Pandemic-Era Changes to Medicaid Home- and Community-Based Services (HCBS): A Closer Look at Family Caregiver Policies
Issue Brief
KFF estimates that there are over 4 million people using Medicaid home- and community-based services (HCBS), which include medical and supportive services that assist people with the activities of daily living (such as eating, bathing, and dressing) and instrumental activities of daily living (such as preparing meals, managing medications, and housekeeping). They are provided to people who need such services because of aging, chronic illness, or disability and may include personal care, adult daycare, home health aide services, transportation, and supported employment. Medicare generally does not cover HCBS and in 2020, Medicaid spent $162 billion on HCBS—a majority of the $245 billion in total HCBS spending. Although all states offer some HCBS through Medicaid, most services are optional for states, and states may cover different services for different types of Medicaid enrollees. To be eligible for Medicaid HCBS, individuals must have limited financial resources and significant functional impairments.
During the COVID-19 pandemic, people who use HCBS were at heightened risk of serious illness or death from exposure to COVID-19 and were disproportionately likely to need hospital or nursing facility care when HCBS were unavailable, but there were fewer workers available and willing to provide services. Recognizing those challenges, the federal government provided states with new authorities to maintain access to HCBS during the public health emergency (PHE), which was in place from 2020 until May 11, 2023. Family caregivers played a critical role in helping to mitigate the consequences of workforce shortages and many states used the new authorities to support and pay family caregivers.
Drawing from KFF’s 50-state survey of state Medicaid HCBS officials, conducted between May and August of 2023, this issue brief describes how states used the PHE authorities to strengthen their HCBS programs, changes as the PHE ends, and the role of family caregivers in providing HCBS. Key take-aways include:
- States used PHE authorities to strengthen their HCBS programs by expanding access to services and investing in the HCBS workforce, and while some of those changes are transitioning into permanent policies, others are ending as the PHE authorities expire.
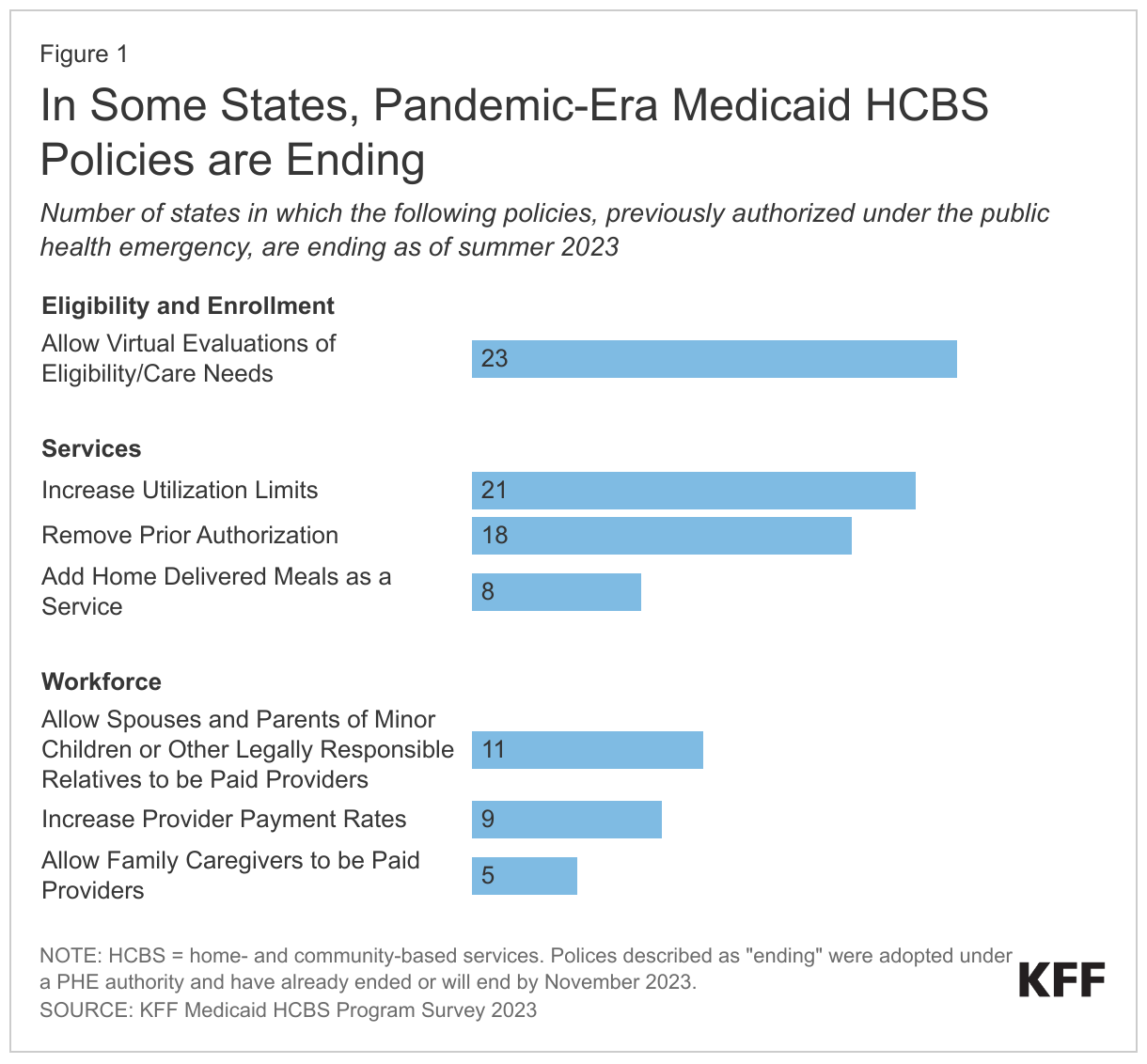
- The most commonly expiring policies will result in the end of virtual evaluations of eligibility and care needs in 23 states, lower utilization limits in 21 states, and reinstated prior authorization in 18 states; changes that may make it harder for Medicaid enrollees to access HCBS or may reduce the amount of HCBS they are able to use (Figure 1).
- Most states now allow family caregivers to be paid for providing personal care, but such payments are most common under waiver programs, which are offered at the states’ discretion and may limit enrollment to people with certain types of disabilities, may cap enrollment or spending at specified levels, and may use waiting lists when the number of people seeking services exceeds the number of waiver slots available.
- In 11 states, payments to family caregivers who are legally responsible for the person they are caring for will be ending and payments to other types of family caregivers will end in 5 states. With ongoing workforce shortages, families may have difficulty finding paid workers to take over their responsibilities when the policies expire.
How did states use public health emergency authorities to support Medicaid HCBS during the pandemic?
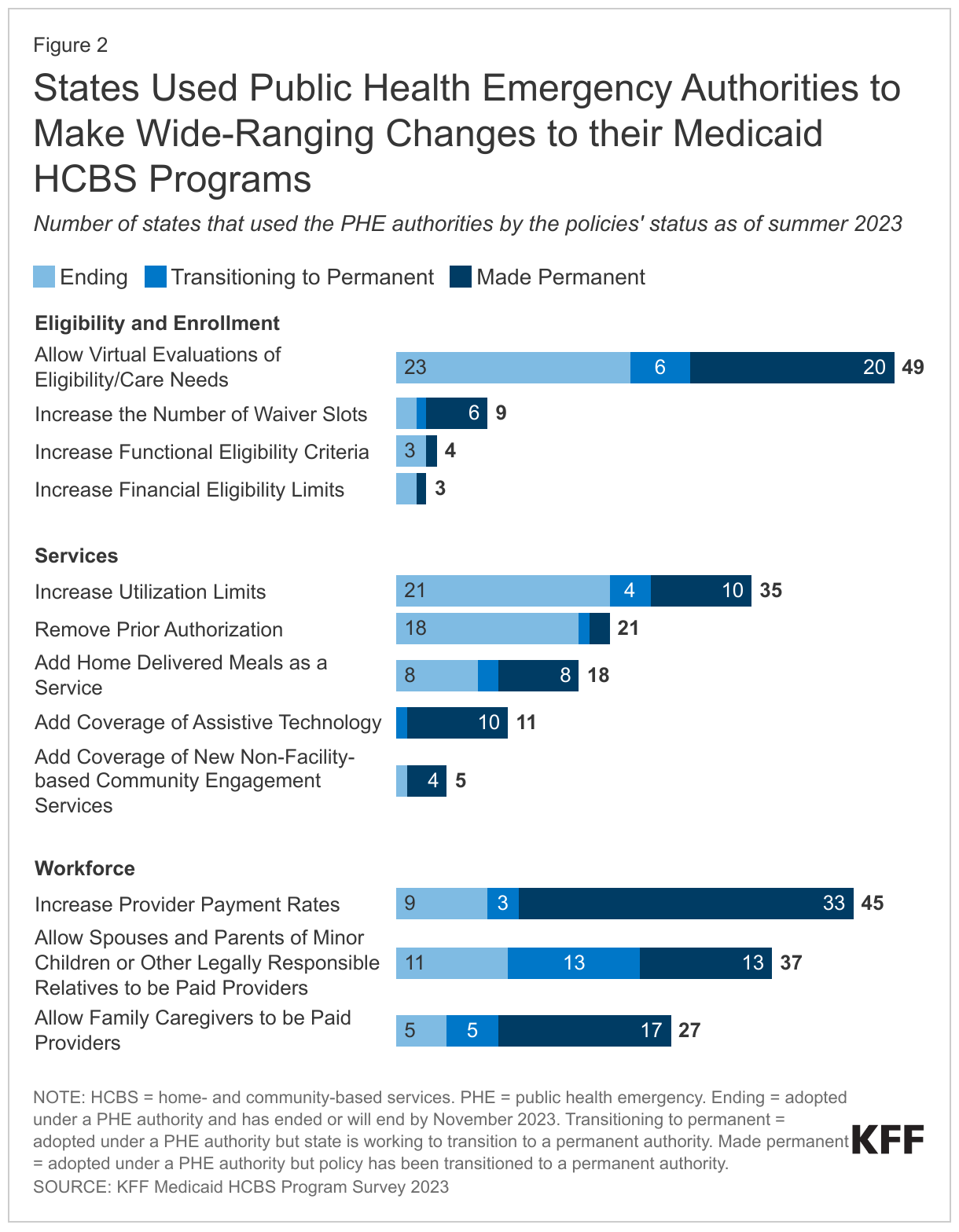
In a 2023 survey of states’ Medicaid HCBS programs, all responding states reported using PHE authorities to strengthen their programs by addressing eligibility and enrollment processes, increasing the availability of services, and addressing workforce challenges (Figure 2, Appendix Table 1). Responding states include the District of Columbia and all states except for Florida. The most common changes included allowing virtual evaluations of people’s eligibility for HCBS or the level of care needed (49 states), increasing payment rates to providers (45 states), allowing spouses and parents of minor children or other legally responsible relatives to be paid providers (37 states), increasing utilization limits on existing services (35 states), and allowing other family members or friends to be paid providers (27 states).
States made these changes using several types of authorities when responding to the COVID-19 PHE, including disaster-relief state plan amendments, 1115 waivers, and Appendix K changes to 1915(c) waivers. When the PHE ended on May 11, 2023, changes made through a disaster-relief state plan amendment or 1115 waiver also ended unless they had been moved to a permanent authority. Changes made using the Appendix K authority will expire within 6 months of the PHE ending (November 11, 2023) unless the state incorporates those changes into section 1915(c) waiver programs.
Although nearly all states are making some of their changes permanent, many other PHE-era policies are ending as the authorities expire. Among states responding to the survey, all states except for Kentucky and New Jersey plan to keep at least one of the policies that they enacted during the PHE. Some policies have already been made permanent—most commonly, increased payment rates (33 states), virtual evaluations of eligibility or level of care (20 states) and allowing family caregivers to be paid providers (17 states). Other policies are currently being transitioned from temporary to permanent authorities, with 13 states currently in the process of transitioning a policy allowing spouses, parents of minor children, or other legally responsible relatives to be paid providers. In other cases, the policies enacted during the PHE are ending, with 23 states ending virtual evaluations of eligibility or level of care, 21 states ending higher utilization limits, and 18 states reinstating prior authorization.
As the public health emergency authorities end, how are states supporting family caregivers?
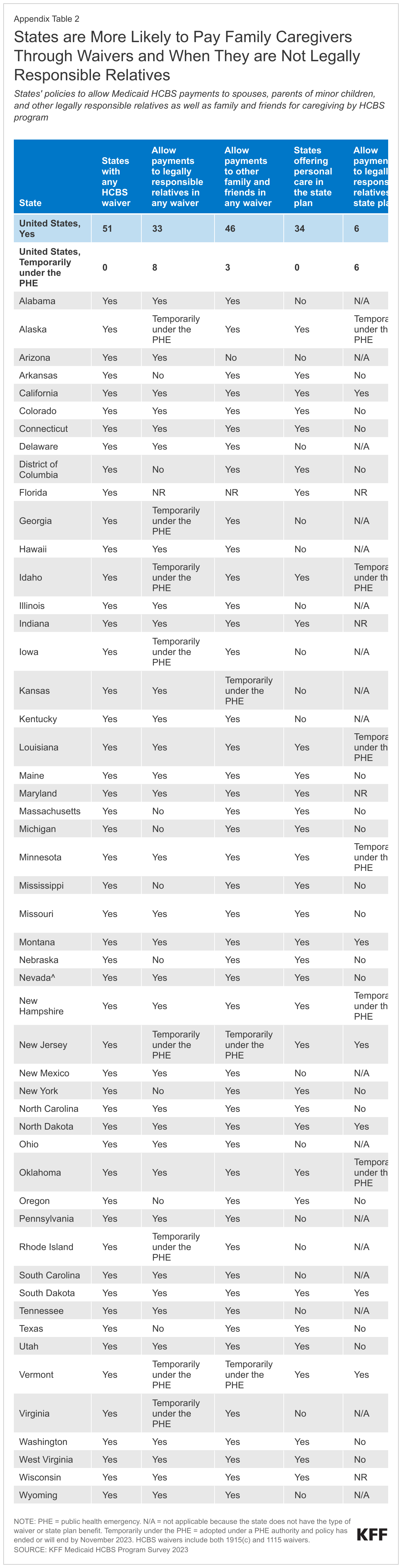
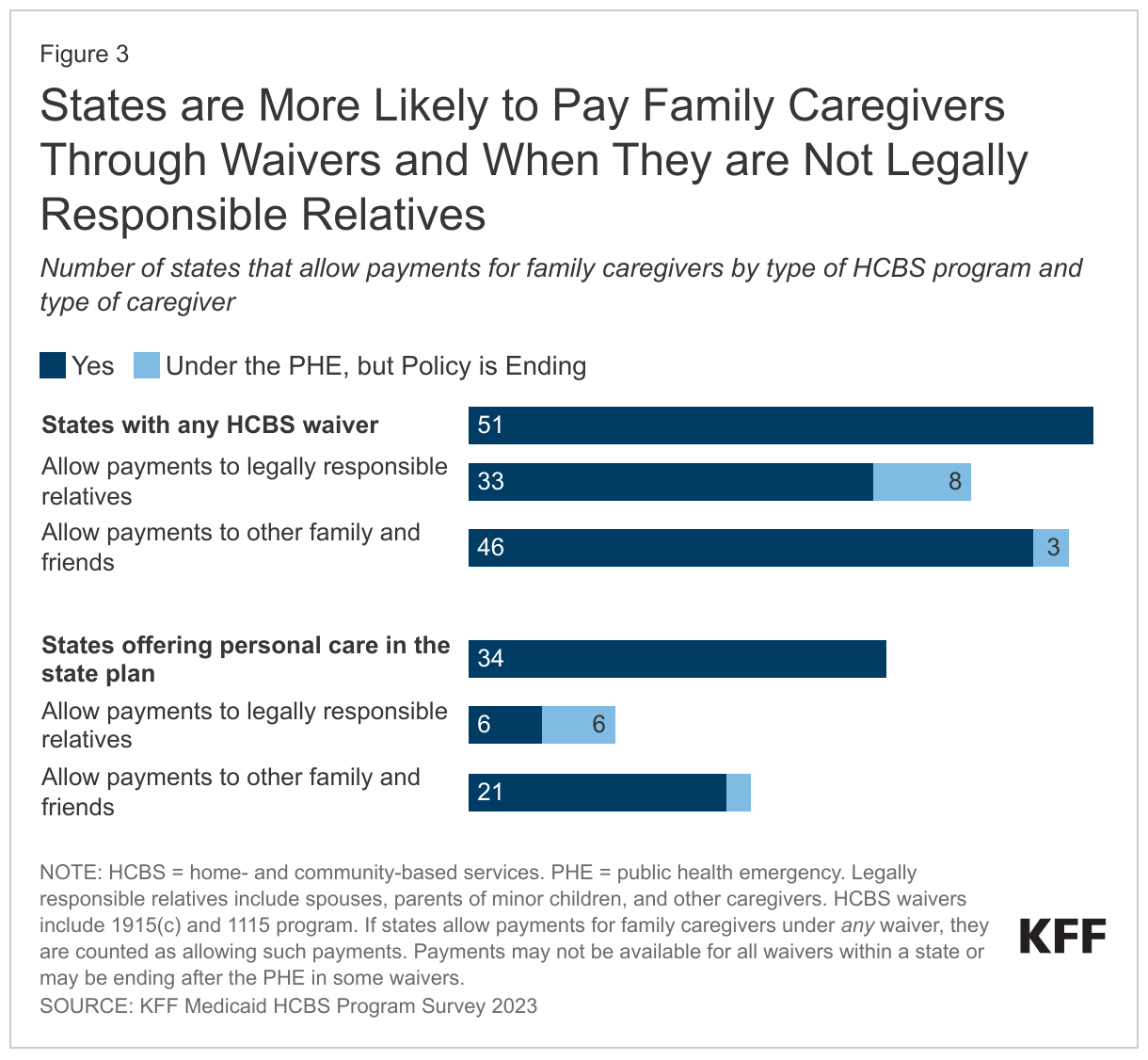
The availability of payments for and support of family caregivers increased during the PHE and even as PHE authorities end, nearly all states allow payments to family caregivers for at least one of their HCBS programs (Figure 3, Appendix Table 2). Payments for family caregivers are generally allowed for the provision of personal care, which may be offered through several different types of Medicaid HCBS programs. Personal care may be provided through waivers such as 1115 or 1915(c) programs, through the Medicaid state plan, or a combination of both. Waiver services tend to encompass a wider range of benefits than the state plan benefit, but waivers are usually restricted to specific groups of Medicaid enrollees based on geographic region, income, or type of disability; and are often only available to a limited number of people, resulting in waiting lists. In 2023, all 50 states and DC offered HCBS through at least one waiver and 34 states offered personal care as a state plan benefit.
States were more likely to allow family caregivers to be paid if they were not legally responsible for the person receiving care and if the person receiving care was enrolled in an HCBS waiver. Among the 50 states with HCBS waivers that responded to the survey, 41 states allow payments to spouses, parents of minor children, and other legally responsible relatives and 49 states allow payments for other family members and friends (those who are not legally responsible relatives). Among the 34 states providing personal care through the Medicaid state plan, 12 states allow payments to legally responsible relatives and 23 states allow payments to other family members and friends. Those numbers include states that allow payments to family caregivers on an ongoing basis and states that only authorized such payments through a PHE authority. The totals also include states that allow payments for family caregivers under at least one of their waivers, but most states have more than one waiver, and such payments may not be permitted under all waivers.
Payments to legally responsible relatives are more likely to end after the PHE authorities expire than are payments to other family and friends. For the state plan benefit, the number of states only paying family members under a PHE authority was 6 states for legally responsible relatives (Alaska, Idaho, Louisiana, Minnesota, New Hampshire, and Oklahoma) and 2 states for other family members and friends (Missouri and New Hampshire). For waiver programs, the number of states that only allowed payments for family caregivers under a PHE authority for any waiver program in the state was 8 states for legally responsible relatives (Alaska, Georgia, Idaho, Iowa, New Jersey, Rhode Island, Vermont, and Virginia) and 3 states for other family and friends (Kansas, New Jersey, and Vermont). Because most states have different policies for different waivers, a larger number of states will have payments to family caregivers ending for specific waiver programs as shown in the next figure.
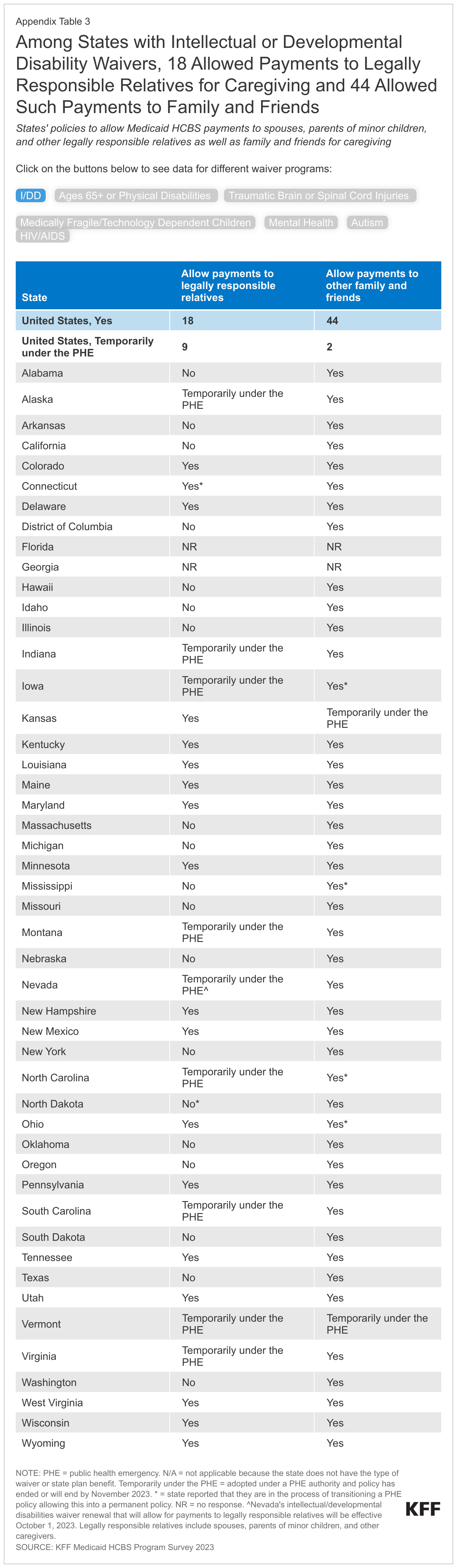
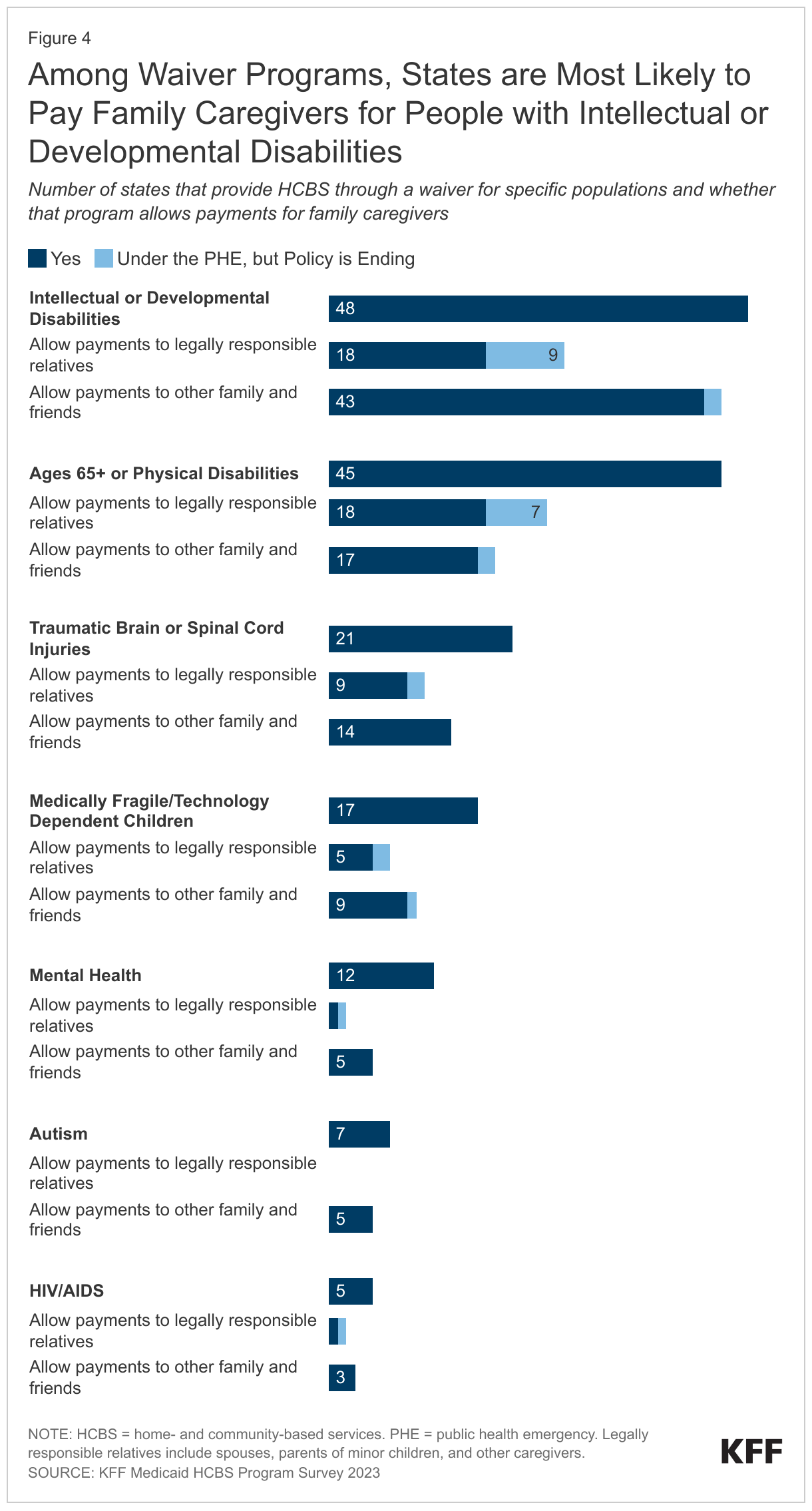
Payments to family caregivers are most common for people with intellectual or developmental disabilities and people who are ages 65 and older or with physical disabilities (Figure 4, Appendix Table 3). Most state waiver programs are limited to people with specific types of disabilities—most commonly, intellectual or developmental disabilities (48 states) and people who are ages 65 and older or have physical disabilities (45 states). Among the states with waivers for people with intellectual or developmental disabilities, 18 states allow payments to legally responsible relatives and 43 states allow payments to other family and friends. Among the states with waivers for people who are ages 65 and older or with physical disabilities, 18 states allow payments to legally responsible relatives and 17 states allow payments to other family and friends.
Several states report that payments to family caregivers will end when the PHE authorities expire. Payments to legally responsible relatives were allowed under the PHE but will be ending in 9 states with waivers for people with intellectual and developmental disabilities, in 7 states with waivers for people who are ages 65 and older or with physical disabilities, in 2 states for people with traumatic brain or spinal cord injuries, and in 2 states for children who are medically fragile or technology dependent. (These numbers are higher than the numbers reported overall in Figure 3 because many states allow payments for family caregivers indefinitely for some waivers but only temporarily for other waivers.)
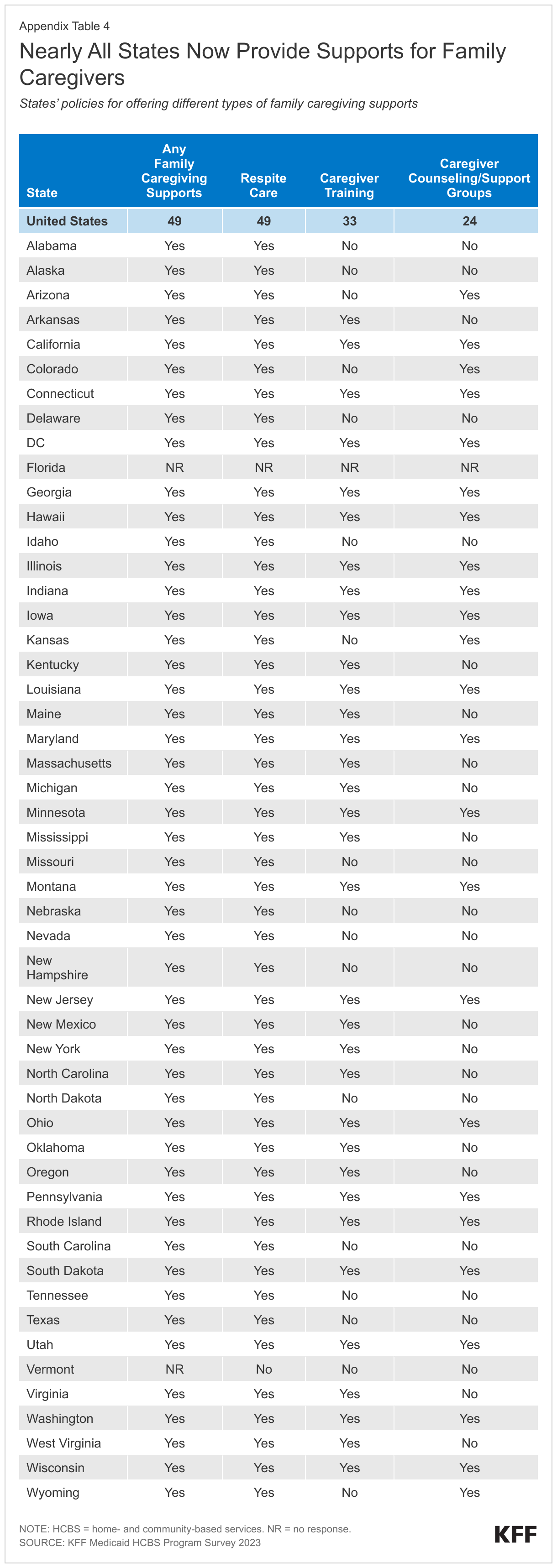
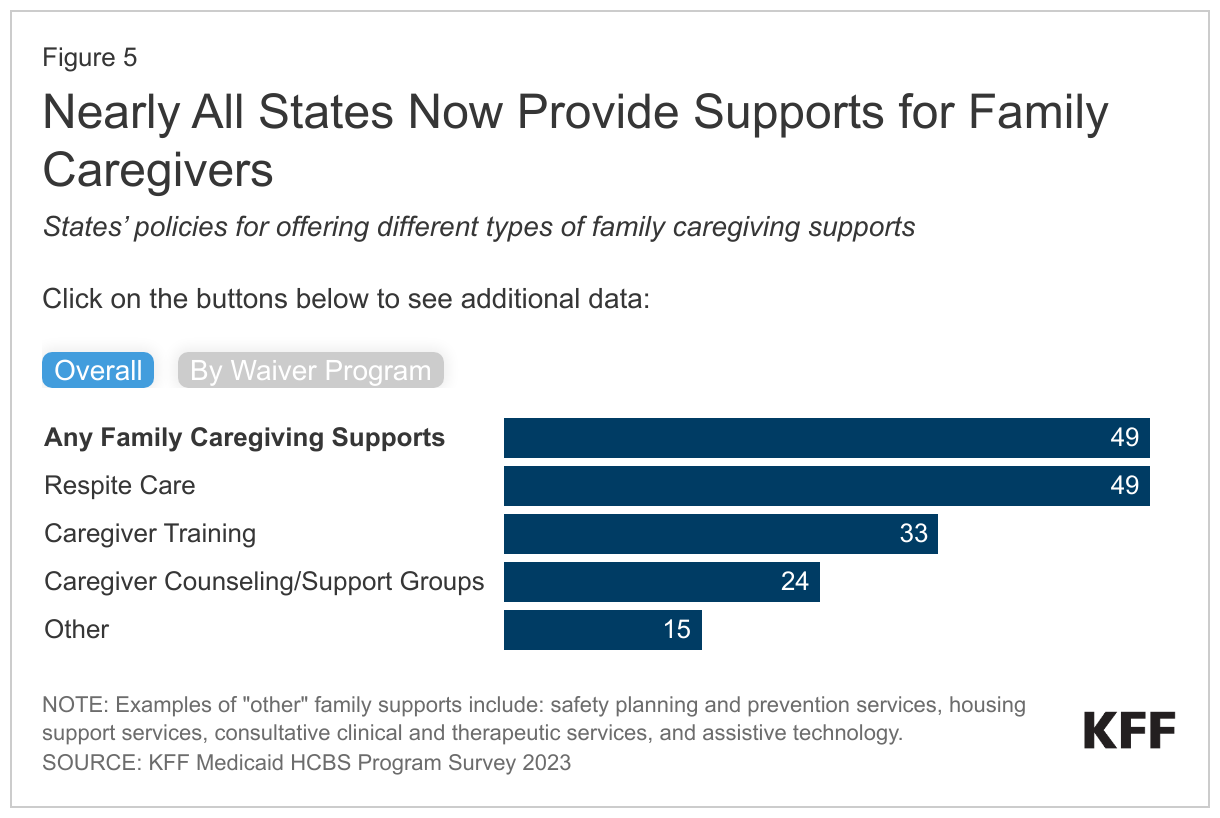
Nearly all states now provide support for family caregivers—who may be paid or unpaid—and most states offer more than one type of support (Figure 5, Appendix Table 4). Almost all (49) states offer at least one family caregiving support in their HCBS programs, and 39 states offer more than one family caregiving support. These supports frequently include respite care (49 states), caregiver training (33 states), and caregiver counseling/support groups (24 states). For all types of waivers, respite care was the most frequently reported support offered and caregiver counseling or support groups was the least frequently reported.
What challenges might Medicaid enrollees who use HCBS face as the PHE ends?
As the PHE authorities expire, there may be additional barriers to accessing HCBS in some states. Although many states are working to make the PHE changes permanent, 23 states will cease evaluating eligibility virtually, 2 states will reduce financial eligibility, 3 states will reduce functional eligibility, and 2 states will reduce the number of waiver slots. Concurrently, 21 states will reinstate utilization limits and 18 states will reinstate prior authorization. Some of those changes will reduce the number of people who are eligible for HCBS or reduce the amount of HCBS eligible enrollees may use.
New HCBS-related administrative barriers could exacerbate the challenges Medicaid enrollees are already experiencing from the unwinding of the pandemic-era continuous enrollment provision, which has resulted in 6.5 million Medicaid enrollees losing coverage as of September 15, 2023. Between February 2020 and March 2023, states received enhanced federal Medicaid funding for keeping people continuously enrolled in Medicaid, and states are now redetermining eligibility for all Medicaid enrollees. Although most people who use HCBS are unlikely to have income or employment changes that render them ineligible for Medicaid, they must still demonstrate their continued eligibility, and some could lose coverage for procedural reasons.
Beyond administrative hurdles, the end of the PHE authorities may place further strain on the HCBS workforce and on family caregivers who provide HCBS. Many of the PHE authorities were enacted in response to HCBS workforce shortages that were exacerbated by the COVID-19 pandemic. As the pandemic era ends, employment in the long-term services and supports sectors continues to remain below pre-pandemic levels and it is unclear whether HCBS workforce shortages will become worse.
In states where payments for family caregivers are ending for some HCBS programs, family members will need to either find new paid workers or will continue to provide care but be unpaid for those services. This situation will be most common for legally responsible relatives who are caring for people with intellectual or developmental disabilities. In states where payments for family caregivers are continuing, such caregivers may experience changes in states’ requirements related to training, documentation, or the maximum number of hours for which they are paid as policies transition to permanent.
Challenges for family caregivers and the HCBS workforce reflect broader challenges in providing care to the many people who use long-term services and supports (LTSS) in both HCBS and institutional settings. The pandemic affected health care workers in all settings but particularly among workers who provide LTSS. As of June 2023, employment levels were still more than 11% below pre-pandemic levels for workers in skilled nursing care facilities and 3% below pre-pandemic levels for workers in elderly care facilities. Recognizing the significance of the LTSS workforce shortage, the Biden Administration has undertaken several steps to bolster the workforce which include issuing major new rules aimed at strengthening the workforce. In HCBS settings, a recent proposed rule on Medicaid access would require states to demonstrate that their payment rates for HCBS are “adequate to ensure a sufficient direct care workforce to meet the needs of beneficiaries and provide access to services.” The rule would also require states to demonstrate that at least 80% of total payments for certain HCBS were compensation to direct care workers. In institutional settings, a recent proposed rule on nursing facility staffing would require facilities to meet minimum staffing requirements and would require states to report on what percentage of Medicaid payments were compensation to direct care workers. Those rules highlight the commitment to supporting LTSS workers, but ultimately, there are only so many people available to provide LTSS and it is likely that challenges will persist.
Appendix Tables