Almost all women use contraception at some point in their life and approximately two-thirds of women of reproductive age currently use contraception.1 Most, but not all, sources of public and private health insurance coverage now pay for contraceptive services and supplies, but the extent of coverage differs by payer. This fact sheet reviews how coverage of contraceptives varies between private insurance and publicly funded programs including Medicaid, Medicare, TRICARE, the Indian Health Service, and Title X funded clinics.
Private Insurance
Private insurance plans include employer-sponsored insurance (ESI) plans in the large and small group markets, plans purchased directly from an insurance company by an individual, and plans purchased through state and federal Marketplaces. A majority (65%) of women ages 15-49 are insured through private plans either as the primary beneficiary or as a spouse or dependent.2 The Affordable Care Act (ACA) creates the first federal contraceptive coverage requirement for private plans. While they apply to most private plans, they do not apply to all insurers.3 A recent HHS study estimates that 55 million women have private insurance coverage that includes no-cost coverage for contraceptive services and supplies.4
- Employer-Sponsored Insurance: As of August 2012, the ACA requires most private insurance plans, including self-funded plans, to cover at least one of each of the 18 FDA approved methods of contraception for women, as prescribed (Table 1). These insurance plans are also required to cover related contraceptive services without cost-sharing, which includes contraceptive counseling, the insertion and removal of a medical device, and follow-up visits. Insurance plans that have not substantially changed the benefits offered and existed before March 23, 2010 are considered “grandfathered” and are exempt.
- The Individual Insurance Market: Individual insurance plans, including those available through the ACA Marketplaces, are required to meet minimum essential coverage, which includes the 18 FDA approved contraceptive methods and related services.
- Religious Employers: Individuals who receive their health insurance through a religious employer may not receive full coverage for contraception.
- Religious institutions defined as “houses of worship” are exempt from the contraceptive coverage requirement and its employees are not entitled to contraceptive coverage.5
- Religiously affiliated nonprofit employers, such as universities and religious charities, and closely held for profit employers that object to contraceptive coverage on religious grounds can receive an accommodation to the contraceptive coverage requirement. Employees and dependents are entitled to contraceptive coverage and receive coverage directly from the insurer or third-party administrator.
- Over the Counter (OTC) Contraception: In recent years, there have been proposals to make oral contraceptives available over the counter to expand women’s access to contraception. Currently, only some forms of emergency contraception are available OTC. In order for a contraceptive to be available OTC, the manufacturer needs FDA approval for dispensation without a prescription. Recently, there have been several Congressional proposals to simplify the FDA approval process in the case of oral contraceptives.6 There is also growing activity at the state level to allow pharmacists prescribe and to dispense oral contraceptives without requiring a doctor’s visit.7
| Table 1: Minimum Contraceptive Coverage Requirements in Private Plans | ||
| Contraceptive Method | Products/Options | Must Cover |
| Surgical sterilization | Also called tubal ligation | √ |
| Implant sterilization | Only Essure available | √ |
| Implantable Rod | Multiple | √ at least 1 |
| IUD – Copper | Only ParaGard available | √ |
| IUD – Progestin | Multiple | √ at least 1 |
| Injection | Multiple | √ at least 1 (may be generic) |
| Oral contraceptives – combined | Multiple | √ at least 1 (may be generic) |
| Oral Contraceptives – progestin only | Multiple | √ at least 1 (may be generic) |
| Oral Contraceptives – extended/continuous use | Multiple | √ at least 1 (may be generic) |
| Patch | Multiple** | √ at least 1 (may be generic) |
| Vaginal Ring | Only NuvaRing available | √ |
| Diaphragm with Spermicide | Only Milex Omniflex available | √ |
| Sponge with Spermicide | Only Today Sponge available | √* |
| Cervical Cap with Spermicide | Only FemCap available | √ |
| Female Condom | Multiple | √* |
| Spermicide alone | Multiple | √ at least 1 (may be generic)* |
| Emergency Contraception-Progestin | Multiple | √ at least 1 (may be generic)* |
| Emergency Contraception- Ulipristal Acetate | Only ella available | √ |
| *Approved for sale over-the-counter but only covered at no cost with a prescription. **The manufacturer of the brand name (OrthoEvra) patch has discontinued production and the generic alternative will be the only patch available. SOURCE: FDA Birth Control Guide and Departments of Labor, Health and Human Services, and Treasury, FAQs about Affordable Care Act Implementation (Part XXVI). |
||
Medicaid
Medicaid is a state-federal program that provides health coverage to individuals with low incomes. The ACA enables states to expand Medicaid eligibility levels to encompass a broader population than has historically been eligible, but only half of states (29 + DC) have expanded their program. Among the 19.4 million women ages 15 and older with full Medicaid benefits in 2011, those in their reproductive years (ages 15 to 49) accounted for 70% of enrollment nationwide (Figure 1).8 All Medicaid programs are required to cover family planning services and supplies without cost-sharing. Medicaid beneficiaries are able to seek family planning services from any provider that accepts Medicaid, regardless if the provider is included in the beneficiary’s network.9 This is particularly important for women enrolled in Medicaid managed care plans or for women who are concerned about confidentiality. Because there is no federally defined standard for family planning, the range of contraceptive products and services that are covered can vary by state and differ depending on how an individual qualifies for Medicaid.
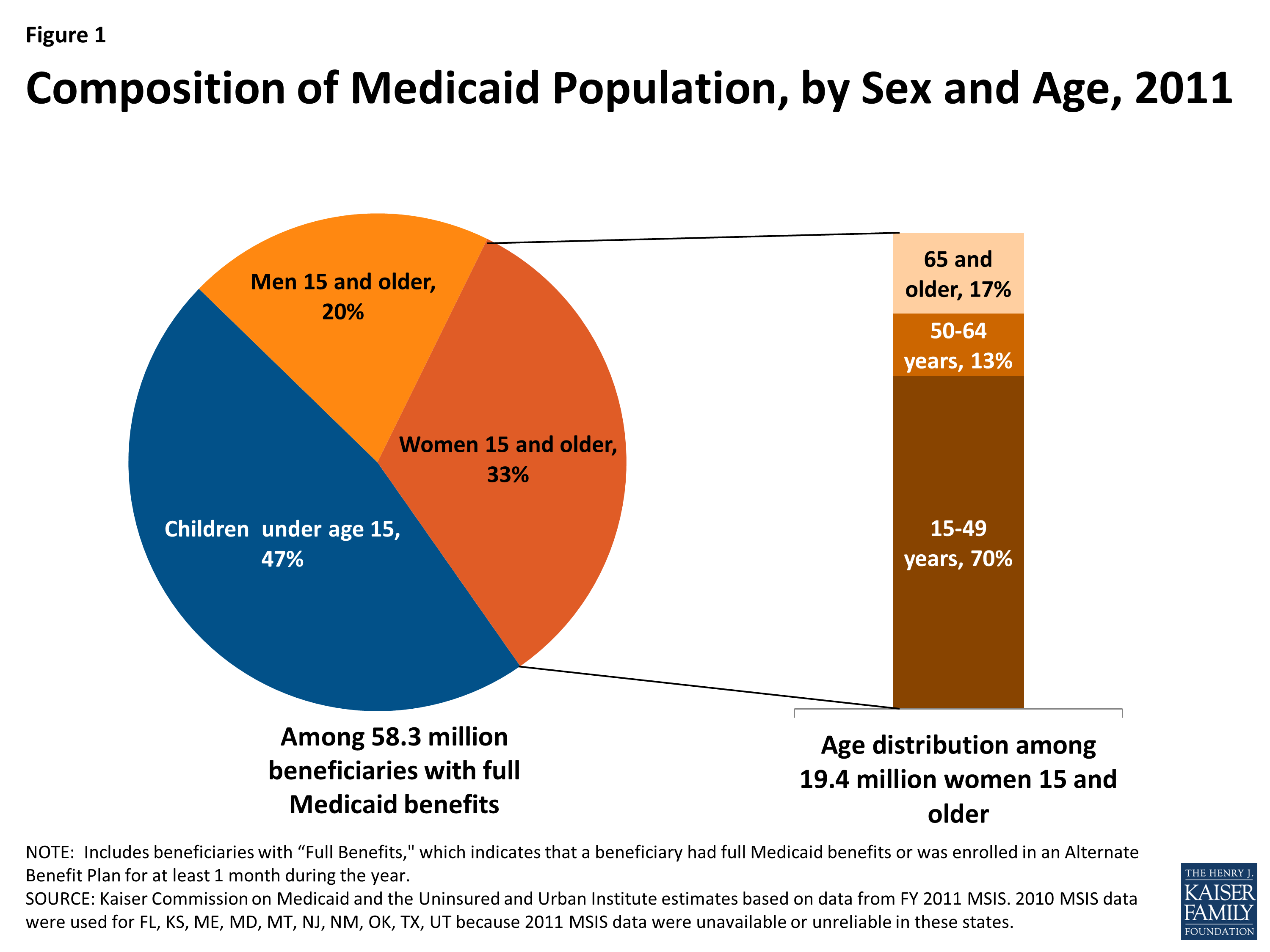
Figure 1: Composition of Medicaid Population, by Sex and Age, 2011
- Traditional Medicaid: Historically, the Medicaid eligibility pathways for women included being very low income and meeting one of the categorical eligibility criteria of being pregnant, a parent of a dependent child under 18, disabled or elderly. All individuals who qualify for traditional Medicaid programs are covered for family planning services and supplies without cost-sharing, but states have the flexibility to determine which services are included. All state Medicaid programs receive an enhanced 90% federal matching payment for family planning services, meaning states are only responsible for 10% of the cost of the service.10
- Medicaid Expansion: The ACA gives states the option of eliminating the historical categorical requirements and expanding Medicaid to all residents with incomes below 138% of the Federal Poverty Level. Individuals who are newly covered as a result of the ACA Medicaid coverage expansion are entitled to the same contraceptive coverage as enrollees in new private plans discussed above, meaning at least one type of all 18 FDA approved methods of contraception are covered without cost-sharing. Depending on state coverage decisions, however, the range of contraceptives available to this expansion group may differ from those who qualify through traditional Medicaid pathways.
- Medicaid Family Planning Expansion Programs: Many states have also established limited scope Medicaid funded programs to extend access to family planning programs to women who either are uninsured, do not qualify for traditional Medicaid or Medicaid expansion, or may have coverage that does not fully cover contraceptives. Just over half of states (29 states) have established these programs through either Medicaid State Family Planning Waivers or State Plan Amendments (SPAs).11,12 In 2011, at least 3.5 million women ages 15 to 49 obtained Medicaid-covered family planning services through family planning waivers.13 States with family planning expansion have flexibility to determine the contraceptive methods and related services that are covered.
- Sterilization: Medicaid covers sterilization procedures; however, federal law requires a 30-day waiting period between when a mentally competent woman (age 21 or older) signs a consent form and the procedure.14 This policy was established as a protection against the eugenic sterilization of low-income women, women with disabilities and women of color. It may have the untended effect of impeding access to sterilization, particularly for women seeking to have the procedure done during the post-partum hospital stay.15 This requirement also applies to all federal programs including TRICARE, the Indian Health Service and Title X and discussed below.
Medicare
Medicare is the federal program that provides health insurance to people ages 65 and older, as well as to younger people with permanent disabilities and end-stage renal disease (ESRD). Although the majority of Medicare beneficiaries are ages 65 and older, almost 920,000 women ages 18 to 44 received insurance coverage through Medicare in 2011 (Figure 2). Contraception is an often over-looked aspect of care for women with chronic conditions and disabilities16 and there is no federal requirement for Medicare to cover contraceptive services and supplies for women of reproductive age enrolled in Medicare.17
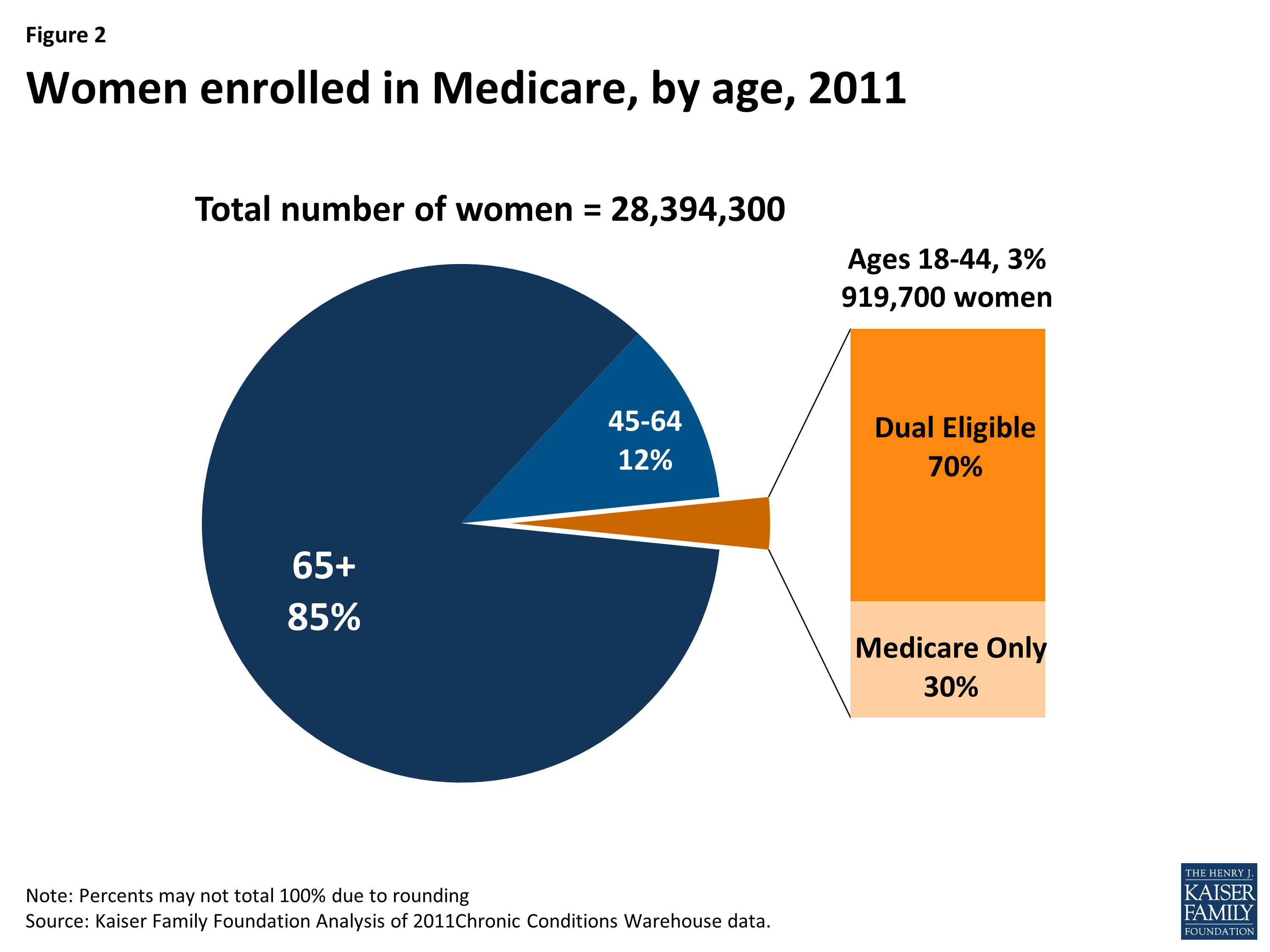
Figure 2: Women enrolled in Medicare, by age, 2011
- Part D and Medicare Advantage: Although there is no requirement that Medicare cover contraceptives, certain hormonal contraceptives may be covered under Part D, Medicare’s voluntary outpatient prescription drug benefit18 or included as a benefit for beneficiaries enrolled in Medicare Advantage (also known as Medicare Part C), a program that allows beneficiaries to enroll in private health plans (such as an HMO or PPO) to receive all Medicare-covered benefits. The majority of Medicare Advantage plans also provide Part D prescription drug coverage and offer additional benefits beyond what is covered under traditional Medicare, which could include coverage of contraceptive services and supplies. The extent and level of coverage for contraceptives can depend on the specific plan an enrollee selects under Part D and Medicare Advantage.
- Sterilization: Medicare only covers surgical sterilization for women when the procedure is a necessary part of treatment of an illness or injury.19 Elective sterilizations are not covered, even if the physician believes pregnancy would endanger the overall health of the woman.
- Dual Eligible Women: Among women on Medicare who are of childbearing age, 70% were dually eligible for Medicare and Medicaid, meaning they were very low-income. While Medicare is the primary payer for dual eligibles, Medicaid can cover cost-sharing, deductibles and monthly premiums, as well as services that are not covered by Medicare, like contraceptives.20 However, enrollees can only get Medicaid coverage after Medicare denies the service, which can create a time delay for women seeking access to affordable contraceptives and put them at higher risk of unintended pregnancy.
TRICARE
TRICARE provides health insurance coverage for more than 200,000 women in the military, as well as 1.1 million female spouses and dependents of active duty military personnel who are of childbearing age. More than 95% of women serving in the military are of reproductive age.21 Coverage decisions are made by the Department of Defense; the ACA contraceptive coverage requirements are not applicable to TRICARE.22
- Scope of coverage: TRICARE covers many contraceptive methods and related services.23 Oral contraceptives, diaphragms, intrauterine devices, emergency contraception, and surgical sterilization are covered when prescribed. TRICARE does not cover condoms or nonprescription spermicidal foams, jellies, or sprays. Although not required, some TRICARE insurance plans also cover contraceptive injections and the vaginal ring.24
- Cost sharing: TRICARE enrollees have coverage for prescription contraceptives without cost sharing, when prescriptions are filled at a military facility, while prescriptions obtained outside of these facilities may be subject to cost-sharing.
- Reforms: In recent years, legislation has been introduced in Congress to give female service members and female dependents coverage for the full range of contraceptive methods without cost sharing, mirroring the ACA private plans contraceptive coverage requirements.25
The Indian Health Service (IHS)
The IHS is the health care system for federally recognized American Indian and Alaska Natives in the United States.26 Services are provided to more than 2.2 million27 American Indians and Alaska Natives without cost sharing through facilities and clinics operated by IHS on or near Indian reservations.28 Federal regulations require IHS to cover health promotion and disease prevention services, which include family planning and treatment of STIs; however availability of these services can vary by clinic.
- Covered Methods: Contraceptives available to women insured through IHS are listed on the National Core Formulary, the list of drugs and devices covered by the program.29 The Copper and hormonal IUD, Depo-Provera injection, implants, emergency contraception, the vaginal ring, the patch, and oral contraceptives are all included in the formulary.
- Availability and Access: Availability of contraceptive methods varies by clinic. Recent surveys have found emergency contraception is inconsistently stocked at IHS pharmacies, and a commercial pharmacy may be geographically unreachable for many women living in rural communities.30,31
Title X
Title X is a federal block grant provided to family planning clinics by the US Department of Health and Human Services’ Office of Population Affairs. More than 4,400 clinics receiving Title X National Family Planning Program funding serve approximately 5 million clients each year, 92% of whom are female.32 Low-income women are able to seek contraceptive services from Title X funded clinics at reduced or no- cost. 33
- Participating providers: Clinics that receive Title X funds include state, county, and local health departments; community health centers; Planned Parenthoods; as well as hospital-based, school-based, faith-based, other private nonprofits.34 Clinics that receive funds must follow service delivery standards, including that a broad range of contraceptive methods be available, and that the services are voluntary and confidential.
- Eligibility: Women with incomes below 100% of the federal poverty level are entitled to receive services without cost, although Title X clinics may charge a third party insurer such as Medicaid. Those with incomes between 101% and 250% of the federal poverty level are charged on a sliding scale, based on ability to pay. Clinics are required to charge women with incomes above 250% of the federal poverty level an amount to recover the reasonable cost of providing services.
***
Private and public coverage of contraceptive services and supplies varies greatly. While most women with private insurance now have comprehensive coverage without cost-sharing, women insured through public programs or who are uninsured lack the same guarantee. The patchwork of policies used by public insurance programs can leave some women vulnerable to gaps in contraceptive coverage or shouldering significant costs for birth control. Although legislative efforts at the federal and state levels have closed some of these gaps, affordable access to the full range of available comprehensive options is still not within the reach of all women in the U.S.
Endnotes
Guttmacher Institute. (2010). Facts on Contraceptive Use in the United States.
Kaiser Family Foundation. (2014). Women’s Health Insurance Coverage.
This fact sheet addresses federal law for contraceptive coverage. Effective January 2016, a new California law requires plans to cover more contraceptives than the ACA requires. The law specifies that a plan does not have to cover more than one therapeutic equivalent of a contraceptive drug, device, or product, as long as at least one is covered without cost-sharing. Contraceptives with the same chemical formulation and delivery mechanism are therapeutically equivalent.
ASPE. (2015). Data Point: The Affordable Care Act is Improving Access to Preventive Services for Millions of Americans.
Kaiser Family Foundation. (2013). A Guide to the Supreme Court's Review of the Contraceptive Coverage Requirement.
S.1438 - Allowing Greater Access to Safe and Effective Contraception Act; and Affordability Is Access Act (AAA)
California Legislative Information, 20113-2014, SB 493- Pharmacy Practice. Oregon House Bill 2879
Kaiser Family Foundation. (2015). Medicaid and Family Planning: Background and Implications of the ACA.
National Health Law Program, et al. (2015). Intrauterine Devices and Implants: A Guide to Reimbursement.
Kaiser Family Foundation. (2015). Medicaid and Family Planning: Background and Implications of the ACA.
Kaiser Family Foundation. (2014). States that Have Expanded Eligibility for Coverage of Family Planning Services Under Medicaid.
State plan amendments provide family planning services, including contraception, to women who are uninsured or underinsured, but who do not qualify for Medicaid and 1115 waivers may use other eligibility criteria.
KCMU and Urban Institute estimates based on data from FY 2011 MSIS.
Sterilization of Persons in Federally Assisted Family Planning Projects, 42 CFR §50.201.
American College of Obstetricians and Gynecologists Committee on Healthcare for Underserved Women. (2012). Committee Opinion: Access to Postpartum Sterilization, Obstetrics and Gynecology.
Kaplan, C. (2006). Special Issues in Contraception: Caring for Women with Disabilities. Journal of Midwifery and Women’s Health 51(6): 450-456.
Institute of Medicine. (2011). Clinical Preventive Services for Women: Closing the Gaps.
Noridian Healthcare Solutions. (May 5, 2015). Medicare Coverage Articles: IUD (Hormone-Eluting) for Endometrial Hyperplasia- CPT 58999.
Centers for Medicare & Medicaid Services. National Coverage Determination for Sterilization (230.3).
Kaiser Family Foundation. (2013). Medicaid's Role of Dual Eligible Beneficiaries.
Center for American Progress. (2015). Access to Contraception for Women Serving in the Armed Forces.
National Women’s Law Center. (2015). Women who rely on the Military for Health Care Deserve Comprehensive Birth Control Coverage and Counseling: Support the Access to Contraception for Women Service members and Dependents Act.
TRICARE, Covered Services - Birth Control.
HealthNet Federal Services: TRICARE, Birth Control.
Access to Contraception for Women Servicemembers and Dependents Act of 2015 (House) H.R. 742 (2015).
Indian Health Service, Eligibility.
Kaiser Family Foundation. (2013). Health Coverage and Care for American Indians and Alaska Natives.
Institute of Medicine. (2011). Clinical Preventive Services for Women: Closing the Gaps.
Indian Health Service. (2015). IHS National Core Formulary.
Office of Senator Barbara Boxer. (March 11, 2015). Boxer, Colleagues urge HHS Secretary Sylvia Burwell to Improve Access to Emergency Contraception at Indian Health Services Facilities.
Native American Women’s Health Education Resource Center. (2014). Plan B/ Emergency Contraceptive Report Card for Indian Health Service Facilities of Great Plains Area, Albuquerque, Navajo, Oklahoma and Bemidji Areas.
Office of Population Affairs, Title X Family Planning.
Department of Health and Human Services, Office of Population Affairs. (2014). Program Requirements for Title X Funded Family Planning Projects.
Office of Population Affairs, Title X Family Planning.