people of color. Recent data show declines in uninsured rates following implementation of the ACA, with larger declines for Blacks and Hispanics relative to Whites. However, Blacks and Hispanics still remain more likely to be uninsured than Whites.3
A large body of existing research suggests that these gains in health coverage will lead to improvements in access to and utilization of care. However, as the group of insured adults becomes more diverse, it is important to understand the extent to which people of color may continue to face disparities in access to and use of care even after ACA implementation. Many factors beyond coverage influence individuals’ access to and use of care, such as linguistic and cultural barriers as well as broad social and environmental factors. Existing research shows that even when controlling for health insurance, income, and other factors, people of color face increased barriers to care.4 ,5
This analysis provides greater insight into the extent to which Black and Hispanic adults with health coverage face disparities in access to and utilization of care and whether these disparities vary between Medicaid enrollees and privately insured adults. It is based on data from the 2014 Kaiser Survey of Low-Income Americans. The survey of 10,502 nonelderly adults was fielded between September 2 and December 15, 2014. Data were analyzed by type of health coverage, including uninsured, Medicaid, and private coverage, and racial and ethnic group, including Non-Hispanic Whites (Whites), Non-Hispanic Blacks (Blacks), and Hispanics. Analysis by additional racial/ethnic groups was not possible due to sample size limitations. Detail on the survey methods is available online.
BACKGROUND
Insurance Status
Based on the survey findings, approximately 11 million non-elderly adults were newly insured in 2014. Blacks and Hispanics were about twice as likely to report being newly insured as Whites (data not shown). Consistent with other recent analysis, this suggests narrowing in the longstanding disparities in coverage among Blacks and Hispanics. Among all insured adults, Blacks and Hispanics were significantly more likely than Whites to have Medicaid and less likely to have private coverage (Figure 1).

Demographic Characteristics and Health Status
In examining differences between Whites, Blacks, and Hispanics in access and utilization, it is important to understand how these groups differ in other ways that may impact access to care. Among uninsured and privately insured adults, Blacks and Hispanics have lower incomes relative to Whites, which may contribute to more financial barriers to care for these groups (Table 1). Among Medicaid enrollees, Hispanics are more likely than Whites to have income in the 139%-400% FPL range. Given that they are more likely to have children, this finding may reflect them being more likely to qualify through a pregnancy-related pathway, which typically has a higher eligibility limit than eligibility pathways for other adults.
Among uninsured adults, Medicaid enrollees, and privately insured adults, Hispanics are younger and more likely to have children than Whites, reflective of overall demographic patterns. Among uninsured and privately insured adults, Blacks are less likely than Whites to be married. Privately insured Hispanic adults are also less likely to be married than their Whites counterparts.
| Table 1: Selected Demographic Characteristics of Adults by Race/Ethnicity and Coverage Type | |||||||||||||||
| Uninsured | Medicaid | Private | |||||||||||||
| White | Black | Hispanic | White | Black | Hispanic | White | Black | Hispanic | |||||||
| Income | |||||||||||||||
| < 138% FPL | 47% | 59% | * | 62% | * | 81% | 77% | 77% | 9% | 23% | * | 20% | * | ||
| 139 – 400% FPL | 43% | 34% | 33% | * | 14% | 19% | 23% | * | 38% | 43% | 53% | * | |||
| >400% FPL | 10% | — | — | — | — | — | 54% | 34% | * | 28% | * | ||||
| Age | |||||||||||||||
| 19-25 | 17% | 18% | 29% | * | 13% | 19% | 28% | * | 9% | 14% | 19% | * | |||
| 26-34 | 29% | 33% | 26% | 20% | 15% | 12% | * | 18% | 21% | 22% | |||||
| 35-44 | 20% | 17% | 20% | 24% | 19% | 25% | 20% | 18% | 28% | * | |||||
| 45-64 | 34% | 32% | 24% | * | 44% | 47% | 35% | 52% | 47% | 31% | * | ||||
| Marital Status | |||||||||||||||
| Married | 33% | 11% | * | 28% | 25% | 17% | 32% | 69% | 35% | * | 56% | * | |||
| Not Married | 67% | 89% | * | 71% | 73% | 82% | 68% | 31% | 65% | * | 43% | * | |||
| Children | |||||||||||||||
| Children | 36% | 29% | 45% | * | 39% | 34% | 56% | * | 43% | 38% | 51% | * | |||
| No children | 64% | 70% | 54% | * | 60% | 66% | 44% | * | 57% | 62% | 49% | * | |||
| NOTES: “–“: Estimates with relative standard errors greater than 30% or with cell sizes less than 100 are not provided.* Indicates statistically significant difference from White, Non-Hispanic of same insurance type at p<0.05 level.SOURCE: 2014 Kaiser Survey of Low-Income Americans and the ACA. | |||||||||||||||
Among uninsured and privately insured adults, Hispanics are more likely than Whites to report fair or poor health (Table 2). However, across uninsured adults, Medicaid enrollees, and privately insured adults, Hispanics are less likely than Whites to report an ongoing condition. Among Medicaid enrollees and privately insured adults, Hispanics also are less likely to report taking a prescription drug. Privately insured Black adults also are less likely to report an ongoing condition or taking a prescription drug than their White counterparts.
| Table 2: Selected Measures of Health Status for Adults by Race/Ethnicity and Coverage Type | |||||||||||||||
| Uninsured | Medicaid | Private | |||||||||||||
| White | Black | Hispanic | White | Black | Hispanic | White | Black | Hispanic | |||||||
| Fair/Poor Health Status | 31% | 36% | 45% | * | 45% | 42% | 46% | 12% | 16% | 18% | * | ||||
| Fair/Poor Mental Health Status | 21% | 16% | 19% | 32% | 32% | 29% | 6% | 6% | 9% | ||||||
| Has an Ongoing Condition | 36% | 37% | 25% | * | 62% | 55% | 39% | * | 38% | 29% | * | 28% | * | ||
| Taking a Prescription Drug | 27% | 32% | 20% | 65% | 67% | 50% | * | 49% | 34% | * | 36% | * | |||
| NOTES: * Indicates statistically significant difference from White, Non-Hispanic of same insurance type at p<0.05 levelSOURCE: 2014 Kaiser Survey of Low-Income Americans and the ACA. | |||||||||||||||
Findings: Access, Utilization, and Financial Confidence
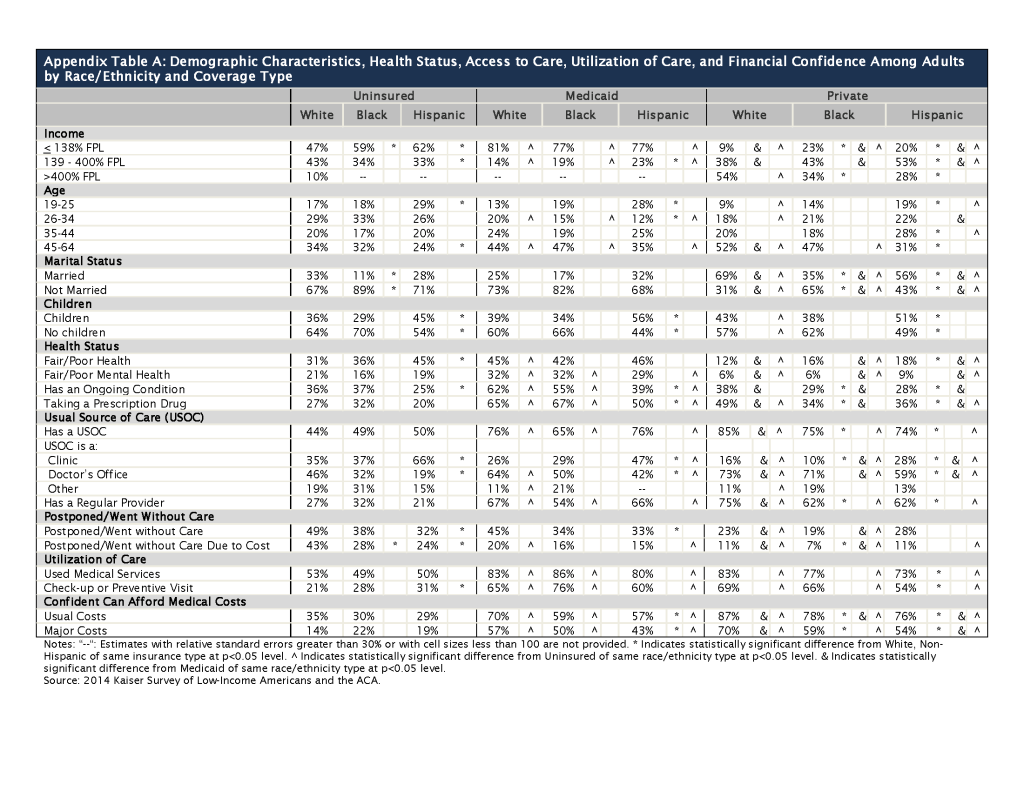
Consistent with other research, the findings show that Medicaid and private coverage are associated with improved access to and utilization of care compared to being uninsured, and these differences generally hold true for White, Black, and Hispanic adults. However, as shown below, privately insured Black and Hispanic adults fare worse than privately insured White adults along several measures of access to and use of care and have less confidence in their ability to afford medical costs. Fewer differences are seen between Blacks and Hispanics compared to Whites among uninsured adults and Medicaid enrollees. Moreover, where there are differences, Blacks and Hispanics fare better relative to Whites in most cases. (See Appendix Table A for complete findings).
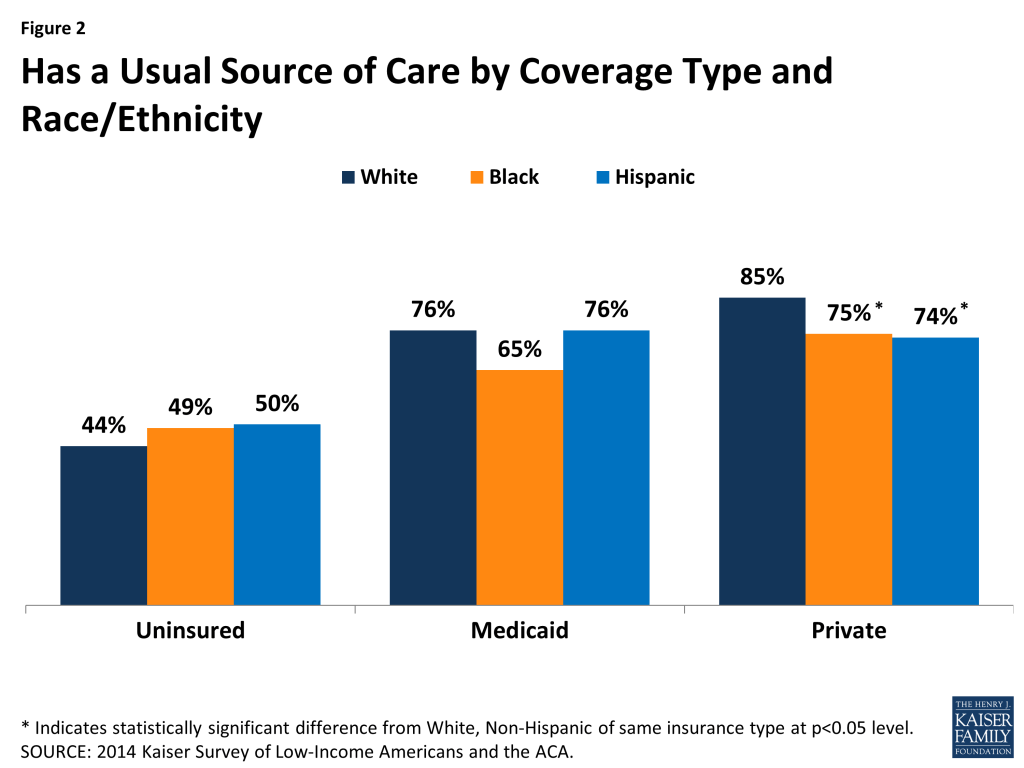
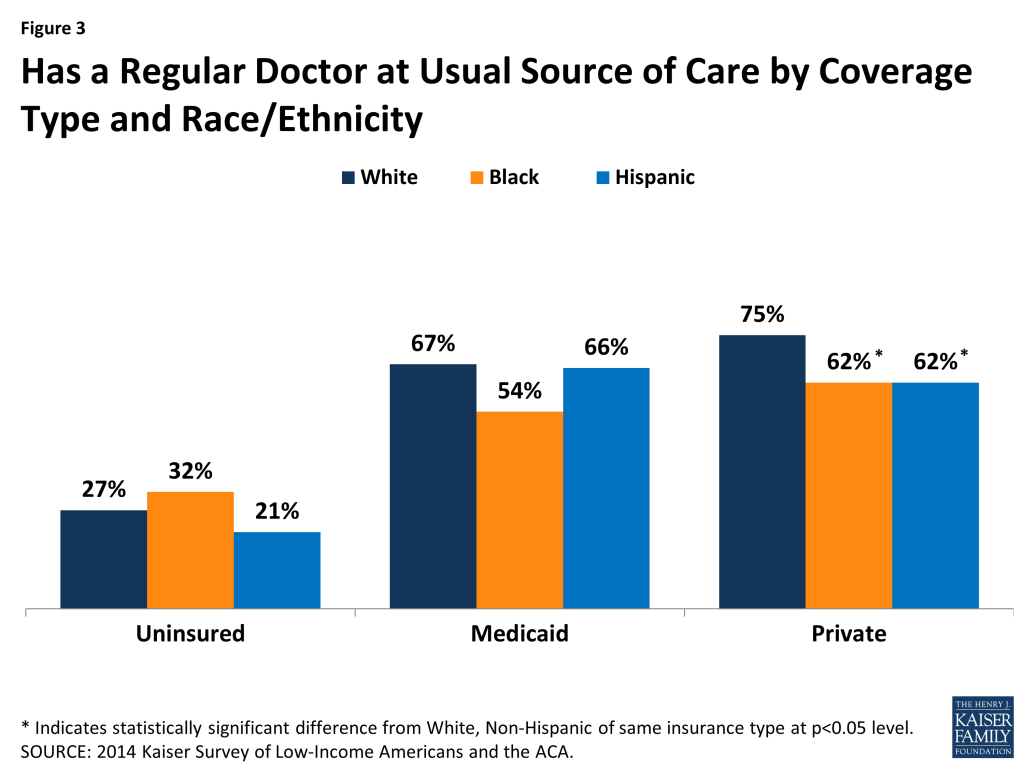
- Usual Source of Care and Regular Doctor. Among privately insured adults, Blacks and Hispanics are less likely than their White counterparts to report having a usual source of care or a regular provider (Figures 2 and 3). There are no significant differences between Blacks and Hispanics compared to Whites in these measures among uninsured adults and Medicaid enrollees.
- Type of Usual Source of Care. Among uninsured adults, Medicaid enrollees, and privately insured adults, Hispanics are more likely than Whites to rely on a clinic and less likely to have a doctor’s office as their usual source of care (Figure 4). In contrast, privately insured Black adults are less likely than their White counterparts to report a clinic as their usual source of care; there is no significant difference in the share relying on a doctor’s office

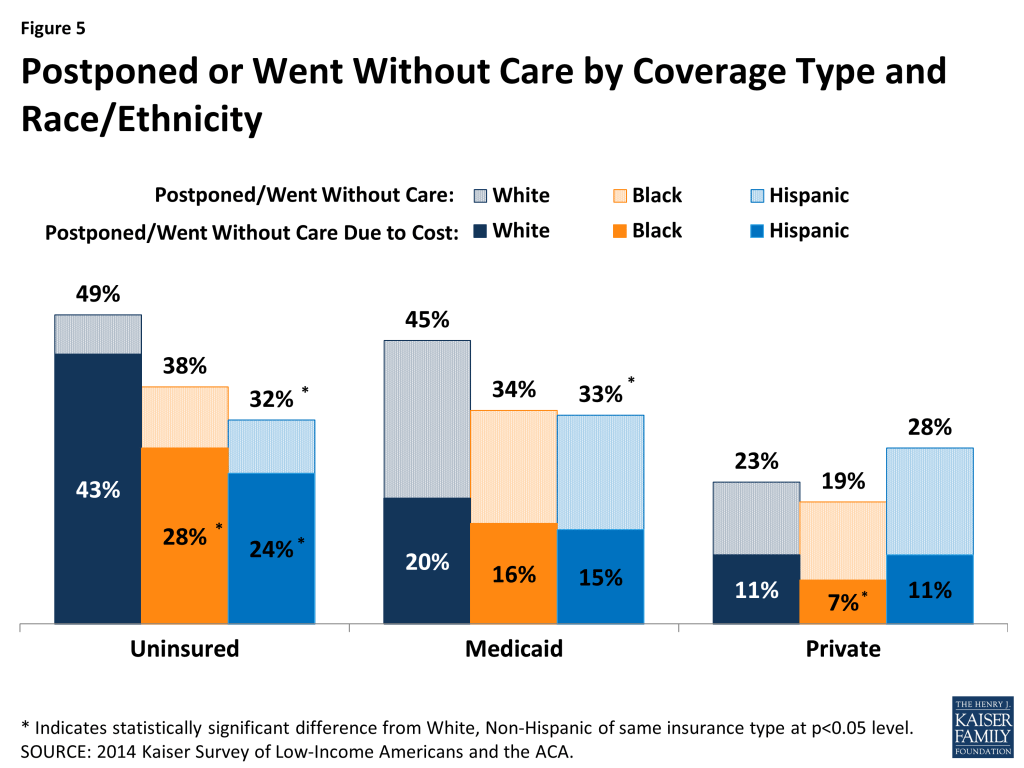
- Postponing or Going Without Care. Among uninsured adults, Medicaid enrollees, and privately insured adults, Blacks and Hispanics are not more likely than Whites to delay or go without care and, in some cases, fare better than Whites on these measures (Figure 5). Among uninsured adults, Hispanics are less likely than Whites to delay or go without care for any reason. In addition, Blacks and Hispanics are less likely than Whites to delay or go without care due to cost, despite having lower incomes relative to Whites. Among Medicaid enrollees, Hispanics are less likely than Whites to delay or go without care for any reason, and, among privately insured adults, Blacks are less likely than Whites to delay or go without care due to cost. Together these data also show that other barriers beyond cost appear to explain a large share of delayed or forgone care for Medicaid enrollees and privately insured adults, particularly for Black and Hispanic privately insured adults.
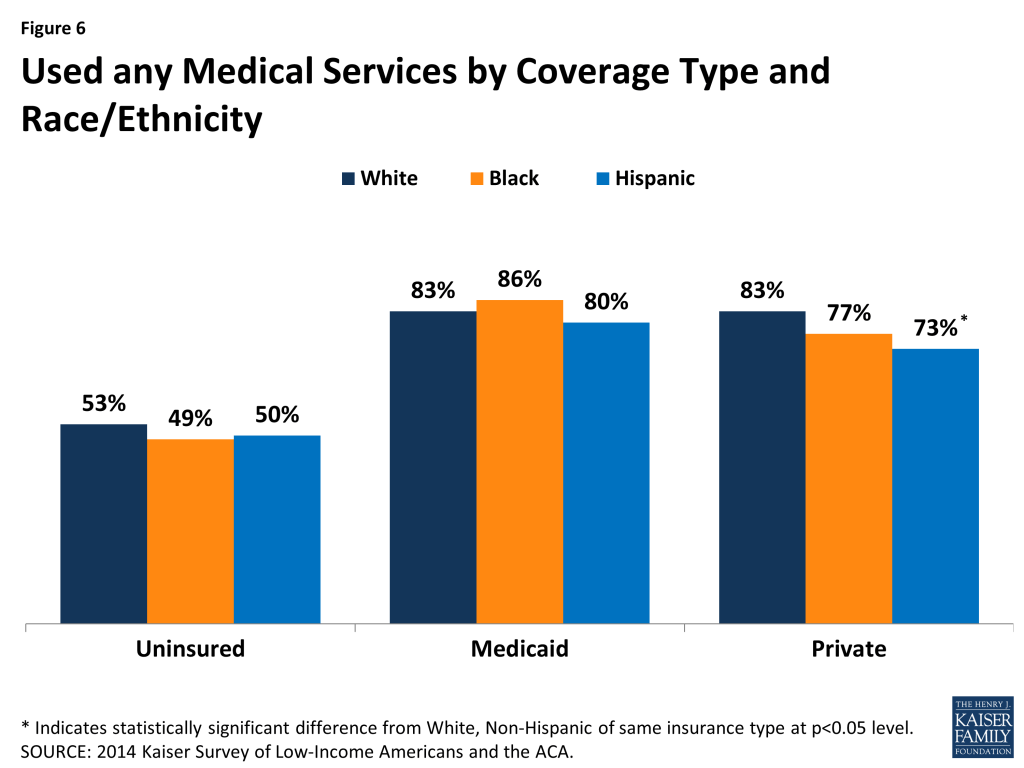
- Use of Medical Services. Among privately insured adults, Hispanics are less likely to report use of medical services than Whites (Figure 6). There are no significant differences in use of services for Blacks and Hispanics compared to Whites among uninsured adults and Medicaid enrollees.
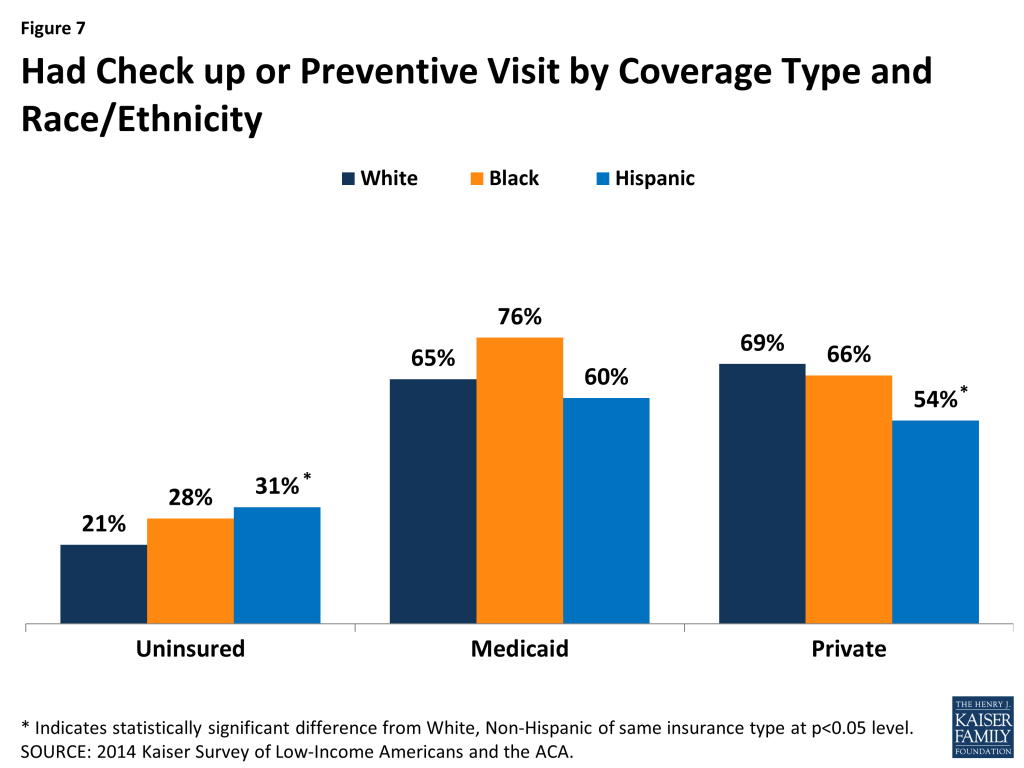
- Preventive services. Privately insured Hispanic adults are less likely than privately insured White adults to report a check-up or preventive visit (Figure 7). In contrast, among uninsured adults, Hispanics are more likely than Whites to have received preventive care. Among Medicaid enrollees, there are no significant differences in the likelihood of receiving preventive care when comparing Blacks and Hispanics to Whites.
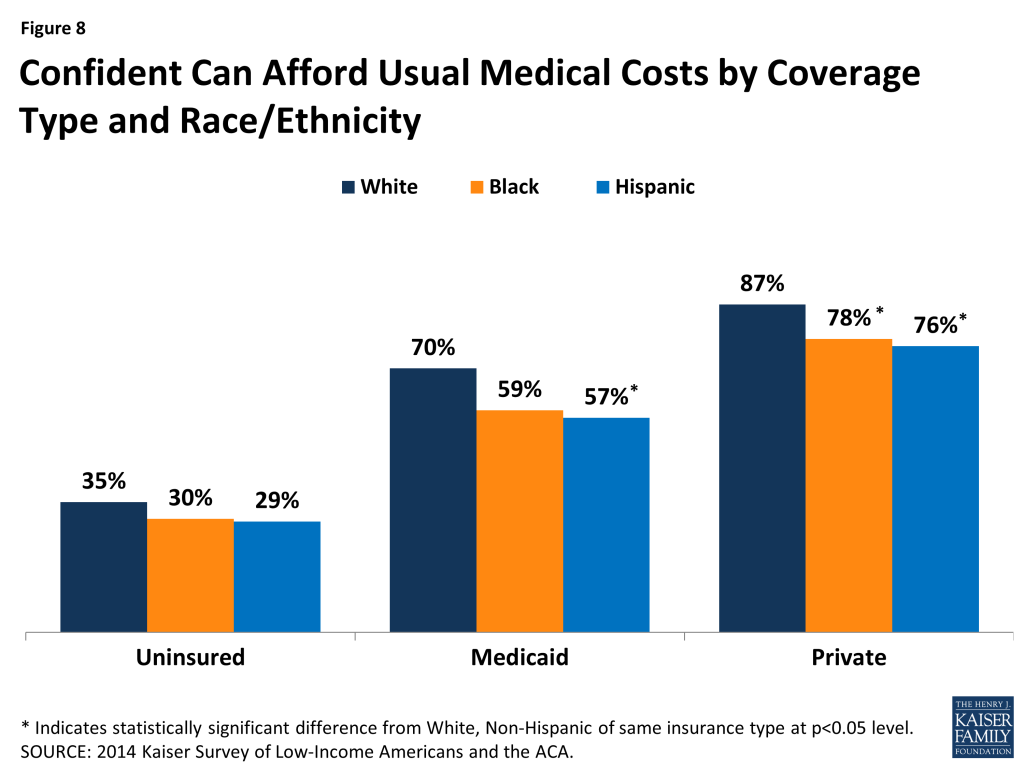
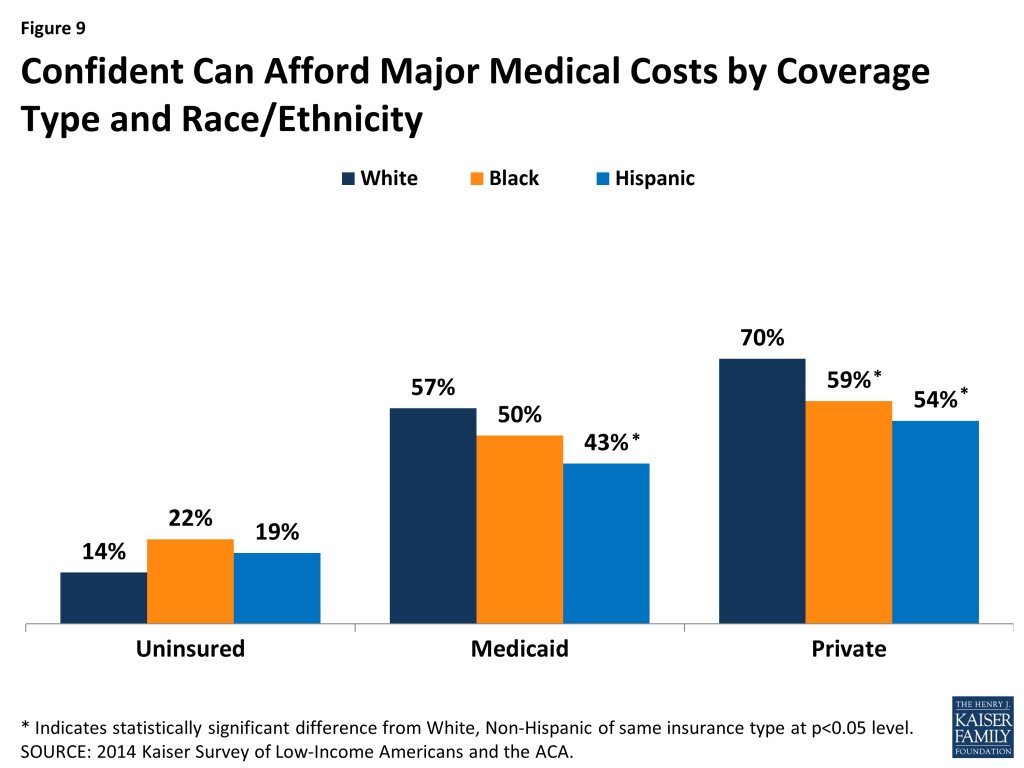
- Confidence in Ability to Afford Medical Costs. Among privately insured adults, Blacks and Hispanics are less likely than Whites to have confidence in their ability to afford both usual and major medical costs (Figures 8 and 9). Hispanic Medicaid enrollees also have less financial confidence compared to their White counterparts. Among uninsured adults, there are no significant differences for Blacks and Hispanics compared to Whites.
Discussion
In sum, these findings show that having health insurance improves access to and utilization of care for White, Black, and Hispanic adults. However, privately insured Blacks and Hispanics fare worse than privately insured Whites along several measures of access to and utilization of care and have less confidence in their ability to afford medical costs. Fewer differences are seen between Blacks and Hispanics compared to Whites among uninsured adults and Medicaid enrollees, and where there are differences, Blacks and Hispanics fare better relative to Whites in most cases (Table 3).
| Table 3: Differences in How Black and Hispanic Adults Fare Relative to Whites with Same Coverage Type for Selected Measures of Access, Utilization, and Financial Confidence | ||||||
| Uninsured | Medicaid Enrollees | Privately Insured | ||||
| Black compared to White | Hispanic compared to White | Black compared to White | Hispanic compared to White | Black compared to White | Hispanic compared to White | |
| Access to Care | ||||||
| Usual Source of Care | Worse | Worse | ||||
| Regular Provider | Worse | Worse | ||||
| Postponing/Going without Care | Better | Better | ||||
| Postponing/Going without Care Due to Cost | Better | Better | Better | |||
| Utilization of Care | ||||||
| Use of Medical Services | Worse | |||||
| Use of Preventive Services | Better | Worse | ||||
| Confidence in Ability to Afford Medical Costs | ||||||
| Usual Medical Costs | Worse | Worse | Worse | |||
| Major Medical Costs | Worse | Worse | Worse | |||
Among uninsured adults, Hispanics fare better than Whites on several measures of access and utilization, including being less likely to delay or forgo care and being more likely to receive preventive care. Black adults also are less likely than White adults to delay or forgo care due to cost. These differences may reflect uninsured Hispanics greater reliance on clinics for care relative to Whites, since clinics often have outreach and supportive services to connect patients to care. They also may reflect cultural differences in perceived need for care.
Among Medicaid enrollees, there are few differences in access to and utilization of care for Blacks and Hispanics compared to Whites. Hispanics are less likely than Whites to delay or forgo care, although no differences are observed among the share delaying or going without care due to cost. Hispanics have less confidence than Whites in their ability to afford usual and major medical costs. The small number of disparities observed among Medicaid enrollees may reflect the program’s role serving diverse and vulnerable low-income populations. Medicaid provides supportive services that can help connect individuals to care, such as transportation and case management. Moreover, Medicaid managed care plans and providers have significant experience serving diverse populations and may provide services designed to address their specific needs.
A greater number of differences are seen among privately insured adults, particularly for Hispanics compared to Whites. Among privately insured adults, Blacks and Hispanics are less likely to have a usual source of care and a regular provider and less likely to have confidence in the ability to afford usual and major medical costs. In addition, Hispanics are less likely than Whites to use medical services or receive preventive care. These differences may, in part, reflect the fact that Black and Hispanic privately insured adults have lower incomes than their White counterparts, although the findings suggest that other factors beyond cost are a substantial barrier to care for these adults.
Overall, the findings suggest that gains in health coverage under the ACA will likely lead to improvements in access to care and utilization across White, Black, and Hispanic adults. They also suggest that as the privately insured population becomes more diverse as a result of greater enrollment of people of color into private plans through the ACA Marketplaces, it will be important to focus attention on addressing racial and ethnic disparities in access to and utilization of care among privately insured adults. Reducing these disparities among privately insured adults will likely involve broad efforts by both insurers and providers to better address the specific linguistic, cultural, and social and environmental needs of diverse populations. Such efforts may build on lessons learned from Medicaid’s experience, given the program’s longstanding role serving a diverse population.
Appendix
Endnotes
- 2014 National HealthCare Quality and Disparities Report., Agency for Healthcare Research and Quality, available at http://www.ahrq.gov/research/findings/nhqrdr/nhqdr14/2014nhqdr.pdf ↩︎
- Smedley, B., Stith, A. and A. Nelson, “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care, Institute of Medicine of the National Academies, 2002, available at: http://iom.nationalacademies.org/Reports/2002/Unequal-Treatment-Confronting-Racial-and-Ethnic-Disparities-in-Health-Care.aspx ↩︎
- Cohen R. and M. Martinez, “Health Insurance Coverage: Early Release of Estimates from the National Health Interview Survey, 2014,” National Health Interview Survey Early Release Program, National Center for Health Statistics, Centers for Disease Control and Prevention, June 2015, available at: http://www.cdc.gov/nchs/data/nhis/earlyrelease/insur201506.pdf ↩︎
- Smedley, B., op cit. ↩︎
- Call K, McAlpine D, Garcia C, 2014. “Barriers to Care in an Ethnically Diverse Publicly Insured Population.” Medical Care 52(8) 720-727. ↩︎