2014 Employer Health Benefits Survey
Section Thirteen: Grandfathered Health Plans
The Affordable Care Act (ACA) is bringing about a number of changes for the American health care system, including for employer-sponsored health insurance. In 2014 many new provisions took effect for group coverage including limits on waiting periods, out-of-pocket maximums, and many reforms for the small employer market. Other key provisions of the ACA, such as the non-discrimination requirements and the employer shared responsibility provision, were delayed until 2015. In some cases small employers were given new coverage options through SHOP exchanges, although the implementation was limited. SHOP marketplaces were available for shopping for coverage, but firms could not complete the transaction online and had to buy directly from the issuer or through a broker. (For more information, see Sections 2, 7, and 11, and the health reform implementation timeline at http://www.kff.org/interactive/implementation-timeline/.) The ACA exempts certain health plans that were in effect when the law was passed, referred to as grandfathered plans, from some of the new standards in the law; these include requirements to cover preventive benefits without cost sharing, have an external appeals process, or comply with the new benefit and rating provisions in the small group market.
Grandfathering
For the employer-sponsored market, health plans that were in place when the ACA was enacted (March 2010) can be grandfathered health plans. Interim final rules released by the Department of Health and Human Services on June 17, 2010, and amended on November 17, 2010, stipulate that firms cannot significantly change cost sharing, benefits, employer contributions, or access to coverage in grandfathered plans.1 New employees can enroll in a grandfathered plan as long as the firm has maintained consecutive enrollment in the plan.
Grandfathered plans are exempted from many of the ACA’s new requirements, but still must comply with other provisions as they become effective, including: (1) provide a uniform explanation of coverage, (2) report medical loss ratios and provide premium rebates if medical loss ratios are not met, (3) prohibit lifetime and annual limits on essential health benefits, (4) extend dependent coverage to age 26, (5) prohibit health plan rescissions, (6) prohibit waiting periods greater than 90 days, and (7) prohibit coverage exclusions for pre-existing health conditions.2 Firms must decide whether to grandfather their insurance plans, which limits the changes they can make to their plans, or whether to comply with the full set of new health reform requirements.
- There is a decline in the percentage of offering firms that have at least one health plan that is a grandfathered plan. Thirty-seven percent of offering firms have at least one grandfathered plan in 2014, down from 54% in 2013, 58% in 2012, and 72% in 2011.
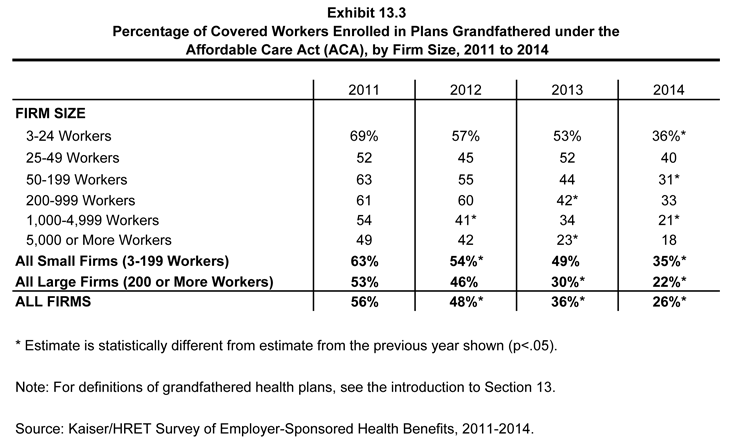
- Worker enrollment in grandfathered plans also has decreased, with 26% of covered workers enrolled in a grandfathered health plan in 2014, down from 36% in 2013, 48% in 2012 and 56% in 2011 (Exhibit 13.3).
- A similar decrease is seen by firm size. In 2014, 35% of covered workers in small firms (3-199 workers) enrolled in a grandfathered health plan, down from 49% in 2013, 54% in 2012, and 63% in 2011. For larger firms, 22% of covered workers enrolled in a grandfathered health plan, down from 30% in 2013, 46% in 2012, and 53% in 2011 (Exhibit 13.3).
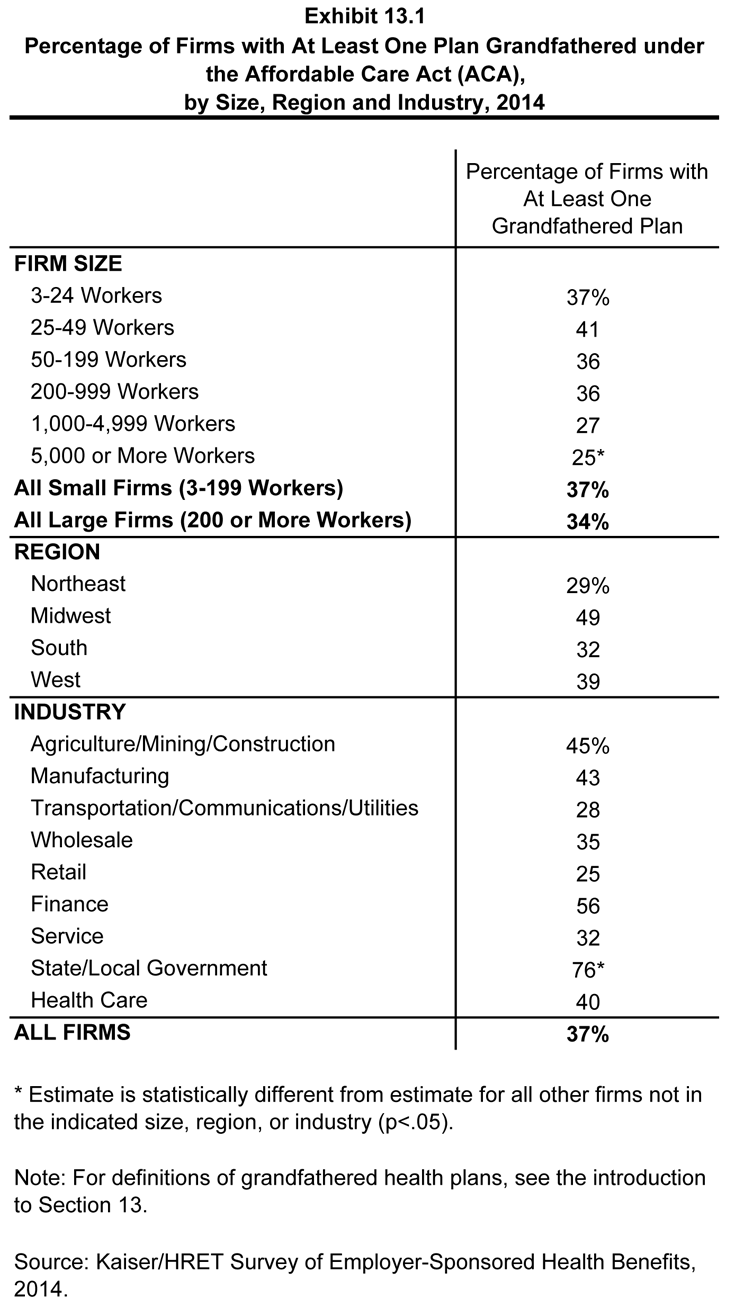
Percentage of Firms with At Least One Plan Grandfathered under the Affordable Care Act (ACA), by Size, Region and Industry, 2014
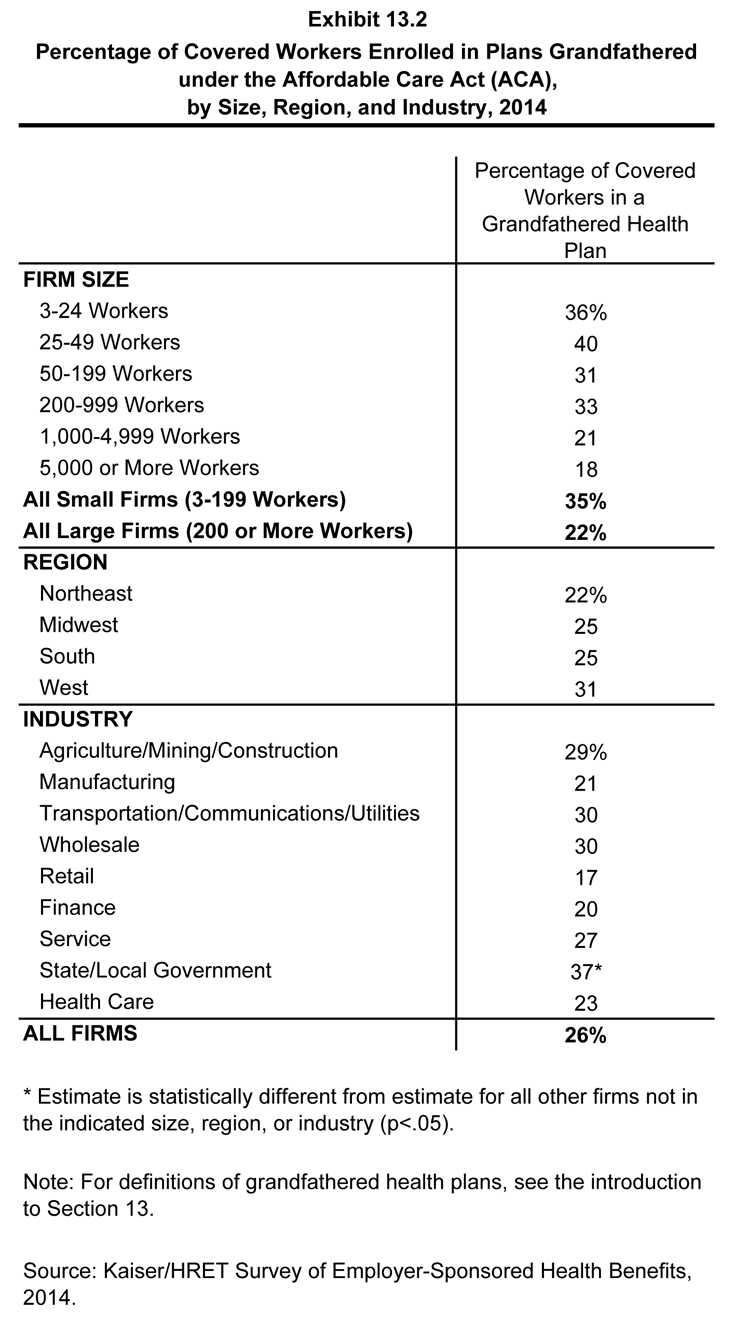
Percentage of Covered Workers Enrolled in Plans Grandfathered under the Affordable Care Act (ACA), by Size, Region, and Industry, 2014