As Pandemic-Era Policies End, Medicaid Programs Focus on Enrollee Access and Reducing Health Disparities Amid Future Uncertainties: Results from an Annual Medicaid Budget Survey for State Fiscal Years 2024 and 2025
Benefits
Context
Scope of Medicaid Benefits. State Medicaid programs must cover a comprehensive set of “mandatory” benefits, including items and services typically excluded from traditional insurance such as non-emergency medical transportation and long-term care. States may additionally cover a broad range of optional benefits defined in statute or permissible under other authorities such as Section 1115 waivers. In recent years, many state Medicaid programs have expanded their coverage of behavioral health, maternity, and dental services. States are also using Medicaid benefits to address social determinants of health (SDOH) and associated health-related social needs (HRSN) (e.g., housing, nutrition).
States may apply reasonable service limits based on medical necessity or to control utilization, but once covered, services must be “sufficient in amount, duration and scope to reasonably achieve their purpose.”1,2 There are additional benefit protections under federal statute for children and youth up to age 21.3 The Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) benefit ensures access to any medically necessary service identified in federal Medicaid statute without limitation, including optional services the state otherwise does not cover. CMS recently released updated guidance for states reinforcing EPSDT requirements and outlining strategies and best practices to strengthen children’s access and the delivery of health care services under the EPSDT benefit.
The ability to cover optional benefits and place limits on items and services results in variation across states. State Medicaid benefit design is also impacted by prevailing economic conditions: states are more likely to adopt restrictions or limit benefits during downturns and expand or restore benefits as conditions improve. States used additional federal funds and Medicaid emergency authorities made available during the COVID-19 public health emergency (PHE) to maintain or even enhance access to needed services. This year, benefit expansions far outweigh benefit restrictions and limitations, consistent with prior years. New and enhanced benefits continue to advance state priorities by expanding access to a continuum of behavioral health services, supporting improved maternal and infant health, and addressing SDOH. In some states, new benefits may be targeted to specific populations or eligibility groups, such as justice-involved individuals, at risk youth, and individuals experiencing homelessness.
This section provides information about:
- Benefit changes
- Medicaid financing of the 988 Suicide & Crisis Lifeline
- Coverage of community violence intervention or prevention services
Findings
Benefit Changes
States were asked about benefit changes implemented during FY 2024 or planned for FY 2025, excluding eligibility expansions, telehealth policy changes, and changes made to comply with federal requirements. Benefit changes may be planned at the direction of state legislatures and may require CMS approval.
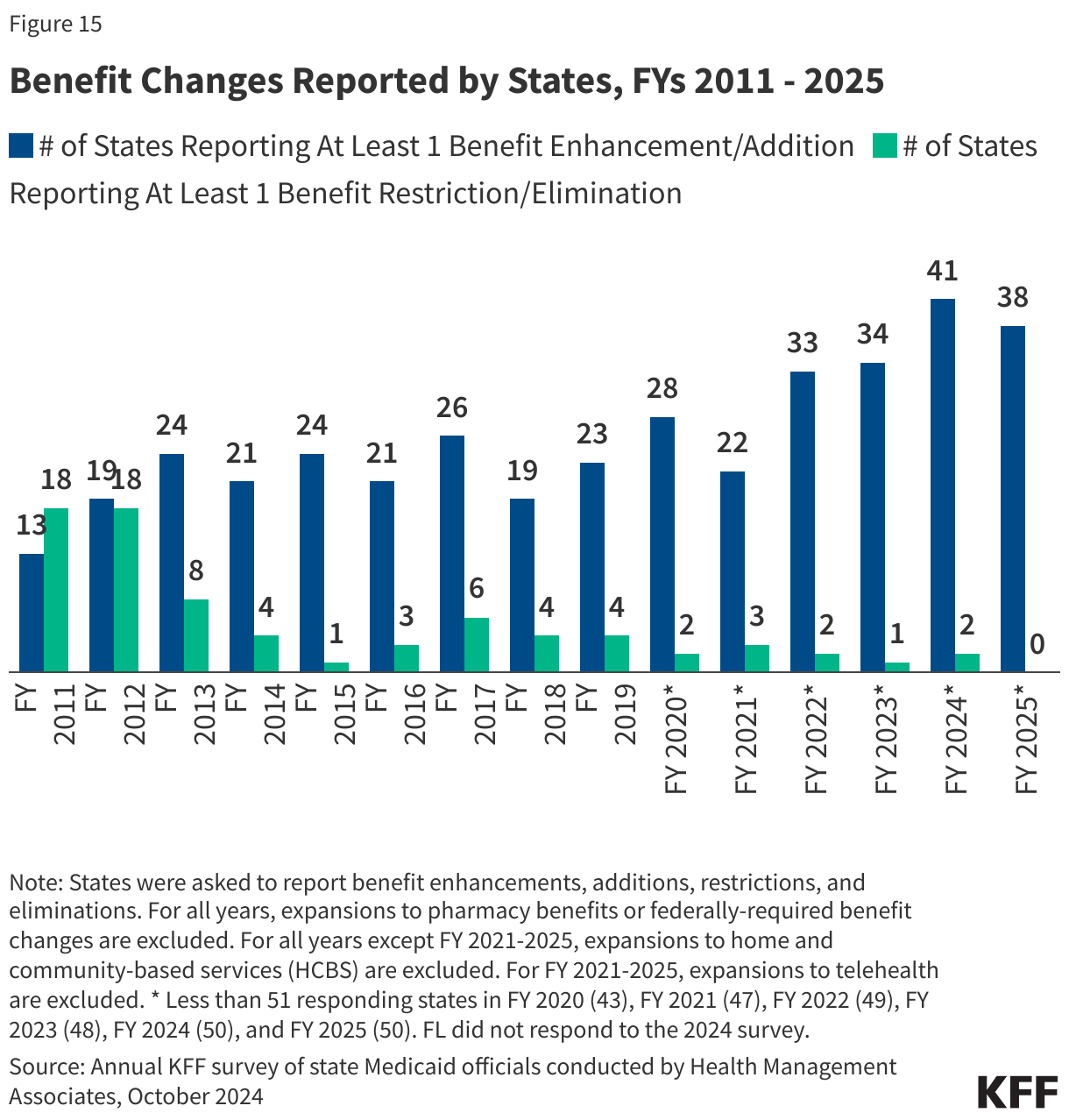
The number of states reporting new benefits and benefit enhancements continues to greatly outpace the number of states reporting benefit cuts and limitations (Figure 15 and Table 5). Forty-one states reported new or enhanced benefits in FY 2024, and 38 states reported plans to add or enhance benefits in FY 2025.4 Only two states (Nevada and Texas) reported eliminating or restricting benefits, both states taking action in FY 2024. There are additional details about benefit enhancements or additions in select benefit categories below (Figure 16).
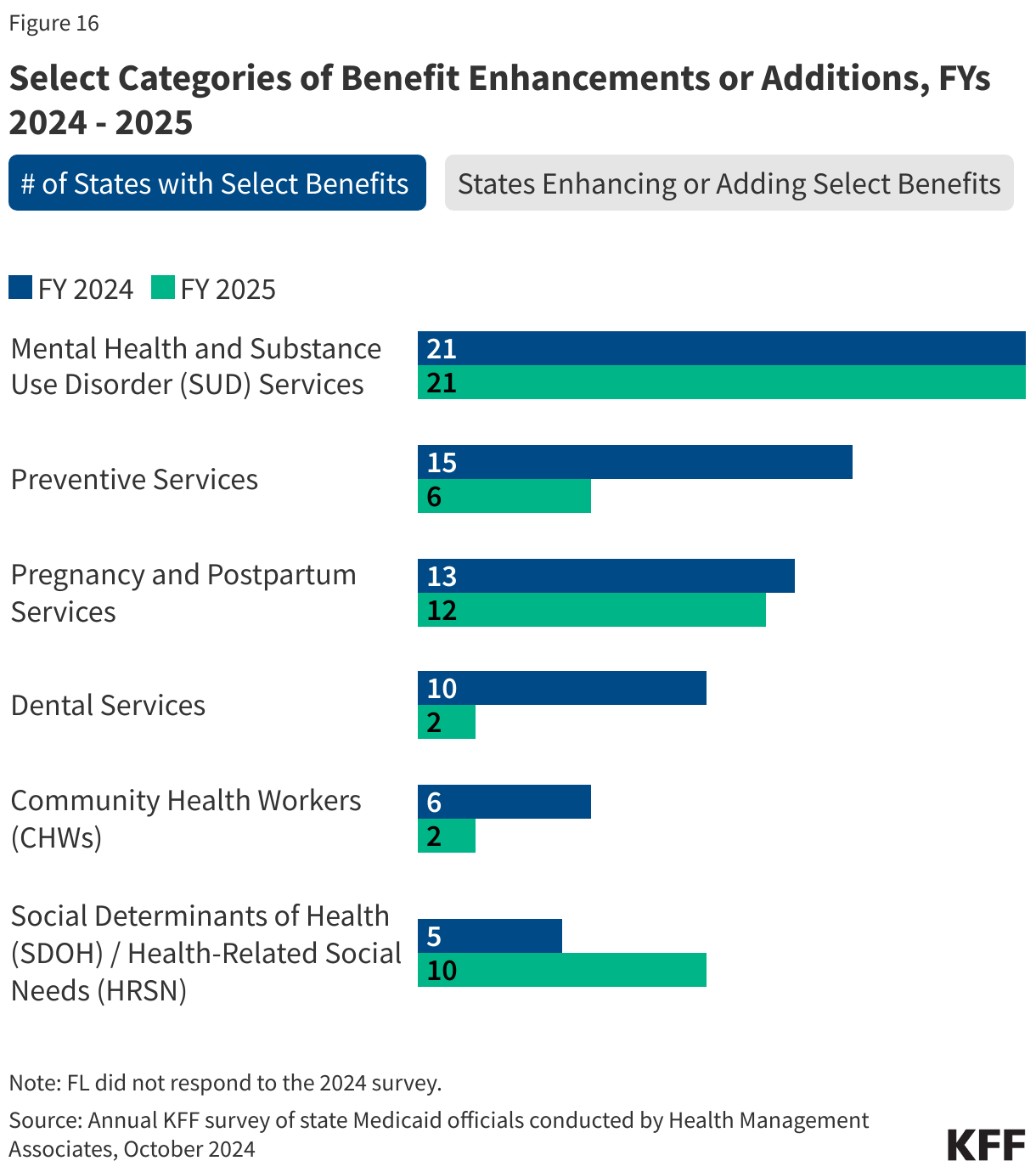
Behavioral Health Services. Behavioral health services are not a specifically defined category of Medicaid benefits. Some fall under mandatory Medicaid benefit categories (e.g., physician services). States may also cover behavioral health services through optional benefit categories (e.g., rehabilitative services). Behavioral health services for children are particularly comprehensive due to Medicaid’s EPSDT benefit for children. Mental health and substance use disorder (SUD) services continue to be one of the most frequently reported categories of benefit expansions. Consistent with trends in recent years, states reported expanding services across the behavioral health care continuum. For FY 2024 and 2025, in conjunction with the ongoing implementation of the 988 Suicide and Crisis Lifeline, there was a particular focus on enhancing crisis services and expanding the availability of other services at home and in the community. States also continue to invest in more coordinated and integrated physical and behavioral health care, including reimbursement for interprofessional consultation, adding coverage for services provided under the Collaborative Care Model (CoCM), and implementing or expanding Certified Community Behavioral Health Clinics (CCBHCs).5
- Crisis Services. At least eleven states6 reported benefit actions related to the addition or expansion of crisis services, including seven states (Louisiana, Maine, Maryland, Montana, Nebraska, New Mexico, and West Virgina) enhancing their mobile crisis response and three states (Connecticut, Louisiana, and Nebraska) adding or expanding crisis services for youth. For example, Connecticut opened and added coverage of services in Children’s Urgent Crisis Centers for children and youth experiencing a behavioral health crisis in FY 2024.
- Contingency Management. Contingency management is an evidence-based psychosocial therapy that uses incentives to motivate and reinforce behavior changes that promote recovery from stimulant use disorder and other SUDs.7 Delaware reported recent approval under a Section 1115 waiver of a 24-week contingency management program for individuals with stimulant use disorder and a 64-week program for pregnant and postpartum individuals with opioid use disorder.8 Three additional states (California, Montana, and Washington)9 have already implemented and/or received CMS approval to implement a contingency management program and at least four states (Hawaii, Michigan, Rhode Island, and West Virginia)10 have requests pending. For example, West Virginia reported a pending Section 1115 waiver request enhancing covered SUD services, including expanded peer supports, expanded secure withdrawal management and stabilization services, the addition of recovery housing and contingency management services, and implementation of quick response teams for SUD emergencies.11
- Physical and Behavioral Health Integration. Four states (District of Columbia, Maryland, Nevada and South Carolina) reported benefit actions related to Medicaid coverage of the Collaborative Care Model (CoCM), an evidence-based model integrating behavioral health into primary care through collaborative care teams that include a case manager and a psychiatric consultant. Five states (Colorado, District of Columbia, New York, Pennsylvania, and South Carolina) added reimbursement of interprofessional consultation codes, following 2023 guidance from CMS reducing barriers to payment for the consulting provider and acknowledging the important role interprofessional consultation plays in improving access to behavioral health services.
Pregnancy and Postpartum Services. Medicaid covers more than 4 in 10 births nationally and the majority of births in many states. To help reduce maternal morbidity and mortality, as well as address disparities in maternal and infant health outcomes, states continue to expand and enhance covered prenatal, delivery, and postpartum services. As reported last year, these benefit enhancements are happening alongside the extension of Medicaid postpartum coverage in many states. Fourteen states reported adding coverage of doula services in FY 2024 or FY 2025.12 Eight states reported new benefits to help parents initiate or maintain breastfeeding, including breast pumps, human donor milk, and lactation consultation.13
- South Dakota reported a new enhanced care coordination program for pregnant individuals designed to increase utilization of timely prenatal and postpartum services.14 In FY 2025, Nebraska is launching its Prenatal Plus Program for at risk pregnant individuals pursuant to LB 857, which includes nutrition counseling, psychosocial counseling and support, education and health promotion, breastfeeding support, and targeted case management.
- New Jersey is the second state in the nation implementing a statewide universal home visiting program to help improve maternal and infant health. The state’s Medicaid program is also piloting programs to provide evidence-based home visiting services for up to 500 families each year15 and medically indicated home-delivered meals for pregnant individuals with diabetes.
- Tennessee is the first state to receive CMS approval to cover diapers for the first two years of a child’s life under its TennCare 1115 waiver. Delaware also received approval under its Section 1115 waiver to expand its Postpartum Nutrition Supports Initiative pilot and cover home-delivered meals or medically appropriate food boxes, as well as a weekly supply of diapers and wipes, for 12 weeks following delivery.
- Massachusetts reported providing temporary housing assistance (up to six months) for pregnant individuals and families who are experiencing homelessness and participating in the state’s Emergency Assistance Family Shelter program.16
Preventive Services. States are required to provide comprehensive preventive care to children through the EPSDT benefit, and states must cover certain preventive services for adults eligible under the ACA’s Medicaid expansion; however, this coverage is not required for “traditional” Medicaid adults. In this year’s survey, states reported benefit actions related to testing, screenings, vaccinations,17 and contraceptives. Some states also report expanding access to preventive services by newly adding coverage of pharmacist services allowable under their scope of practice (Illinois, Pennsylvania, Wisconsin, and Wyoming) and adding local health departments to providers that may be reimbursed for screenings and other services (Texas).
- Two states reported covering at home testing and screening services. Pennsylvania added coverage of at home sexually transmitted infection (STI) test kits. Wyoming added coverage of Cologuard® at home colorectal screening tests to help increase colorectal cancer screening rates.
- Three states (Louisiana, Mississippi, and New Hampshire) reported addition or expansion of smoking cessation counseling services beyond required benefits and covered populations.
Services Targeting Social Determinants of Health (SDOH). Outside of Medicaid home and community-based services programs, state Medicaid programs have more limited flexibility to address enrollee social needs (e.g., housing, food, transportation, etc.). Certain options exist under Medicaid State Plan authority as well as Section 1115 waiver authority to add non-clinical benefits. In 2022, CMS released a new framework for covering health-related social needs (HRSN) services under Section 1115 waivers, expanding flexibility for states to add certain short-term housing and nutrition supports as Medicaid benefits (building on CMS guidance from 2021). Additional guidance and resources that identify allowable HRSN services and supports were released by CMS in late 2023. In this year’s survey, states continued to report services targeting SDOH, including housing services and supports, nutrition services, and medical respite.
- CMS has approved ten states (Arizona, Arkansas, California, Illinois, Massachusetts, New Jersey, New Mexico, New York, Oregon, and Washington) under the new HRSN Section 1115 framework. States continue to seek approval for SDOH-related services in and outside of this framework. Of note in this year’s survey, at least three states (California, District of Columbia, and Hawaii) reported pending Section 1115 waiver requests to provide short-term rental assistance, utilities assistance, and/or temporary housing in addition to other housing services and supports.
- Eight states (District of Columbia, Hawaii, Kentucky, Massachusetts, Michigan,18 Minnesota, Nebraska, and Utah) reported plans to add coverage of medical respite services (also known as recuperative care or pre-procedure/post-hospitalization housing) in FY 2024 or later. This intervention includes room and board and clinically oriented services and supports19 to provide a safe and stable environment before a procedure or following an inpatient discharge for individuals experiencing homelessness. State activity to cover this benefit continues.20
Community Health Workers. Eight states (Kansas, Michigan, Nevada, New Jersey, New Mexico, New York, Oklahoma, and Pennsylvania) added or expanded coverage of services provided by Community Health Workers (CHWs) in FY 2024 or FY 2025, continuing a trend observed in Medicaid programs in recent years. Services provided by CHWs may include culturally appropriate health promotion and education, care coordination, and help accessing medical and non-medical services.
- New York reported adding coverage of CHW services for children, pregnant and postpartum individuals, and other high-risk enrollees in FY 2024.21 New Mexico’s CHW benefit includes services provided by CHWs or Community Health Representatives (CHR) trained under the Indian Health Service (IHS).22
Dental Services. While EPSDT requires states to provide comprehensive dental services for children, states are not required to provide dental benefits to adults. States may choose to provide dental coverage for adults, and with increasing frequency, are expanding coverage from limited (e.g., extractions or emergency services) to more comprehensive (e.g., diagnostic, preventive, and restorative services). Following adult dental benefit expansions in several states reported in recent surveys, benefit actions related to dental services in FY 2024 and FY 2025 are more nuanced. Examples include but are not limited to adding select periodontal services (Connecticut), dentures and partial dentures (Kansas), adult oral examinations (Missouri), and Silver Diamine Fluoride (SDF)/interim caries arresting medicament application for children and targeted adult populations (Missouri and Texas). Texas reported narrow restrictions on dental benefits in FY 2024, impacting coverage of topical fluoride treatment and space maintainers.
- Georgia is expanding its adult dental benefit in FY 2025 to include diagnostic, preventive, restorative, periodontal, prosthodontic, orthodontic, endodontic, emergency dental services, and oral surgery.23 Nebraska reported removing the annual adult benefit cap ($750) in FY 202424 and Vermont eliminated the annual dental benefit cap for certain adult populations in FY 2024.25
Other State Benefit Actions. In this year’s survey, several states reported expanding other optional benefits covered by their Medicaid programs. Three states (New Mexico, Rhode Island, and Washington) reported adding chiropractic services, one state (Wyoming) reported adding podiatry services, and one state (Washington) reported adding acupuncture services.
- Palliative Care. Hawaii and New Jersey reported adding a community palliative care benefit in FY 2024 or FY 2025 to prevent and provide relief from symptoms and stress of serious illness and improve enrollees’ quality of life. Illinois reported introducing a pediatric palliative care benefit in FY 2024.
- School-based services. Schools can be a key setting for providing services to Medicaid-covered children. Seven states (Alaska, Maine, Maryland, New York, Ohio, Oklahoma, and Rhode Island) report expanding their school-based services programs. Examples include adding services (e.g., outpatient therapy, psychological testing, early intervention), provider types (e.g., school psychologists), or populations served. For example, a few states are extending services to children who do not have an Individualized Education Program (IEP) or Individualized Family Service Plan (IFSP).
Box 2: Section 1115 Medicaid Reentry Waivers
In April 2023, CMS released guidance encouraging states to apply for a new Section 1115 demonstration opportunity to test transition-related strategies to support community reentry and care transitions for individuals who are incarcerated. This opportunity allows states to partially waive the statutory Medicaid inmate exclusion policy, which prohibits Medicaid from paying for services provided during incarceration (except for inpatient services). As of October 2024, eleven states have approval to provide pre-release services and 15 additional states (including DC) have pending pre-release waivers under review at CMS. In July 2024, CMS announced it had developed a standard demonstration application and special terms and conditions to expedite the review and approval of reentry waiver requests (approving 7 reentry waivers in July). States with governors across political parties have pursued these waivers. California will be the first state to implement its reentry demonstration in October 2024 (after gaining approval in January 2023).
Starting January 1, 2025, the 2023 Consolidated Appropriations Act (CAA) requires Medicaid and CHIP to cover screenings (medical, dental, and behavioral health), diagnostic services, and case management for all eligible youth (under age 21 and former foster care youth under age 26) in public institutions (including state prisons, local jails, tribal jails and prisons, and all juvenile detention and youth correctional facilities) 30 days prior to release. States must continue to provide case management services for at least 30 days post-release. The 2023 CAA also gives states an option to provide full Medicaid or CHIP services to all youth (under age 21 and former foster care youth under age 26) in public institutions pending disposition of charges (i.e., awaiting the outcome of charges).
988 Suicide & Crisis Lifeline
On July 16, 2022, the federally mandated crisis number, 988, became available to all landline and cell phone users at no charge. This three-digit number provides 24/7 access to crisis counselors for everyone, regardless of financial ability. Insurer payments can help financially sustain 988 and other crisis services, and some states bill Medicaid. Recent CMS guidance confirms Medicaid administrative match, including enhanced federal matching rates for health IT costs, is available to support 988 operations such as establishing or improving local call centers, system integration, and information exchange. This year’s survey asked states whether Medicaid supported administration of the 988 hotline or paid for 988 services delivered to Medicaid beneficiaries.
A handful of states reported using Medicaid funding to support and sustain the 988 Suicide & Crisis Lifeline as of July 1, 2024. Four states (Georgia, Indiana, Michigan, and Utah) reported using Medicaid administrative funds to support hotline operations, and an additional three states (Idaho, West Virginia, and Wyoming) plan to do so in FY 2025. Seven states (Arizona, Colorado, Georgia, Indiana, Michigan, New Mexico, and West Virginia) reported using Medicaid funds to pay for hotline services provided to individual Medicaid enrollees and two (Idaho and Wyoming) additional states plan to do so in FY 2025. Some states explained that 988 hotline administration was fully covered by SAMHSA grants and other funding, and a few states noted that insurance or other identifying information is not collected, making it challenging to bill Medicaid.
Medicaid Coverage of Community Violence Intervention Services
Community violence intervention services are multi-disciplinary, community-based strategies for individuals and groups at risk of participating in or being a victim of gun violence. They may provide safety planning, conflict intervention, trauma-informed care, a connection to social services, and other interventions to reduce the likelihood of future violence. In 2021, the Biden-Harris Administration announced an investment in community violence intervention programs, including Medicaid funding. More recently, the administration announced additional clarifying guidance on Medicaid reimbursement for violence intervention programs, as well as counseling on firearm safety, is forthcoming. This year’s survey asked states if they have in place a Medicaid-funded State Plan community violence intervention or community violence prevention benefit.
Six responding states reported covering community violence intervention or community violence prevention services in Medicaid as of July 1, 2024. These states are California, Connecticut, Illinois, Maryland, New York, and Oregon. Service definitions, delivery model, and provider qualifications vary across the states, but commonly include evidence-based, trauma-informed education and services to promote recovery, support behavior change, and prevent future injury or violence. States generally cover these services when provided by certified violence prevention professionals following an individual assessment, but two states (California and New York) cover violence prevention services as a CHW service. Illinois’ Reimagine Public Safety Act created Violence Prevention Community Support Teams to provide peer supports, therapy and counseling, and community support, including at an enrollees’ home or school. At least one state (Connecticut) noted low utilization despite covering the benefit since 2022.
