What Is the Scope of the Mexico City Policy: Assessing Abortion Laws in Countries That Receive U.S. Global Health Assistance
Key Facts
- On January 23, 2017, President Trump reinstated and expanded the Mexico City Policy requiring foreign NGOs to certify that they will not “perform or actively promote abortion as a method of family planning,” using any funds (including non-U.S. funds), as a condition for receiving U.S. government global health assistance. The U.S. government issued initial guidance related to U.S. global family planning assistance on March 2, and further guidance on other U.S. global health assistance is expected soon.
- This data note assesses how the Mexico City Policy affects the provision of legal abortion services in U.S. assisted countries.
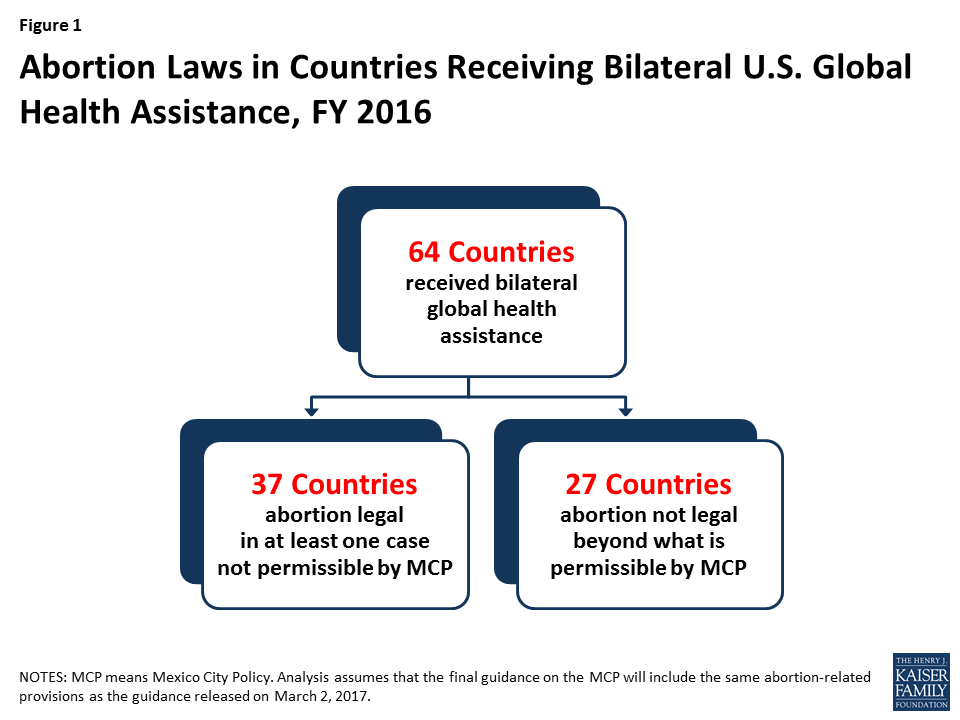
- It finds that the majority of countries that received U.S. bilateral global health assistance in FY 2016 (37 of 64), allow for legal abortion in at least one case not permissible by the MCP. These countries accounted for 53% of bilateral global health assistance. In all other countries, abortion is not legal beyond what is permissible by the MCP, although other activities are prohibited by the policy.
- While foreign NGO recipients of U.S. global health assistance will be required to certify that they are in compliance with the MCP regardless of where they work, where countries’ laws allow for abortion in cases not permitted by the MCP, they will be prohibited from providing legal services with non-U.S. funds as a condition of receiving U.S. assistance.
Introduction
On January 23, 2017, President Trump reinstated and expanded the Mexico City Policy (MCP).1 The MCP, first instituted by President Reagan in 1984 and rescinded and reinstated by Presidents along party lines since, requires foreign NGOs to certify that they will not “perform or actively promote abortion as a method of family planning,” using non-U.S. funds (including private funding), as a condition for receiving U.S. government global family planning assistance and, as expanded by President Trump, “global health assistance furnished by all departments or agencies”2 (see KFF explainer and Table 1). On March 2, the U.S. government took the first step in implementing the reinstated policy by issuing guidance on its application to family planning assistance;3 further guidance on other U.S. global health assistance is expected soon. This analysis assumes that the final guidance will include the same abortion-related provisions as the guidance released on March 2. One metric for gauging impact of the MCP is assessing the abortion laws in countries that receive bilateral U.S. global health assistance. This data note provides an assessment of the legal landscape to identify how the MCP affects the provision of legal abortion services by foreign NGOs.
The Mexico City Policy requires foreign NGOs to certify, as a condition of receiving U.S. global health assistance, that they will not “perform or actively promote abortion as a method of family planning” with any funds, including non-U.S. funds. The following definitions apply:5 ABORTION IS A METHOD OF FAMILY PLANNING WHEN used for the purpose of spacing births (including, for example, abortion to preserve a woman’s physical or mental health). TO PERFORM ABORTION means to operate a facility where abortions are performed as a method of family planning. TO ACTIVELY PROMOTE ABORTION means for an organization to commit resources to increase the availability or use of abortion as a method of family planning by:
- operating a family planning counseling service that provides advice and information regarding the benefits and availability of abortion as a method of family planning;
- providing advice that abortion is an available option in the event that other methods of family planning are not used or are not successful or encouraging women to consider abortion;
- lobbying a foreign government to legalize (or continue legality of) or make available abortion as a method of family planning; and
- conducting a public information campaign regarding the benefits and/or availability of abortion as a method of family planning.
Excluded from these definitions are the following EXCEPTIONS (allowable activities):
- abortion in cases where the pregnancy either poses a risk to a woman’s life or is the result of incest or rape;[endnote 215568-12]
- treatment of injuries or illnesses caused by legal or illegal abortions (e.g., post-abortion care); and
- responding to a question regarding where a safe, legal abortion may be obtained if the question is specifically asked by a woman who is already pregnant, she clearly states that she has already decided to have a legal abortion, and the family planning counselor reasonably believes that the ethics of the medical profession in the country requires a response regarding where it may be obtained safely.
Analysis
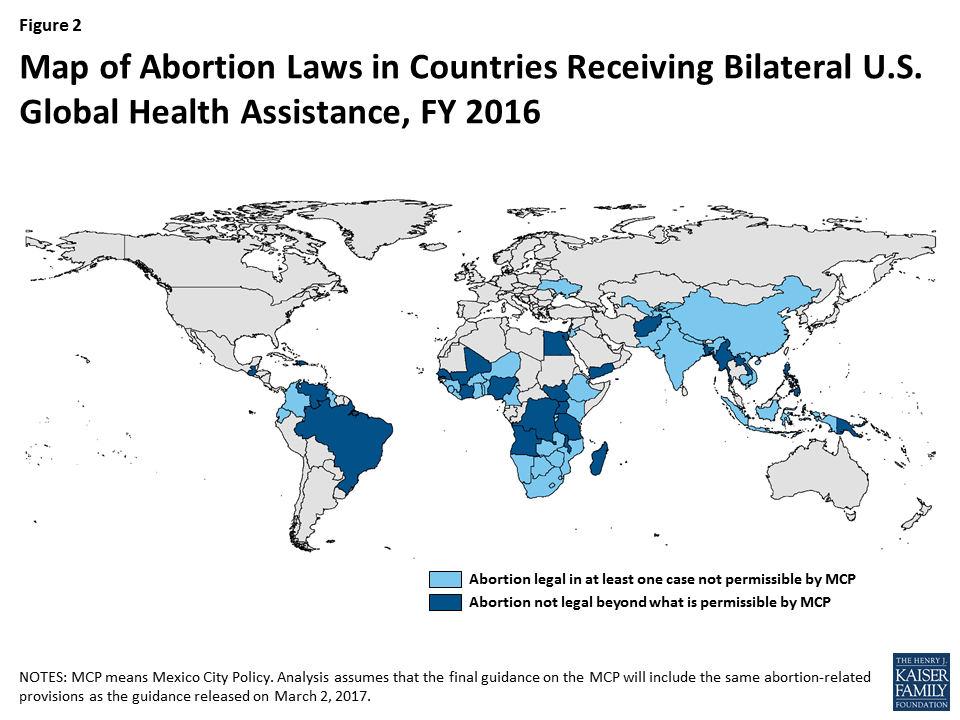
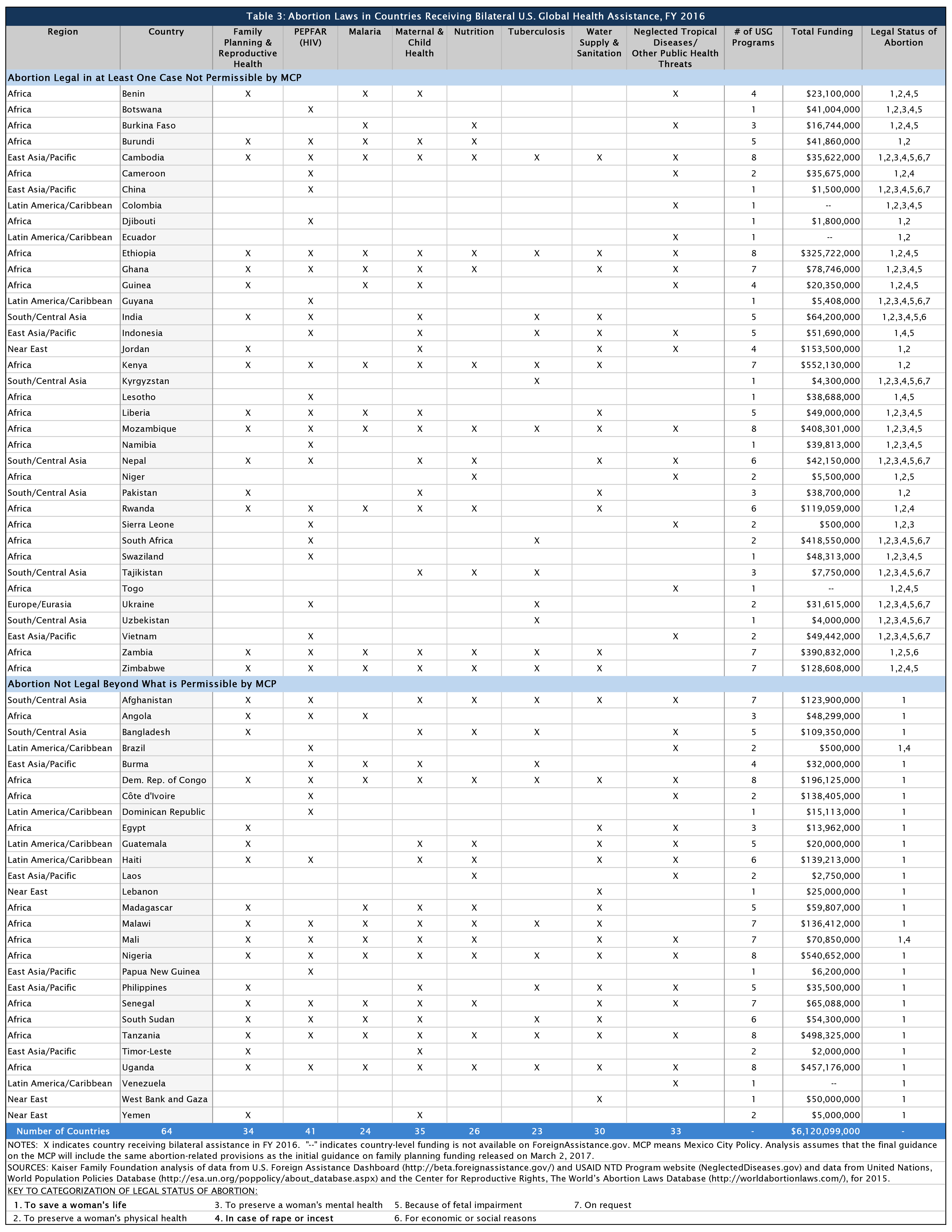
To assess how the MCP would likely affect the provision of legal abortion services in U.S.-assisted countries, we first identified all countries that received bilateral U.S. global health assistance in FY 2016.6 We then looked at the abortion laws in these countries.7 Specifically, we assessed whether abortion was legal in any of the following circumstances: threats to a woman’s life; to preserve a woman’s health; to preserve a woman’s mental health; in the case of rape or incest; because of fetal impairment; for economic or social reasons; and/or on request. We next categorized countries into two groups based on their abortion laws: (1) those that allow for legal abortion in at least one case not permissible under the Mexico City Policy and (2) those that do not allow for legal abortion in any case other than the MCP exceptions (or in fewer cases than the exceptions). We include analysis by the eight major global health program areas supported by the U.S. government: family planning and reproductive health (FP/RH), PEPFAR (HIV), malaria, maternal and child health (MCH), nutrition, tuberculosis (TB), water supply/sanitation, and neglected tropical diseases (NTDs)/other public health threats. The results are as follows (see Figures 1 & 2):
- In FY16, the U.S. provided bilateral global health assistance to 64 countries. More than half (34) were countries in Africa. The next largest region was East Asia and the Pacific (9). Funding for PEPFAR was directed to the greatest number of countries (41), followed by MCH (35) and FP/RH (34). Together, bilateral global health assistance in these 64 countries totaled just over $6.1 billion in FY16.8
- Among these 64 countries, 37 allow for legal abortion in at least one case not permissible under the MCP.9 Most (22) were in Africa; the next largest region was South/Central Asia (6). In nearly all of these countries (35), abortion is legal to preserve a woman’s physical health. In 28 countries, abortion is legal in the case of fetal impairment. PEPFAR reached the greatest number of countries (25) in this group, followed by MCH (18), NTDs/other public health threats (17), and FP/RH (16) (see Tables 2 & 3). Together, these 37 countries accounted for 53% of bilateral global health assistance in FY16.
- In 27 countries, abortion is not legal in any case beyond the MCP exceptions. Almost half of these countries were in Africa (12), followed by Latin America/Caribbean (5) and East Asia and the Pacific (5). Most of these countries (25) have abortion laws that are more restrictive than the MCP, allowing abortion only to save a woman’s life; only 2 also allow abortion in the cases of rape or incest. FP/RH reached the greatest number of countries (18) in this group, followed by MCH (17), PEPFAR (16), water supply/sanitation (16), and NTDs/other public health threats (16) (see Tables 2 & 3). Together, these 27 countries accounted for 47% of U.S. bilateral global health assistance in FY16.
- The MCP affects these two groups of countries differently. Where a country’s laws allow for abortion in cases not permissible under the MCP, foreign NGOs would be prohibited from providing legal services with non-U.S. funds as a condition of receiving U.S. global health assistance. Where a country’s laws do not allow for abortion beyond what is permissible by the MCP, the policy would not curtail legal abortion services, although it would still prohibit other activities, such as providing counseling about abortion as a method of family planning (see Table 1). In all cases, foreign NGO recipients of U.S. global health assistance will be required to certify that they are in compliance with the MCP.10 In addition, any U.S. NGO recipient of global health assistance who in turn provides a sub-award to a foreign NGO will be required to ensure that the foreign NGO certified its compliance with MCP.
| Table 2: Abortion Laws in Countries Receiving Bilateral U.S. Global Health Assistance, by Program Area, FY 201611 | ||
| Program Area | Abortion Legal in at Least One Case Not Permissible by MCP (# of Countries) | Abortion Not Legal Beyond What Is Permissible by MCP (# of Countries) |
| FP/RH | 16 | 18 |
| PEPFAR (HIV) | 25 | 16 |
| Malaria | 13 | 11 |
| MCH | 18 | 17 |
| Nutrition | 13 | 13 |
| TB | 13 | 10 |
| Water Supply & Sanitation | 14 | 16 |
| NTDs/Other Public Health Threats | 17 | 16 |
| NOTES: MCP means Mexico City Policy. FP/RH means family planning/reproductive health. MCH means maternal and child health. TB means tuberculosis. NTDs means neglected tropical diseases. Analysis assumes that the final guidance on the MCP will include the same abortion-related provisions as the guidance released on March 2, 2017. | ||
- White House, “The Mexico City Policy,” Memorandum for the Secretary of State, the Secretary of Health and Human Services, the Administrator of the Agency for International Development, Jan. 23, 2017, https://www.whitehouse.gov/the-press-office/2017/01/23/presidential-memorandum-regarding-mexico-city-policy. ↩︎
- “Policy Statement of the United States of America at the United Nations International Conference on Population (Second Session), Mexico City, Mexico, August 6-14, 1984,” undated; Bill Clinton Administration, “Subject: AID Family Planning Grants/Mexico City Policy,” Memorandum for the Acting Administrator of the Agency for International Development, January 22, 1993, National Archives and Records Administration’s Clinton Presidential Materials Project, https://clinton6.nara.gov/1993/01/1993-01-22-aid-family-planning-grants-mexico-city-policy.html; FY 2000 Consolidated Appropriations Act, P.L. 106-113; George W. Bush Administration, “Subject: Restoration of the Mexico City Policy,” Memorandum for the Administrator of the United States Agency for International Development, January 22, 2001, Bush Administration White House Archives, https://georgewbush-whitehouse.archives.gov/news/releases/20010123-5.html; “Subject: Restoration of the Mexico City Policy,” Memorandum for the Administrator of the United States Agency for International Development, March 28, 2001, Federal Register, https://www.federalregister.gov/documents/2001/03/29/01-8011/restoration-of-the-mexico-city-policy; George W. Bush Administration, “Subject: Assistance for Voluntary Population Planning,” Memorandum for the Secretary of State, August 29, 2003, Bush Administration White House Archives, http://georgewbush-whitehouse.archives.gov/news/releases/2003/08/20030829-3.html; Barack Obama Administration, “Mexico City Policy and Assistance for Voluntary Population Planning,” Memorandum for the Secretary of State, the Administrator of the United States Agency for International Development, January 23, 2009, https://www.whitehouse.gov/the-press-office/mexico-city-policy-and-assistance-voluntary-population-planning; White House, “The Mexico City Policy,” Memorandum for the Secretary of State, the Secretary of Health and Human Services, the Administrator of the Agency for International Development, Jan. 23, 2017, https://www.whitehouse.gov/the-press-office/2017/01/23/presidential-memorandum-regarding-mexico-city-policy. ↩︎
- USAID, “Standard Provisions for U.S. Nongovernmental Organizations: A Mandatory Reference for ADS Chapter 303,” ADS Reference 303maa, partial revision March 2, 2017, https://www.usaid.gov/ads/policy/300/303maa; USAID, “Standard Provisions for Non-U.S. Nongovernmental Organizations: A Mandatory Reference for ADS Chapter 303,” ADS Reference 303mab, partial revision March 2, 2017, https://www.usaid.gov/ads/policy/300/303mab. ↩︎
- USAID, “Standard Provisions for U.S. Nongovernmental Organizations: A Mandatory Reference for ADS Chapter 303,” ADS Reference 303maa, partial revision March 2, 2017, https://www.usaid.gov/ads/policy/300/303maa; USAID, “Standard Provisions for Non-U.S. Nongovernmental Organizations: A Mandatory Reference for ADS Chapter 303,” ADS Reference 303mab, partial revision March 2, 2017, https://www.usaid.gov/ads/policy/300/303mab. ↩︎
- Assumes that the final guidance on the MCP will include the same abortion-related provisions as the guidance released on March 2. ↩︎
- Kaiser Family Foundation analysis of data from the U.S. Foreign Assistance Dashboard (http://beta.foreignassistance.gov/) and USAID NTD Program website (NeglectedDiseases.gov). The U.S. Foreign Assistance Dashboard includes global health funding provided to countries by USAID and the Department of State only, but not funding provided by the CDC. Our analysis includes all bilateral global health assistance provided to countries but not assistance designated as regional or worldwide, which may in turn be provided to countries but is not identifiable by country (estimated to be approximately $1.1 billion in FY16). It also does not include global health assistance provided to multilateral institutions, such as the Global Fund to Fight AIDS, Tuberculosis and Malaria, GAVI, and others, which totaled approximately $2 billion in FY16, and are expected to be exempt from MCP requirements. ↩︎
- Kaiser Family Foundation analysis of data from the United Nations, World Population Policies Database (http://esa.un.org/poppolicy/about_database.aspx), and the Center for Reproductive Rights, The World’s Abortion Laws Database (http://worldabortionlaws.com/), for 2015. ↩︎
- FY16 funding amount does not include $100 million that was provided for NTDs, which is not identifiable by country. ↩︎
- These 37 countries include 9 countries that, while allowing for legal abortion in at least one case not permitted by the MCP, do not allow abortion in all MCP excepted cases (e.g., allow abortion to preserve a woman’s physical health but not in the cases of rape or incest). ↩︎
- While all foreign NGOs will be required to certify that they are in compliance with the MCP, not all foreign NGOs provide services that are prohibited by the MCP. Such an assessment was beyond the scope of this analysis. ↩︎
- Kaiser Family Foundation analysis of data from the U.S. Foreign Assistance Dashboard (http://beta.foreignassistance.gov/) and USAID NTD Program website (NeglectedDiseases.gov) and data from the United Nations, World Population Policies Database (http://esa.un.org/poppolicy/about_database.aspx), and the Center for Reproductive Rights, The World’s Abortion Laws Database (http://worldabortionlaws.com/), for 2015. ↩︎