New OIG Report Examines Prior Authorization Denials in Medicaid MCOs
Medicaid managed care organizations (MCOs) deliver care to more than two-thirds of all Medicaid enrollees nationally. Managed care plans often require patients to obtain approval of certain health care services or medications before the care is provided—an insurance practice commonly referred to as “prior authorization” (or PA). This allows the health plan to evaluate whether care is covered and medically necessary. If the health plan determines the requested service (or medication) isn’t appropriate or medically necessary, they may deny the request (fully or partially). While Medicaid MCOs may limit services based on medical necessity or utilization management tools (e.g., prior authorization), federal rules specify services must be no less (in amount, duration, and scope) than offered under fee-for-service and MCOs cannot arbitrarily deny or reduce a required service based solely on an enrollee’s illness or condition.
A recent KFF survey of consumer experiences with health insurance found that about one in five Medicaid enrollees say they’ve had issues with prior authorization—higher than for most other types of insurance–and close to a quarter said that their health got worse because of this or another insurance problem. Doctors have indicated that prior authorization can delay care and can result in negative clinical outcomes. To better understand the implications of prior authorization policies, Congress asked the U.S. Department of Health and Human Services (HHS) Office of Inspector General (OIG) to investigate whether Medicaid MCOs are providing medically necessary health care services to their enrollees. OIG gathered data about prior authorization denials for 2019 from the 7 biggest “parent” MCO companies (representing 115 comprehensive Medicaid MCO plans in 37 states and about 29 million enrollees (or 57% of MCO enrollees in these states)). OIG also surveyed state Medicaid officials about oversight of prior authorization denials and appeals.
What are rates of Medicaid managed care prior authorization denials?
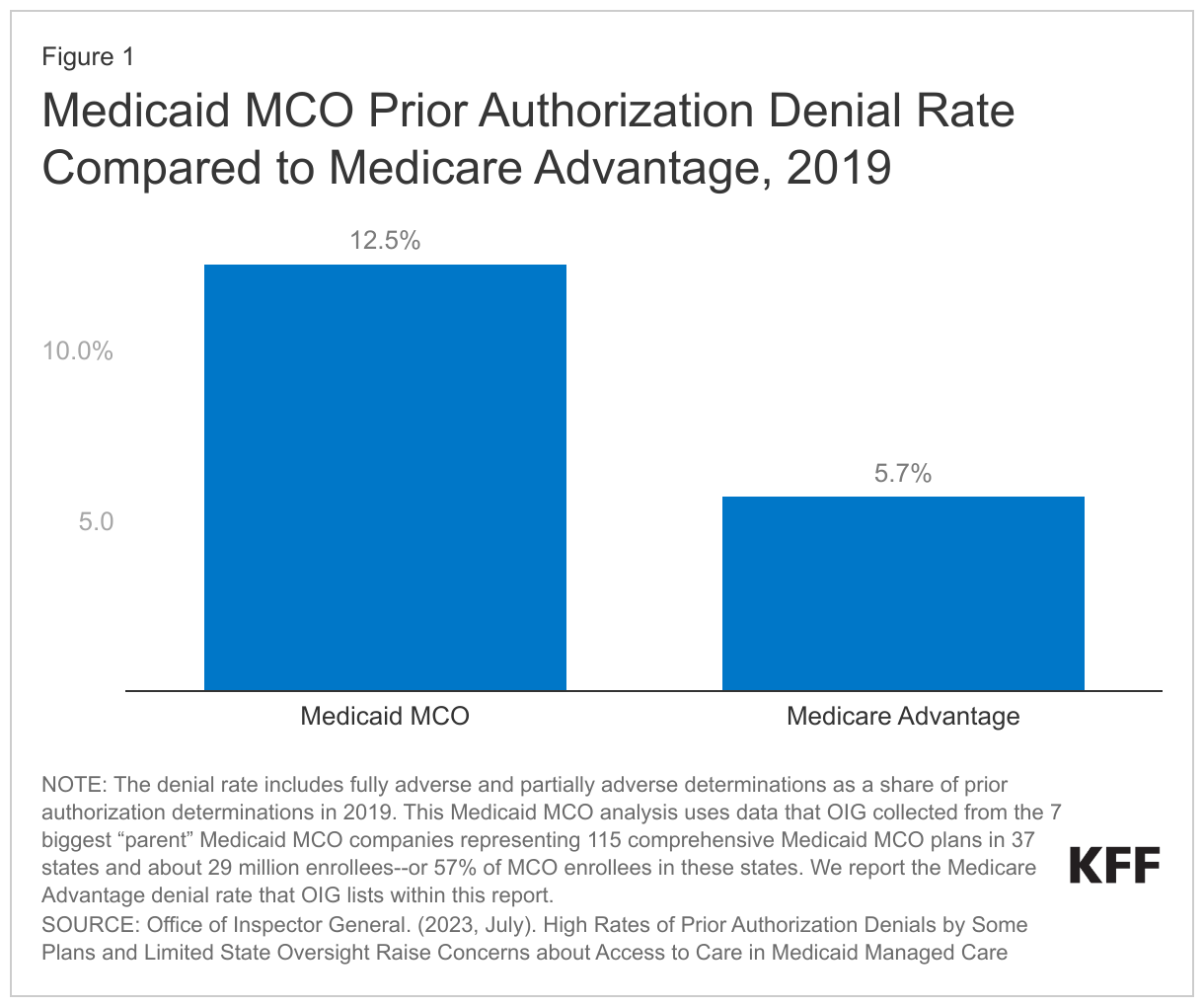
OIG found that Medicaid MCOs had an overall prior authorization denial rate of 12.5%–more than 2 times higher than the Medicare Advantage rate (Figure 1). In 2019, the Medicaid MCOs included in the OIG review requested over 17 million prior authorizations. Medicaid MCOs denied (fully or partially) over 2.2 million of these requests, meaning they rejected (full or partially) about 1 in 8 or 12.5% of the prior authorization requests. The overall prior authorization denial rate is more than two times higher than the Medicare Advantage denial rate—at 5.7%.
Prior authorization denial rates ranged widely across and within parent firms and states. For example, the parent firm, Molina, had individual MCOs with denial rates that ranged from 7% to 41%. Parent firms included in the OIG review operated from 3 (CareSource) to 33 (Centene) individual MCOs.

What happens after a Medicaid prior authorization denial?
After a prior authorization request is denied, Medicaid enrollees can appeal, but it’s not always straightforward and many appeals don’t change the initial decision. Enrollees or providers who disagree with the MCO’s prior authorization decision have a right to appeal to the MCO for reconsideration. If an MCO upholds its initial denial, enrollees have a right to request a state fair hearing. However, the OIG review found most (89%) Medicaid enrollees do not appeal to the MCO for reconsideration, perhaps because they don’t know that they can, which aligns with findings from KFF’s survey of consumer experiences with health insurance. Of the few who do appeal, only about one-third get the initial denial overturned—far less than for Medicare Advantage appeals (Figure 3). Further, the OIG review found that of the prior authorization denials that MCOs upheld, only 2% were appealed to a state fair hearing—perhaps due to lack of awareness and/or complicated process.

Unlike in Medicare Advantage, if a Medicaid MCO upholds its original denial, there is no automatic, independent external medical review. In both Medicaid and Medicare Advantage, the first step for enrollees who receive a prior authorization denial (and wish to pursue it further) is to appeal to the managed care plan for reconsideration. In Medicare Advantage, if the managed care plan upholds the original denial, the case is automatically sent to an independent review entity. In Medicaid, states may offer an external review option, but most don’t. (Even in the states that offer external medical reviews, OIG found limited use of these reviews.) OIG suggests that this automatic independent review process might help explain why Medicare Advantage’s appeal overturn rate is 82%–far higher than Medicaid MCOs.
OIG found that state Medicaid agency oversight of prior authorization denials is limited. States are not federally required to conduct oversight of MCO denials (e.g., monitoring denial rates or reasons for denial, monitoring outcomes of appeals, or auditing denials to assess whether they are clinically appropriate). OIG found that most states either don’t regularly check denial decisions for clinical appropriateness (i.e., to see if denials follow state’s coverage and medical necessity rules) or only check when they feel it is necessary (“ad hoc”) (e.g., in response to specific disputes, provider complaints etc.) (Figure 4). OIG also reported that while 22 states collect MCO denials data to keep an eye on MCO prior authorization decisions,15 states don’t collect denials data for oversight (data not shown).

What are key issues to watch?
The OIG report underscores concerns about prior authorization and access in Medicaid managed care, keeping this issue at the forefront of ongoing policy discussions. While prior authorizations can help manage health care utilization, denials can create barriers to receiving care, cause delays, affect patient health, and may exacerbate health disparities. OIG suggests that the wide variation in denial rates might be due to varying policies or how they’re carried out. They recommend adding denials and appeals processes that are similar to Medicare Advantage, including stronger state monitoring of denials and a requirement for automatic external medical reviews following MCO appeal denials. In addition to proposed rules to improve access to care in Medicaid managed care, CMS has separately proposed rules around prior authorizations, but these rules mostly focus on streamlining process, reducing approval wait times, and improving transparency.