Medicaid and CHIP Eligibility, Enrollment, Renewal, and Cost Sharing Policies as of January 2018: Findings from a 50-State Survey
Medicaid and CHIP Eligibility
Eligibility Limits
As of January 2018, 49 states cover children with incomes up to at least 200% FPL ($41,560 per year for a family of three in 2018) through Medicaid and CHIP, including 19 states that cover children with incomes at or above 300% FPL ($62,340 per year for a family of three in 2018) (Figure 6). Only two states (Idaho and North Dakota) limit children’s Medicaid and CHIP eligibility to lower incomes. The median income eligibility limit for children is 255% FPL ($52,989 per year for a family of three in 2018). Across states, the upper Medicaid/CHIP eligibility limit for children ranges from 175% FPL in North Dakota to 405% FPL in New York. Children’s eligibility levels remained stable under the ACA, reflecting its maintenance of effort (MOE) provision that requires states to maintain eligibility levels for children that are at least as high as those in place when the ACA was enacted in 2010. The recent ten-year extension of CHIP continues the MOE. Beginning after October 1, 2019, the MOE will only apply to children in families with incomes at or below 300% FPL (305% FPL after the five percentage point of income disregard), although states can maintain current eligibility above that level and receive federal CHIP matching funds.
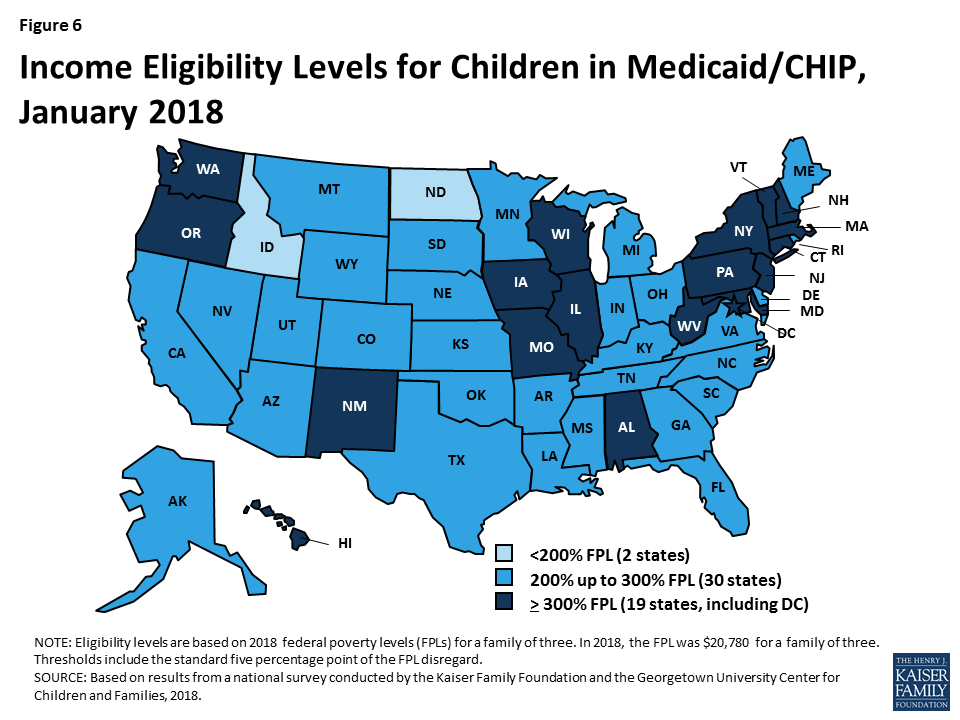
Figure 6: Income Eligibility Levels for Children in Medicaid/CHIP, January 2018
All states cover pregnant women with incomes up to at least 138% FPL ($28,676 per year for a family of three in 2018), and 34 states cover pregnant women with incomes at or above 200% FPL ($41,560 per year for a family of three in 2018) as of January 2018 (Figure 7). Across states, eligibility for pregnant women ranges from 138% FPL in Idaho and South Dakota to 380% FPL in Iowa. These eligibility levels reflect extensions in coverage through CHIP in five states (Colorado, Missouri, New Jersey, Rhode Island, and Virginia). Similar to eligibility levels for children, eligibility for pregnant women remained largely stable across states under the ACA.
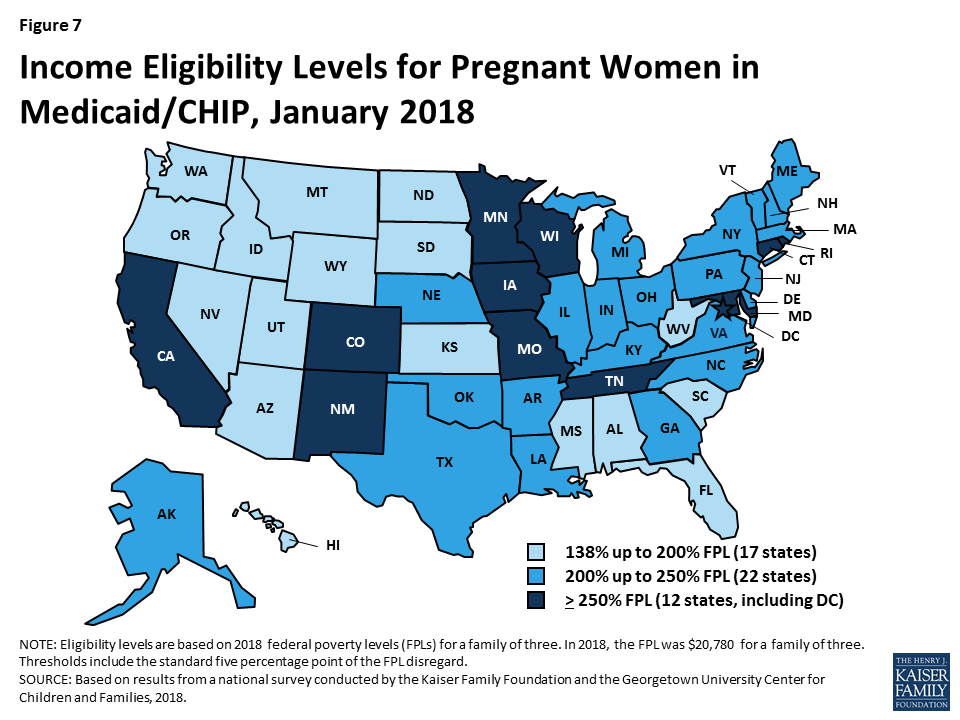
Figure 7: Income Eligibility Levels for Pregnant Women in Medicaid/CHIP, January 2018
As of January 2018, 32 states cover parents and other adults with incomes up to at least 138% FPL ($28,676 per year for a family of three and $16,753 per year for an individual in 2018) under the ACA Medicaid expansion to low-income adults (Figures 8 and 9). The District of Columbia extends eligibility beyond the expansion limit to parents with incomes up to 221% FPL and other adults with incomes up to 215% FPL, and Alaska covers parents with incomes up to 139% FPL. In addition, Minnesota and New York use the ACA Basic Health Program option to cover adults with incomes between 138% and 200% FPL, rather than having individuals in this income range access coverage through the Marketplace.
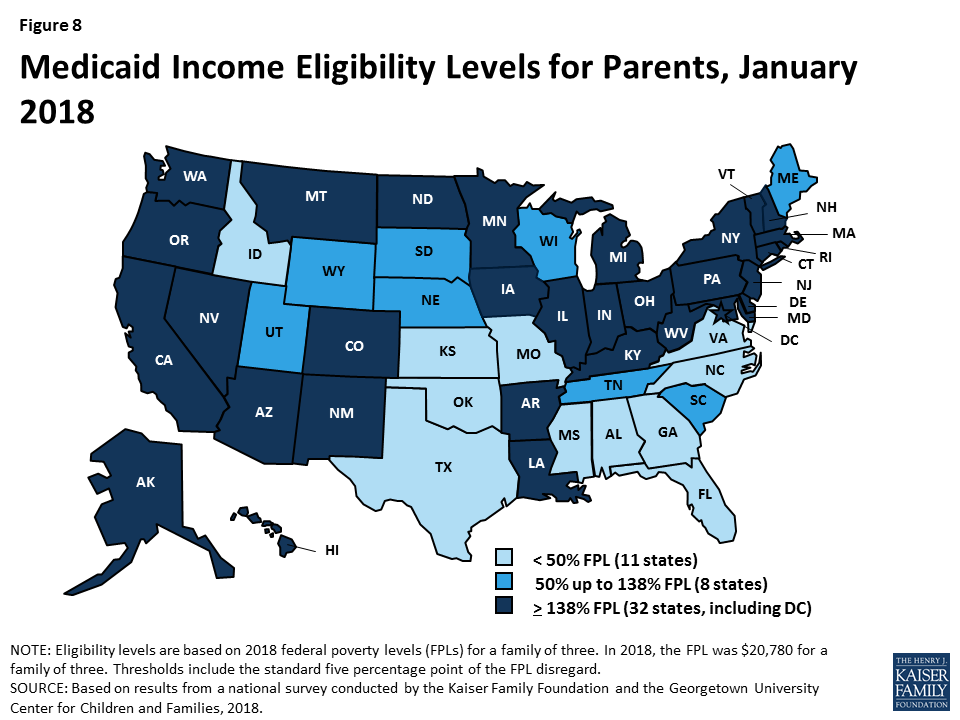
Figure 8: Medicaid Income Eligibility Levels for Parents, January 2018
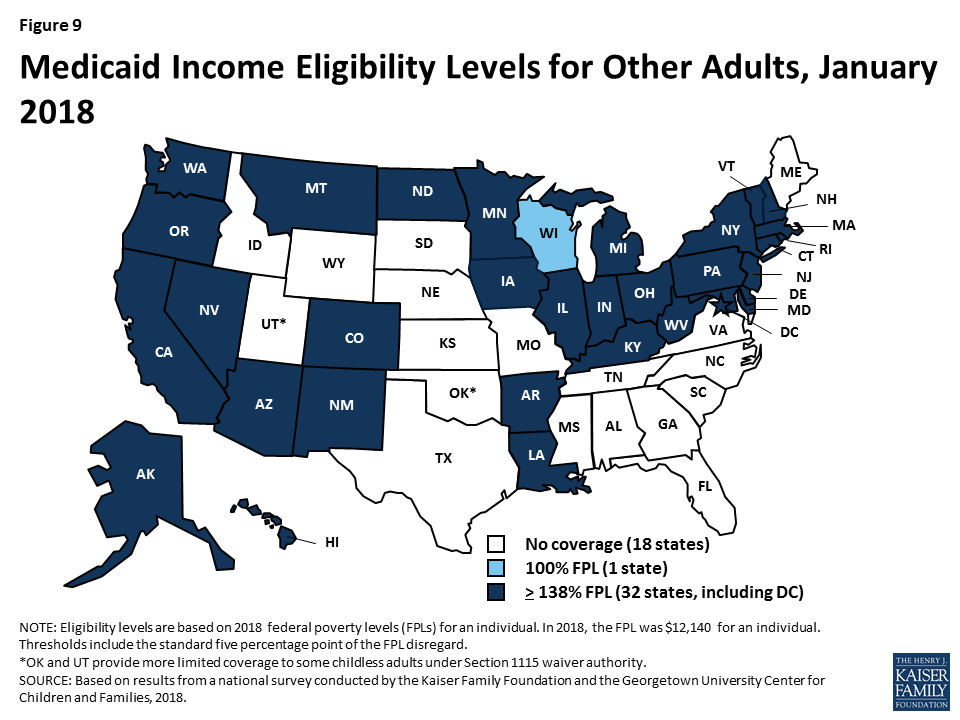
Figure 9: Medicaid Income Eligibility Levels for Other Adults, January 2018
In the 19 states that have not expanded Medicaid, parent eligibility is limited to those with very low incomes and other adults generally remain ineligible, leaving many in a coverage gap. Among non-expansion states, the median eligibility level for parents is 43% FPL ($8,935 per year for a family of three in 2018), and other adults remain ineligible for Medicaid regardless of income, except in Wisconsin. Only Maine and Wisconsin cover parents at or above 100% FPL ($20,780 per year for a family of three in 2018), while 11 states limit parent eligibility to less than half the poverty level (Figure 10). Alabama and Texas have the lowest parent eligibility levels at 18% FPL or $3,740 per year for a family of three in 2018. Given these limited eligibility levels, 2.4 million poor adults fall into a coverage gap in non-expansion states.1 These adults earn too much to qualify for Medicaid but not enough to qualify for subsidies for Marketplace coverage, which become available at 100% FPL.
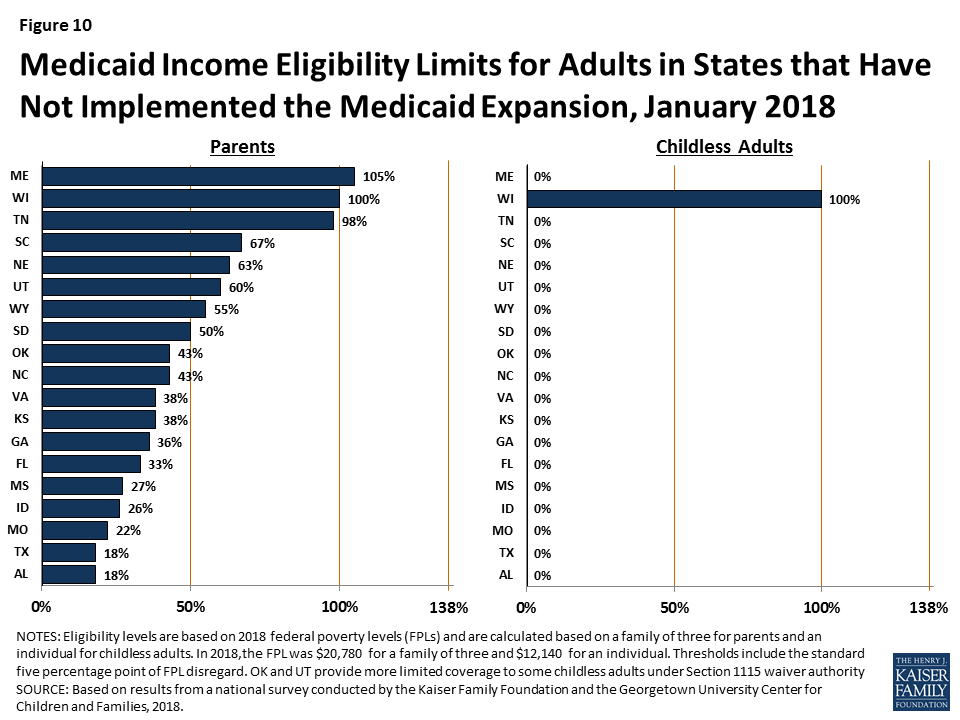
Figure 10: Medicaid Income Eligibility Limits for Adults in States that Have Not Implemented the Medicaid Expansion, January 2018
Eligibility for parents and other adults has significantly increased compared to before the ACA, and the disparity in eligibility for adults in expansion and non-expansion states widened. Prior to the ACA, 34 states limited parent eligibility to less than 100% FPL, including 16 states that had eligibility limits below half of poverty. Moreover, before the ACA, states could not cover other low-income adults with federal Medicaid funds; as such, they generally were not eligible except in some states that obtained waivers. The ACA Medicaid expansion significantly increased eligibility for both parents and other adults. Across states, the median eligibility level for parents increased from 61% FPL ($11,913 per year for a family of three) in 2013 to 138% FPL ($28,676 per year for a family of three) in 2018 (Figure 11). Median eligibility increased from 0% to 138% FPL ($0 to $16,753 per year for an individual) for other adults. States that implemented the Medicaid expansion began with broader eligibility for adults compared to non-expansion states before the ACA. As of 2013, expansion states had a median parent eligibility level of 90% versus 48% in non-expansion states. This gap widened with the expansion.

Figure 11: Median Medicaid Eligibility Levels for Adults as a Percent of the Federal Poverty Level, 2013 and 2018
Eligibility levels remained largely stable during 2017. During 2017, Maine adopted the Medicaid expansion through a ballot initiative, but it has not yet been implemented. . In addition, Utah increased parent eligibility from 45% FPL to 60% FPL and obtained a waiver that expanded coverage to a limited number of adults without dependent children with incomes below 5% FPL who have behavioral health needs.2 In contrast, at the direction of the state legislature, Connecticut reduced parent eligibility from 150% FPL to the Medicaid expansion limit of 138% FPL. Outside of these changes, eligibility levels for parents, adults, children, and pregnant women remained stable.
Targeted Coverage Expansions
Over time, states have continued to take up options to expand coverage to targeted groups that primarily focus on children and pregnant women. Many of these options were available to states before the ACA, but states have continued to adopt them since implementing the ACA to minimize gaps in and increase access to coverage.
- Eliminating waiting periods for CHIP. In 2013, 38 states had waiting periods for CHIP that required children to be uninsured for a period of time before enrolling. These waiting periods were intended to discourage families from dropping private coverage to enroll in the program but contributed to coverage gaps for children. As of January 2018, only 15 states still have waiting periods, while 36 states do not have any waiting period (Figure 12). Between 2013 and 2018, 23 states eliminated their waiting periods and two states (California and Michigan) moved all children from their separate CHIP programs into Medicaid, which does not allow waiting periods.
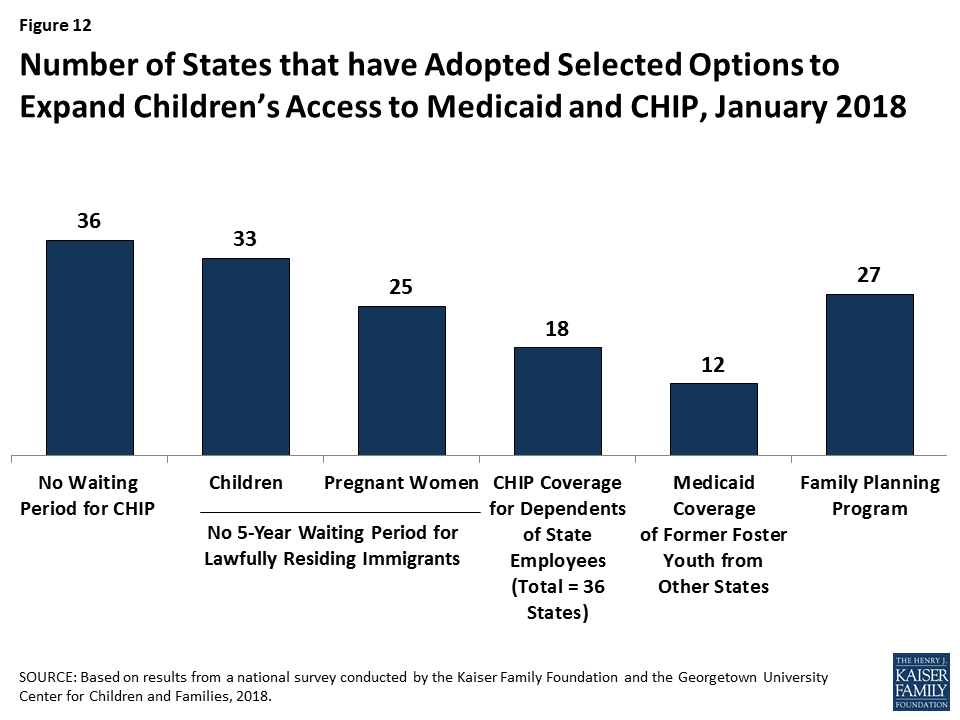
Figure 12: Number of States that have Adopted Selected Options to Expand Children’s Access to Medicaid and CHIP, January 2018
- Coverage for lawfully residing immigrant children and pregnant women. Under federal law, most lawfully present immigrants must wait five years after obtaining lawful status before they may enroll in Medicaid or CHIP. Since 2009, states have had the option to eliminate this five-year wait for lawfully residing immigrant children and pregnant women. By 2013, 25 states had taken up this option for children in Medicaid and/or CHIP and 20 had adopted it for pregnant women. These numbers have increased to 33 states for children and 25 states for pregnant women as of January 2018. In addition, 16 states use CHIP funds to provide coverage through the unborn child option, under which they cover income-eligible pregnant women who are not eligible due to immigration status. Some states also use state-only funds to cover income-eligible individuals who do not qualify for federally funded Medicaid or CHIP coverage due to immigration status; this coverage is often limited to children, pregnant women, or other specified groups.3
- Coverage for dependents of state employees in CHIP. Since 2009, states have had an option to enroll dependents of state employees in CHIP in certain circumstances. Through this option, states can provide a coverage option to children of part-time workers and other state employees who lack access to affordable dependent coverage in the state employee health plan. By 2013, 12 states had implemented the option, and that number grew to 18 of 36 states with a separate CHIP program as of January 2018.
- Coverage for former foster youth from other states. The ACA extended the age that youth who were formerly in foster care could qualify for Medicaid from age 21 to 26. This change mirrors the ACA provision that allows young adults to remain on their parents’ private health plan until age 26. However, a technical error in the law limited the provision to those who were formerly in foster care within the state they were seeking Medicaid coverage. Initially, the Centers for Medicare and Medicaid Services (CMS) allowed states to cover former foster youth from other states as a state plan option. However, it later clarified that states must obtain a waiver to provide coverage to former foster youth from other states. As of January 2018, 12 states were covering former foster youth from other states.
- Family planning programs. States must provide family planning services as a covered benefit to Medicaid enrollees. Historically, some states also used waivers to provide family planning services to women or men who did not qualify for full Medicaid coverage. The ACA made a new state plan option available for states to expand family planning services coverage. As of January 2018, 27 states use federal funds to provide family planning coverage through a waiver or the state plan option.
During 2017, a few states continued to adopt targeted options to expand coverage while others discontinued use of certain coverage options. For example, Arkansas and South Carolina took up the option to eliminate the five-year waiting period for lawfully residing immigrant children and pregnant women, Maine began covering dependents of state employees in CHIP, Delaware added coverage for former foster children from other states, and Georgia increased eligibility for its family planning program from 205% FPL to 216% FPL. In contrast, several states phased out coverage of former foster youth from other states (Louisiana, Montana, and New York). Iowa ended its Medicaid family planning program, but is now covering family planning services with state-only funds.