States Obtain Special Waivers to Help Unwinding Efforts
This policy watch was updated on Jan. 16, 2024 to reflect ongoing policy changes.
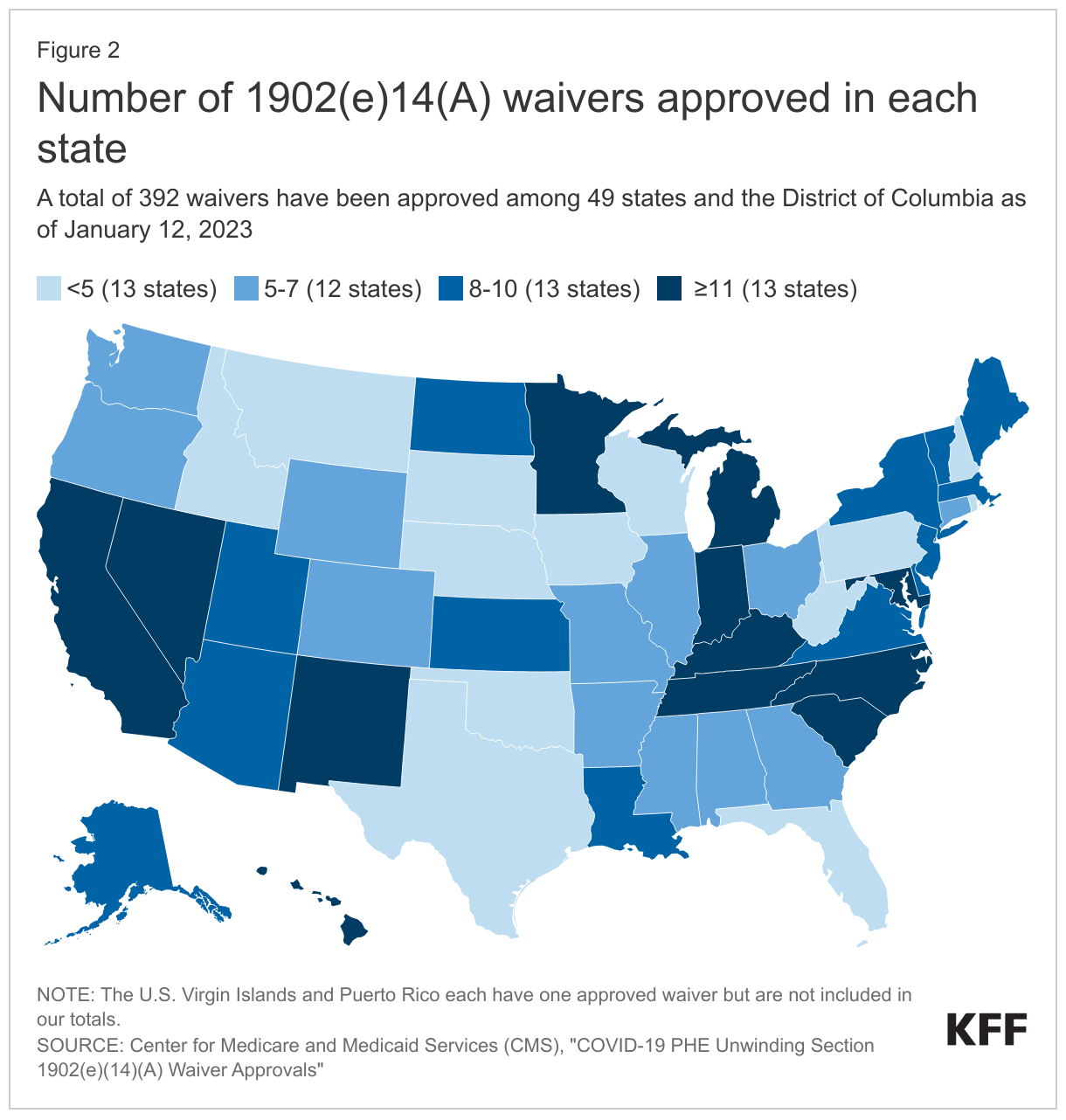
As states unwind the continuous enrollment provision and complete redeterminations for all Medicaid enrollees, they face numerous challenges including staffing shortages and outdated systems. More than six months into the unwinding of the continuous enrollment provision, over 14 million individuals have been disenrolled with 71% due to procedural reasons. To give states additional tools to comply with federal renewal requirements, the Centers for Medicare and Medicaid Services (CMS) identified a range of strategies, including the availability of temporary waivers under section 1902(e)(14)(A) of the Social Security Act. Nearly all states adopted one or more of these temporary waivers. As of January 12, 2023, CMS had approved a total of 392 waivers for 49 states and the District of Columbia. At the end of December 2023, growing concern over loss of Medicaid coverage for children prompted federal officials to issue new data showing that adoption of waiver flexibilities influences renewal outcomes for children and additional guidance highlighting strategies to reduce procedural disenrollments. The guidance included an announcement that the waivers will be extended to be available through the end of 2024 (unless approved for a longer duration) instead of being tied to the unwinding period. The Secretary of HHS also sent letters to nine states with large declines in Medicaid child enrollment, urging them to take up additional policy options to prevent disenrollments due to paperwork or procedural issues.
How are states using unwinding waivers?
CMS groups available “1902(e)(14)(A)” waivers into four buckets: options to increase ex parte renewals, supporting enrollees in completing and submitting renewal forms, updating enrollee contact information, and facilitating reenrollment for individuals disenrolled for procedural terminations. States can also request authority to adopt additional strategies to protect enrollees during the unwinding; these waivers are counted in the Other category but discussed in the bucket where the strategy fits in best.
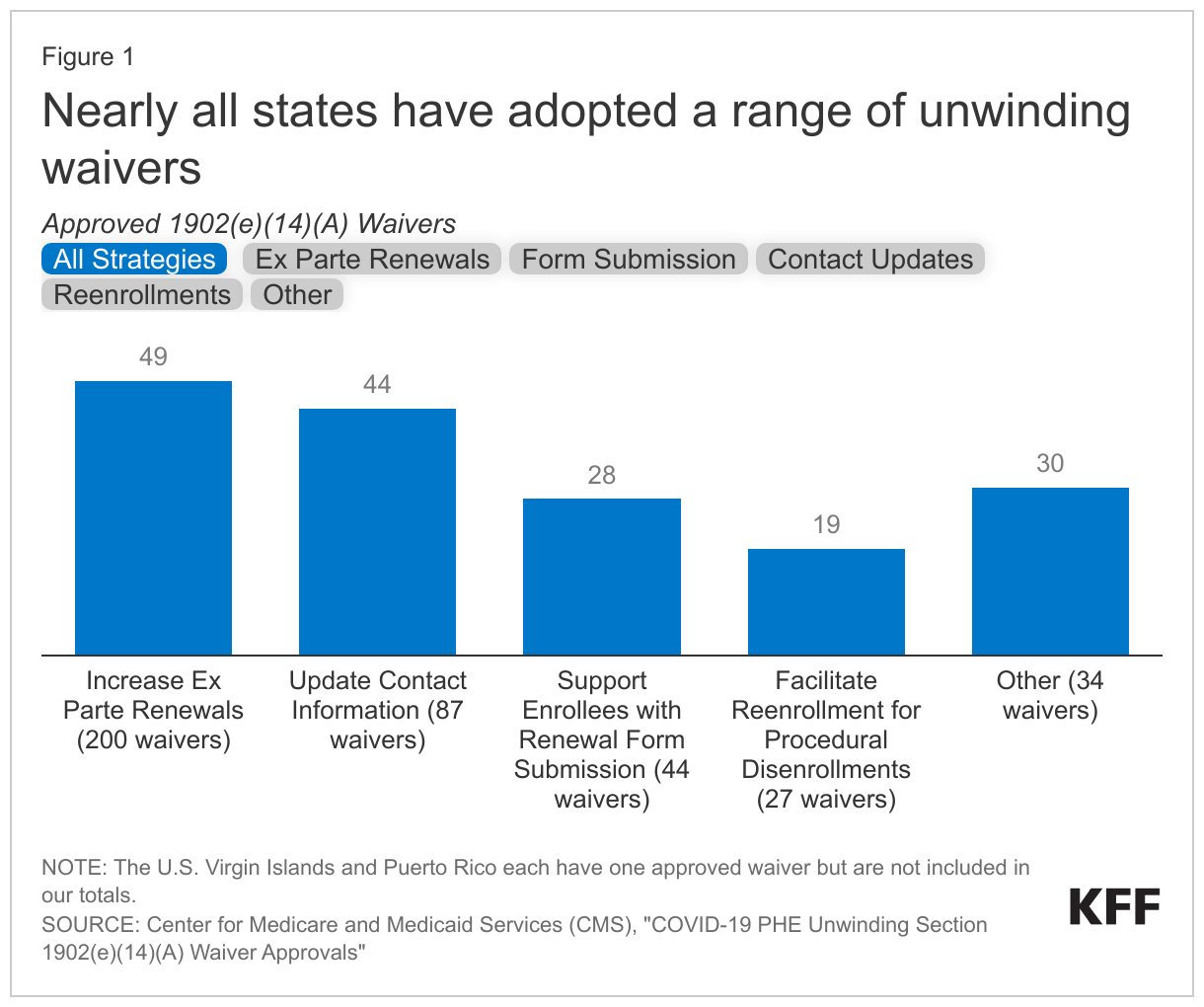
- Nearly all states (49) have approved waivers to help increase ex parte rates. Ex parte renewals work by eliminating the need for enrollees to submit renewal forms. Instead, state Medicaid staff use administrative data on income and other circumstances to determine eligibility. Of states with waivers in this category, 38 adopted waivers to allow for ex parte renewals for individuals with no income and /or income at or below 100% of the federal poverty level (FPL). Under this option, CMS allows an ex parte renewal if the most recent income determination was no earlier than March 2019 and the state has checked financial data sources and no information is received; without the waiver states would need to conduct new data matches or otherwise document that an individual has no or low-income. Thirty-three states have waivers to allow the state to assume no change in assets if there is no information returned through the asset verification systems or to allow states to renew eligibility based on a simplified asset verification process. More than half of states (27) have waivers to use Supplemental Nutrition Assistance Program (SNAP) or Temporary Assistance for Needy Families (TANF) eligibility to confirm ongoing Medicaid eligibility. Other approved waivers in this category include the use of Title II disability income data, suspending requirements to apply for other benefits, and requiring manual ex parte reviews before terminating coverage.
- Forty-four states have waivers to update enrollee contact information. Updating contact information is an important step to ensure that renewal forms are sent to the correct addresses. States can obtain updated contact information from the National Change of Address (NCOA) and/or USPS returned mail databases (37 states), MCOs (32 states), enrollment brokers who aid beneficiaries in enrollment (six states), or Programs of All-Inclusive Care for the Elderly (PACE) (six states). Five states have waivers allowing states to obtain contact information from other sources, including Qualified Health Plans and a state-designated Health Information Exchange.
- Twenty-eight states have waivers to help enrollees complete and submit renewal forms. Twenty-one states have waivers that allow managed care organizations (MCOs) to help enrollees complete sections of their renewal forms, beyond sections relating to managed care plan selection. Eleven states have waivers that permit applicants and enrollees to designate an authorized representative over the phone without requiring a signed designation. This phone designation enables assisters and others who are helping enrollees complete renewals by phone to provide timely support without waiting for signed documents. Eleven states have flexibilities to waive the recording of telephonic enrollee signatures. One state (Alaska) has a waiver permitting the use of a simplified renewal form.
- A total of 19 states have waivers to help individuals re-enroll if they were disenrolled for procedural reasons. Seventeen waivers have been approved to reinstate coverage from the date of termination for individuals who were disenrolled for procedural reasons but later found to be eligible. This ensures that any health care services obtained after individuals were disenrolled are covered. Ten states obtained waivers to extend automatic reenrollment into an MCO plan from the standard 60 days up to 120 days. Twenty-four states have waivers to extend the amount of time to take final actions on fair hearing requests beyond the standard 90 days, and two states have other waivers that relate to fair hearing strategies (these are included in the other category). CMS allows waivers to designate state agencies or community organizations, pharmacies, and providers as qualified entities to determine presumptive eligibility for MAGI enrollees who were disenrolled for procedural reasons. However, no states have obtained either of these waivers yet.
- States vary widely in their use of 1902(e)(14)(A) waivers, ranging from 15 in Indiana and Tennessee to 0 in Florida. There may be several reasons for this variation in uptake related to differences in how state eligibility systems function, the need to address compliance issues, interest in maintaining coverage, and more.
What are the key issues to watch?
During the unwinding period, CMS has issued guidance on how to mitigate procedural disenrollments using multiple strategies. Data suggests that states that have taken advantage of unwinding flexibilities have reduced procedural terminations and kept more eligible children enrolled. On December 18, 2023 CMS sent letters to the nine states with the highest child disenrollment rates and encouraged them to adopt additional flexibilities to maintain coverage for eligible children, including 1902(e)(14)(A) waivers. CMS also announced that unwinding waivers will remain in effect until at least the end of 2024 and that states can request new waivers up until that point.
Efforts to improve renewal processes and reduce procedural disenrollments will likely last beyond the unwinding period, and CMS and states may look to extend some unwinding flexibilities and/or make some permanent for regular operations. A KFF brief based on interviews with state officials and others in four states provides insights into which waivers have been most effective at achieving the goals of increasing ex parte renewal rates, updating contact information, and reducing administrative burden. Input from these and other states can help to inform CMS decisions over whether to maintain some waiver options.