Dobbs-era Abortion Bans and Restrictions: Early Insights about Implications for Pregnancy Loss
Key Takeaways
- Abortion bans can limit care for those who are experiencing a miscarriage or stillbirth. The medical interventions used to manage pregnancy losses are often the same medicines and procedures used in abortions.
- While all state bans have exceptions for cases of life endangerment of the pregnant person, they do not necessarily account for the wide range of circumstances people may face when experiencing a pregnancy loss. This has resulted in several cases of women experiencing health threatening situations with imminent fetal demise or in early stage of pregnancy loss, yet being unable to obtain medical treatment until their health declined to the point where their lives were on the line.
- Clinicians practicing in states that ban abortion report that the restrictions are worsening their ability to practice within the standard of care, manage miscarriages and pregnancy related emergencies, and having a negative impact on patient-provider relationships.
- When severe or fatal fetal anomalies are detected during pregnancy and loss is inevitable or highly likely, people in states with bans may not have the option to terminate the pregnancy.
- Laws that grant “fetal personhood” can deter pregnant people, particularly some people of color, from seeking care during a pregnancy loss because a miscarriage may be conflated with a self-managed abortion, risking criminalization for pregnancy loss.
Introduction
Since the Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization in 2022, 14 states now ban the provision of abortion and several more limit abortion up to gestational limits very early in pregnancy. However, the impact of these bans and restrictions is not limited to abortions. Abortion bans and gestational restrictions also restrict care for people experiencing loss of a pregnancy – either miscarriage or stillbirth – since many of the medical treatments for pregnancy loss are the same medications and procedures used for abortion care. For many people experiencing a miscarriage or stillbirth, the loss of the pregnancy is a physically, mentally, and emotionally taxing experience. While some people experiencing a pregnancy loss do not require medical intervention, some do, and abortion restrictions and bans limit the range of treatment options they can receive, as has been shown in multiple high-profile cases of pregnant people who have been denied care. The threat of criminalization and penalties for clinicians who provide abortions in states with bans creates an unmeasurable yet important chilling effect on clinical care. There is also a growing concern that abortion restrictions create a medical and legal environment that exacerbates health inequities, making some people of color who are experiencing a pregnancy loss hesitant to seek care due to the ongoing biases and discrimination in the health care and legal systems. This brief examines pregnancy loss management in the Dobbs era and explores how limiting or banning abortion may have negative consequences on people experiencing pregnancy loss.
An Overview of Pregnancy Loss
Pregnancy loss, which includes miscarriage and stillbirth, is common, occurring in up to an estimated 20% of all pregnancies. Among the US medical community, the term miscarriage (or spontaneous abortion) refers to a spontaneous loss of a nonviable, intrauterine pregnancy before 20 weeks of gestation. Most pregnancy losses occur in the first trimester before 13 weeks gestation. Stillbirth (also called fetal death and intrauterine fetal demise) is the loss of a pregnancy at or after 20 weeks gestation. Since many miscarriages happen early in pregnancy and without medical intervention, data are very limited. Rates of stillbirth have declined over the past three decades, yet roughly 1% of births in the U.S. end in stillbirth, which translates to more than 21,000 stillbirths annually. Cases of stillbirth are unexpected and extremely stressful. and can be traumatic for pregnant people and their loved ones.
Often, the cause of a pregnancy loss is unknown even after thorough evaluation. Of those with a suspected cause, the majority of miscarriages are attributed to genetic abnormalities. Similarly, most stillbirths are caused by genetic abnormalities, problems with the placenta, fetal growth restriction, or infection.
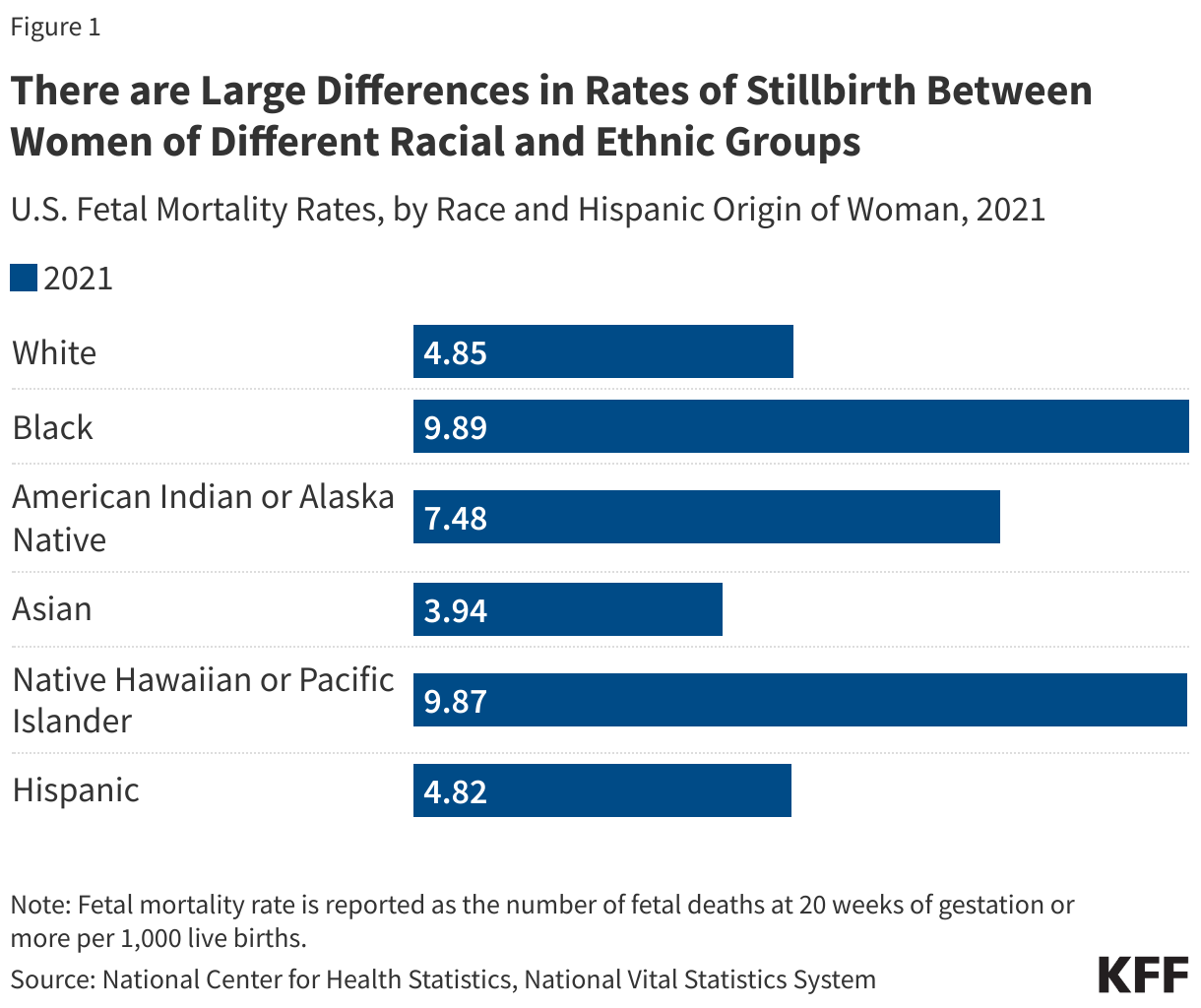
The rates of pregnancy loss are higher among some populations, particularly Black and Native Hawaiian or Pacific Islander women. Black women are more likely to experience miscarriage and stillbirth (commonly reported as a fetal mortality rate) than their White counterparts. According to data from the National Center for Statistics, fetal mortality rates were highest among Black and Native Hawaiian or Pacific Islander people in 2021 (Figure 1).
This underlying disparity is not fully understood. Broader social and economic factors and structural and systemic racism and discrimination play a major role in shaping health and disparities in health. In maternal and infant health specifically, the intersection of race, gender, poverty and other social factors shapes individuals’ experiences and outcomes. Studies have linked long-term psychological stress and “weathering” to poor pregnancy outcomes such as pregnancy loss. Under Dobbs, there is concern that restrictive abortion policies such as outright abortion bans and gestational limits will exacerbate inequities in birth outcomes.
Constraints on Treatment Options
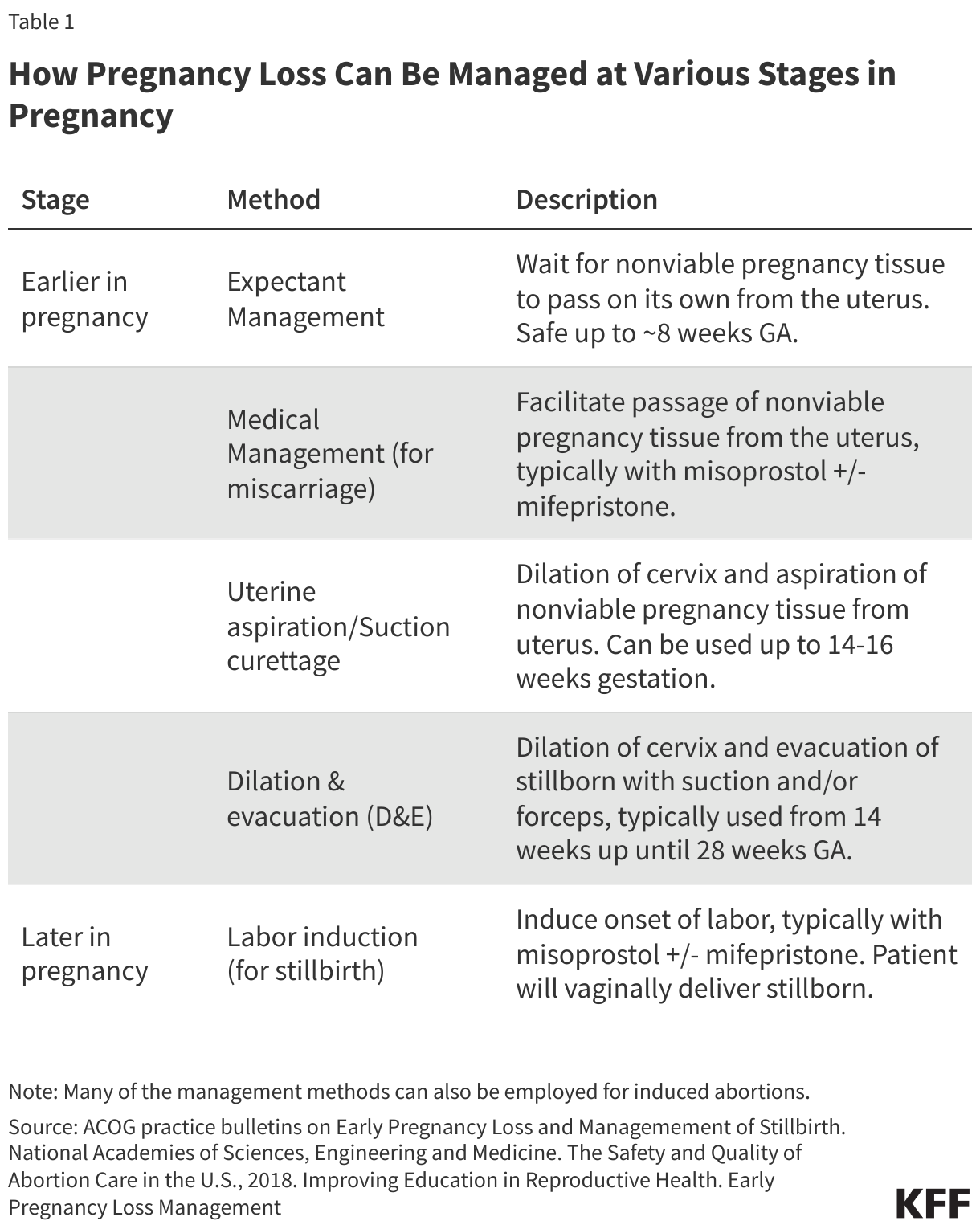
Depending on the stage in pregnancy, the pregnant person’s preferences, and the clinical scenario, patients experiencing pregnancy loss can be managed with (1) expectant management, (2) medications, like misoprostol with or without mifepristone, or (3) a medical procedure, either uterine aspiration (D&C) or dilation and evacuation (D&E). Almost all of the clinical interventions used to manage miscarriages and stillbirths are identical to those used in abortions because they result in emptying the pregnant person’s uterus. Pregnant people experiencing a miscarriage or a lethal fetal anomaly may seek one of these treatments to complete the loss and/or because their health may worsen with continuation of the pregnancy (Table 1).
The medications that can be used to manage early miscarriages – misoprostol and mifepristone – are the same ones used for a medication abortion. Medication abortion, also known as medical abortion or abortion with pills, is a medical regimen that terminates a pregnancy by taking two different drugs, mifepristone and misoprostol. This regimen is approved in the U.S. for use up to the first 70 days (10 weeks) of pregnancy, and accounts for the majority (63%) of all abortions today. These medications are also commonly used to manage early pregnancy loss. Although most miscarriage patients who receive medications to complete the miscarriage are given misoprostol alone, the combination of the two drugs is more effective, and this protocol is recommended by ACOG and other professional clinical organizations.
Since it was first approved for use in the U.S. more than 20 years ago, the provision of mifepristone has been subject to many federal requirements, including the FDA’s Risk Evaluation and Mitigation Strategy (REMS) restrictions, which initially only permitted physicians to dispense the medication to the patients with an in-person visit. Over the years, with the addition of many studies demonstrating the safety and effective of the drugs, some of these restrictions have been modified, now allowing certified non-physician clinicians to prescribe and dispense mifepristone. Nonetheless, in a case currently pending a decision from the Supreme Court, FDA v. Alliance for Hippocratic Medicine, a group of anti-abortion clinicians claim that the FDA did not follow the correct processes in making these changes, and that the Supreme Court should revert to older protocols for mifepristone across the country. If the Court decides to reinstate older protocols, people experiencing an early miscarriage would likely be unable to obtain the medication via mail, at a commercial pharmacy, or to manage their miscarriage if it occurs after 7 weeks, limiting miscarriage management options in all states across the country.
Some pregnancy losses are managed by the same medical procedures used for abortions. This includes D&C, D&X, and D&E procedures. The D&C is most common and can be used up to approximately 16 weeks gestation. Even prior to Dobbs, some states had laws that banned or limited clinicians’ use of the rarely used dilation and extraction (D&X) procedure, (the so-called “partial birth abortion”, which is not a medical term but has been used by anti-abortion policymakers to refer to the D & X procedure), which can be used both to provide an abortion and manage a stillbirth.
State abortion bans may result in the use of expectant management (waiting for the contents of the uterus to empty on its own) in cases where it is not medically indicated, because of clinicians concerns about civil or criminal penalties associated with the violation of state abortion bans. Alongside medications and procedures, expectant management, which refers to waiting for the miscarriage to resolve on its own without any medical intervention, is considered another form of care for pregnancy loss. Expectant management is generally restricted to the first trimester, due to lack of safety studies and concerns about hemorrhage in the second trimester. When pregnant people who are experiencing a loss after the first trimester do not have the option for a D&C or other procedure due to the effects of an abortion ban, they may be forced to wait and let the miscarriage pass on its own– even when it is not recommended, which can endanger their health.
While all state abortion bans have exceptions to preserve the life of the pregnant person, it is not clear if and when exceptions apply to cases of pregnancy loss that are harming the pregnant person’s health. Many miscarriages have harmful effects on physical and mental health but they may not be considered imminently life threatening. Clinicians in states without explicit exceptions for miscarriages may fear criminal liability or loss of their medical license or financial penalties if they provide treatment in these cases. This can lead to delays in care, so that even when a miscarriage or inevitable loss is harming the pregnant person’s health, but fetal cardiac activity is still detectable, clinicians may deny or postpone termination of the pregnancy until a patient’s life is more overtly “threatened” or “endangered”. Some supporters of abortion bans and restrictions state that they are not intended to withhold treatment for pregnancy loss. However, the legal standards for when a pregnant person qualifies for a life or health exception vary, with some states leaving physicians in a legally vulnerable position such that an expert witness could contradict their medical judgment. In the 2023 national KFF Survey of OBGYNs, the majority of OBGYNs (61%) practicing in states with abortion bans reported they are concerned about their legal risk when making decisions about the necessity of abortion care for their patients, much higher than those who practice in states where abortion is available.
Timeliness and patient preferences are important elements of miscarriage management, and several documented cases of miscarriage or inevitable pregnancy loss demonstrate the impracticability of trying to legislate the circumstances around clinical care. In the wake of the Dobbs ruling and state abortion bans, the federal government reiterated hospitals’ obligations under the federal Emergency Medical Treatment and Active Labor Act (EMTALA) law to provide emergency care, including abortion care if it is needed to stabilize the patient. While this guidance may offer clarity to clinicians in some of the most dire and dangerous cases of pregnancy loss, it does not necessarily address the wide array of circumstances that may not immediately rise to the level of “emergent.” This term, in the case, Idaho v. United States, the Supreme Court is considering whether HHS properly issued the guidance and if EMTALA preempts state abortion bans that only allow exceptions under very narrow circumstances – to prevent the pregnant person’s death. The narrow scope of exceptions in state abortion bans is also being debated in multiple cases in state courts as well.
Some fetal anomalies that are detected during the prenatal period may eventually lead to a loss during pregnancy or soon after birth. Additionally, few of the state bans explicitly make exceptions for provision of care when a lethal or severe fetal anomaly has been diagnosed. In these cases, a pregnant person may not be actively losing a pregnancy, but the condition is such that there is a high chance of miscarriage, stillbirth or death of the child shortly after birth. Some pregnant people may want to continue their pregnancies after such a diagnosis, but in states without exceptions for lethal anomalies, pregnant people may be forced to continue a pregnancy where loss is inevitable, although not necessarily always imminent. In some cases, this may place pregnant people at risk for childbirth-related health risks when a termination earlier in the pregnancy would have been less risky to them. While some people who reside in states where abortion is banned have traveled out of state to obtain abortion services after a fatal fetal anomaly diagnosis or while actively miscarrying, this may not be an option for many people. The significant financial and logistical costs, including transportation, lodging, childcare, and time off work to just name a few can be insurmountable barriers to traveling out of state for care.
Constraining Clinical Care and Judgement
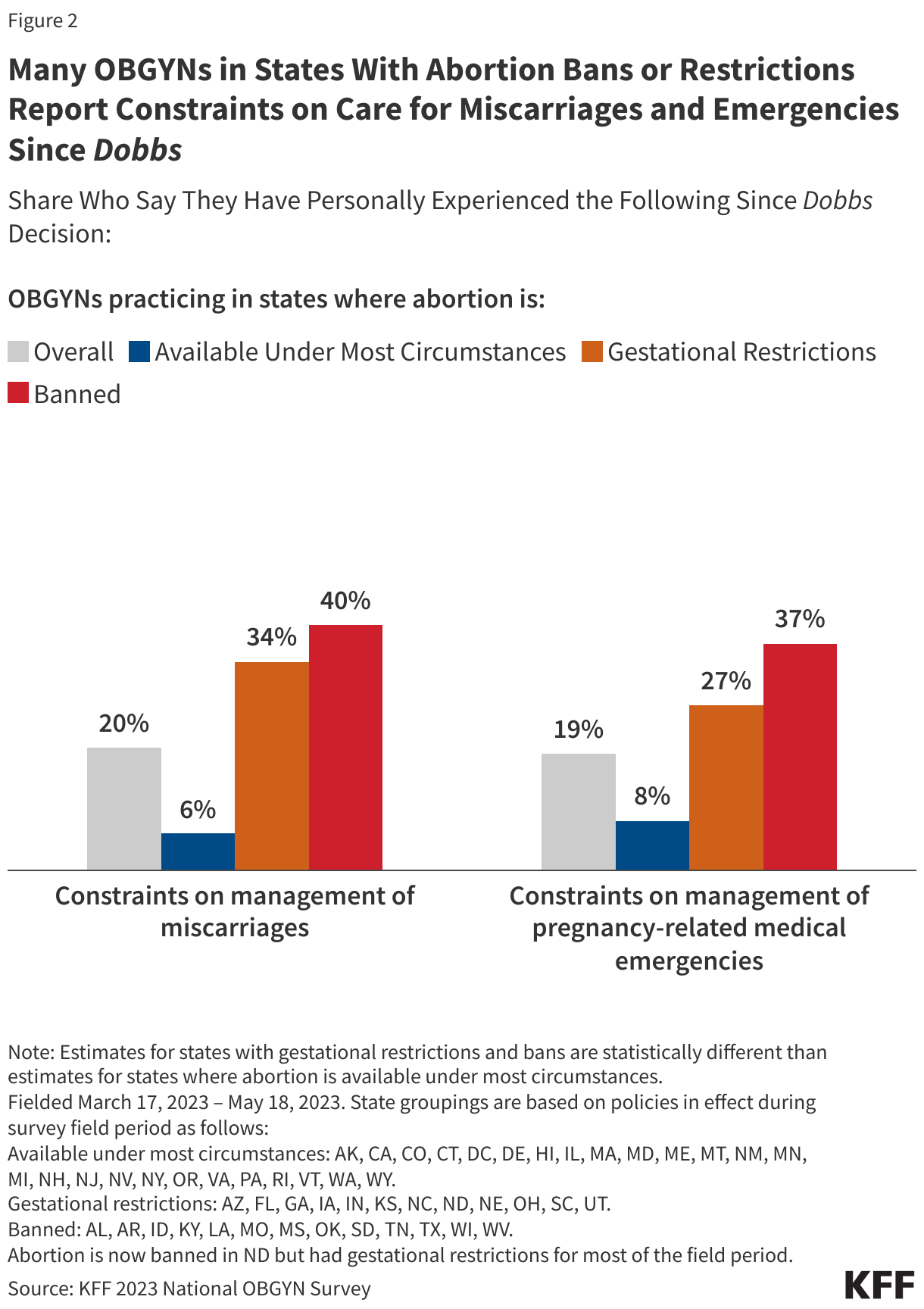
Since Dobbs, clinicians in abortion restrictive states report that they are facing constraints in caring cases of pregnancy loss. In the KFF 2023 Survey of OBGYNs, one in five OBGYNs nationally said they have been constrained in providing care for miscarriages (20%) and pregnancy-related emergencies (19%) since the Dobbs ruling. However, this is significantly higher among OBGYNs in states that ban or restrict abortion, compared to those practicing in states where abortion is available under most circumstances (Figure 2).
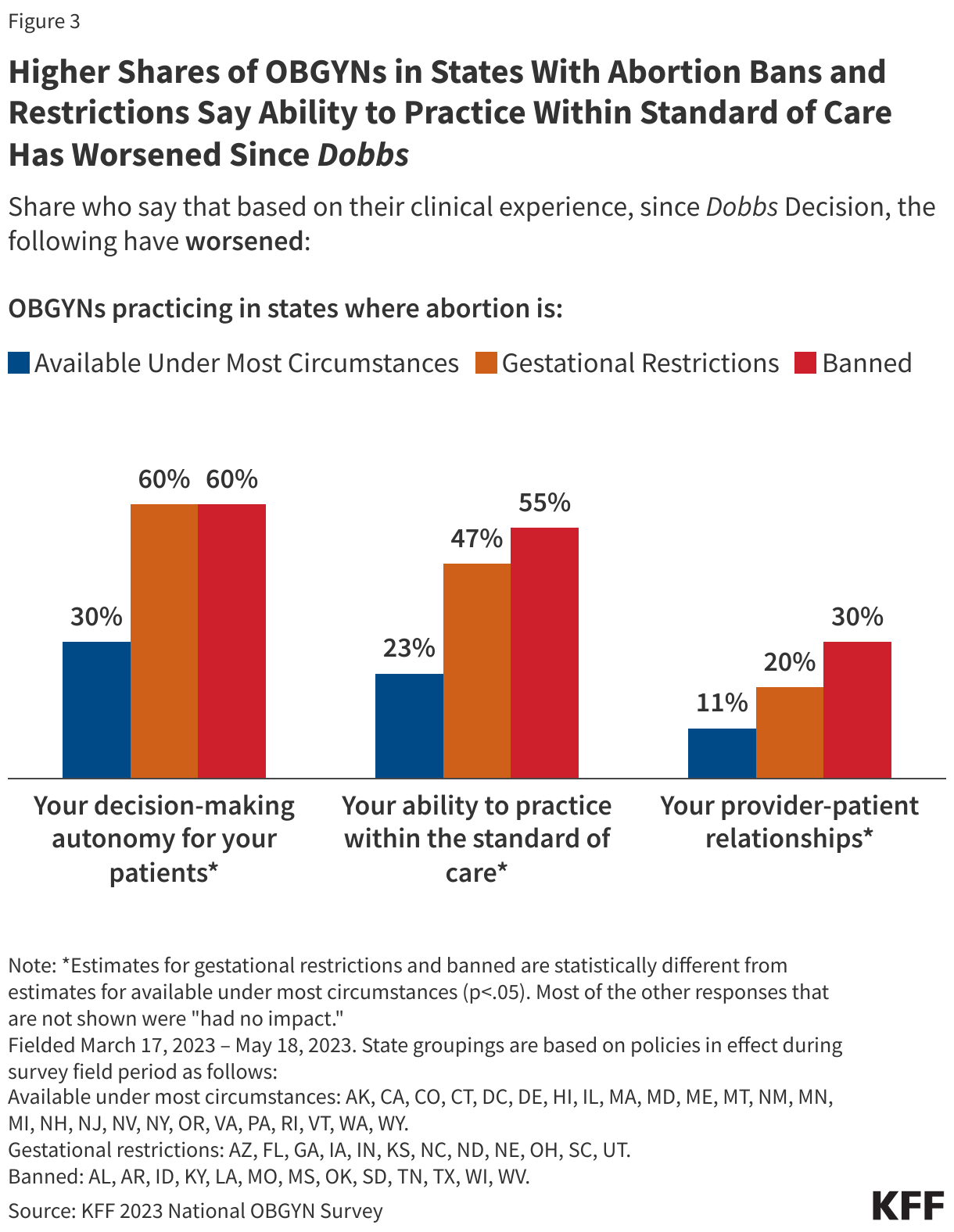
Abortion bans and restrictions may also hinder clinician counseling, an essential element of the patient-clinician relationship for pregnancy loss. The standard of care for pregnancy loss counseling is to inform pregnant patients of all the options. Prior to Dobbs, clinicians in all states could offer this counseling; however, in states that now have bans and gestational limits, clinicians may fear that they cannot offer all of these options, nor referrals to this care. In states with bans, many OBGYNs do not even give patients referrals to clinicians out of state who offer abortions. This may be particularly heightened in states such as TX that have enacted laws that prohibit aiding and abetting the receipt of abortion services. More than half of OBGYNs practicing in states with abortion bans (55%) say that the Dobbs decision has made their ability to practice within the standard of care worse, more than twice the share (23%) who practice in states where abortion is available (Figure 3).
Laws that grant “fetal personhood” may deter people experiencing pregnancy loss from seeking medical care, alter the patient-provider relationship, and promote mistrust between patients and clinicians. Miscarriage, stillbirth, and abortion have all been heavily stigmatized in our society. Prior to Dobbs, there were several cases of pregnant people facing charges for fetal harm, endangerment, and other crimes because they engaged in activity that was alleged to harm their fetuses, most often substance use while pregnant. Since Dobbs, fear of seeking care may be heightened in states with bans or restrictions because patients could be accused of “self-managing ” an abortion, especially since accusations of fetal harm often come to the attention of law enforcement by health care professionals.
This can be especially risky for some people of color who already suffer poorer maternal outcomes, harbor greater distrust towards the medical community, have higher rates of pregnancy loss, and higher rates of criminalization for self-managed abortion. Symptoms of pregnancy loss are indistinguishable from “self-managed” abortions.
State abortion bans and restrictions raise concerns about the preparedness of future health care professionals to effectively treat pregnancy loss. Training in abortion care is an important skill for all clinicians who care for pregnant people since those services are also used in management of miscarriages and stillbirths. The Accreditation Council for Graduate Medical Education (ACGME) requires all U.S. OBGYN residency programs provide training in miscarriage management as well as “opt out” access to abortion training for their residents. Surveys of resident physicians have found that those who received training in abortion care felt more prepared to provide care for pregnancy losses after training.
Even prior to Dobbs, only 60% of OBGYN residents reported having routine access to abortion training. Clinical trainees in states that now ban abortion may now have to travel out of state to obtain training on management of pregnancy loss. Logistical obstacles related to travel, coordination with home programs, financial costs, and housing, may impede the ability of some trainees to travel out of state to obtain the necessary training and caseload to become proficient in these skills. Furthermore, programs in states where abortion remains legal may not have the capacity to meet the demand from trainees other states and limit options to have rotations for out-of-state clinicians and still train their own residents and students. Furthermore, clinicians other than OBGYNs care for pregnant patients and need training on management of pregnancy loss, including physicians in family practice and emergency medicine, midwives, nurses, and other advance practice clinicians.
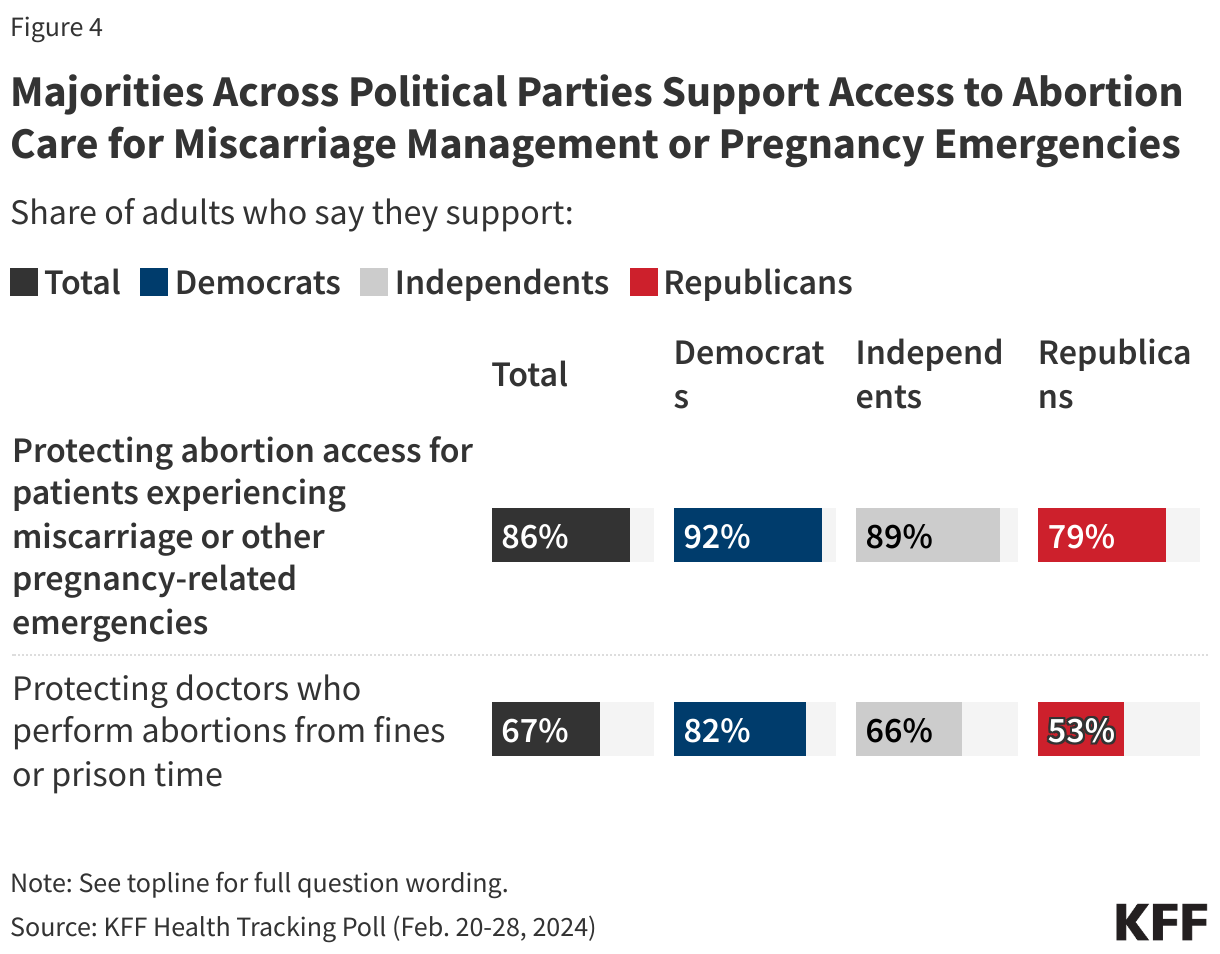
Majorities across party lines support access to abortion care for people experiencing pregnancy losses and protecting doctors who offer abortions from criminal or financial penalties (Figure 4). There have been numerous reports and litigation brought by pregnant women experiencing pregnancy loss or imminent fetal demise who have denied miscarriage management and emergency medical care in states that have banned abortion. Abortion generally will be a significant issue in the November 2024 election, and particularly in the states that will have ballot initiatives addressing abortion rights.
The authors would like to acknowledge Tatyana Roberts, a former KFF-UCSF fellow for her work on an earlier draft of this brief and Gabriel Wiegel, MD, a former KFF-UCSF fellow who co-authored an earlier published brief on this topic.