What to Know Ahead of the Supreme Court Case on Youth Access to Gender Affirming Care
Background
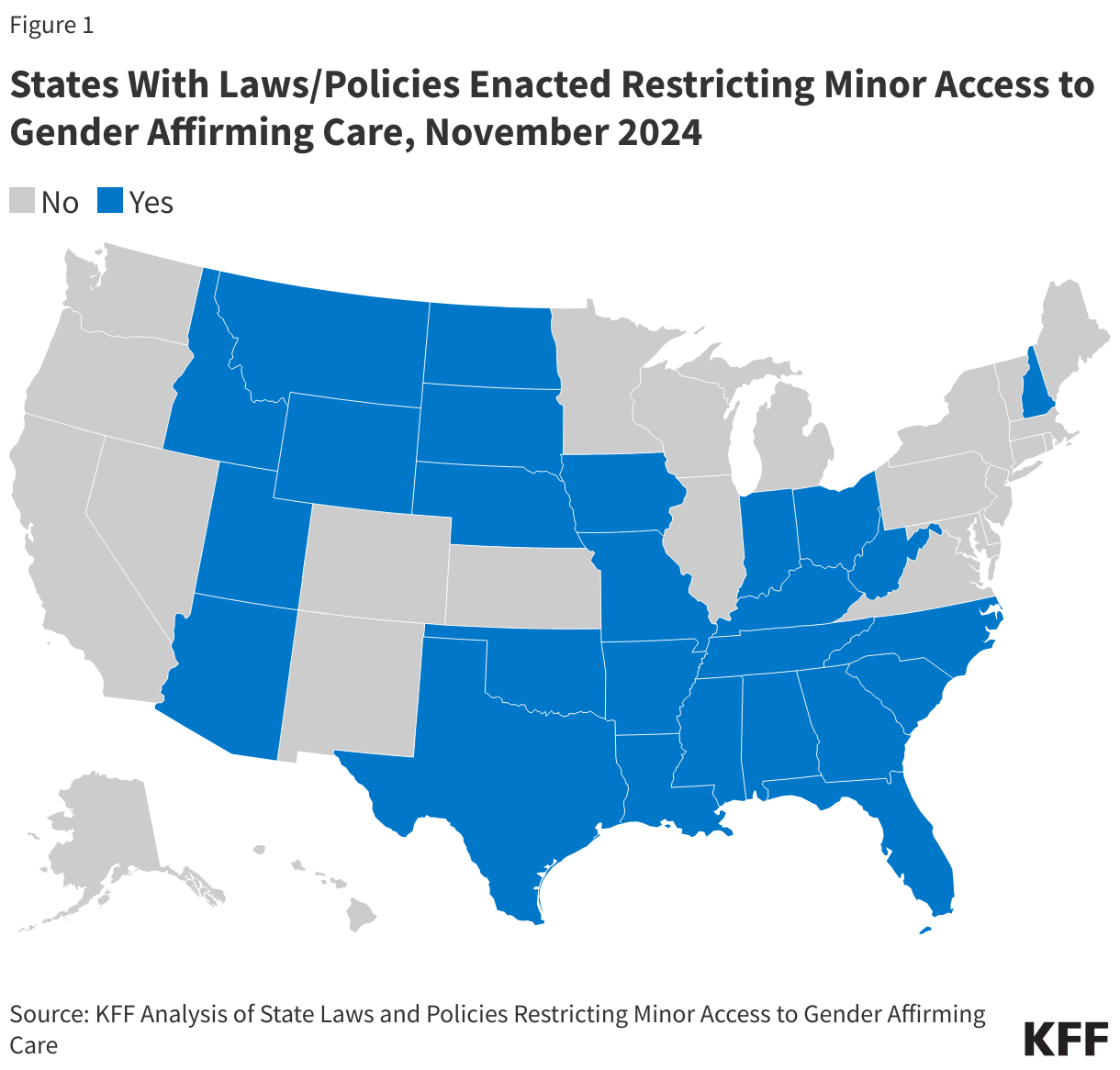
Youth access to gender affirming care has become an increasingly politicized and contentious issue in recent years. Today, 26 states have enacted laws restricting youth access to gender affirming care, most of which are facing legal challenges. On December 4th, the Supreme Court will hear a case challenging the constitutionality of such state restrictions for the first time. The case before the Supreme Court challenges the Tennessee ban (United States v. Skrmetti) under the Equal Protection Clause of the 14th Amendment. Both the plaintiffs, three families and a provider, who originally challenged the law (L. W. et al v. Skrmetti et al) and the Biden administration, as an intervener, requested review and the Court granted certiorari in the challenge brought by the Biden administration.
The case has garnered significant attention with 84 amicus briefs having been filed, 32 in support of the petitioners, 51 in support of the respondents, and one in support of neither party. Amicus briefs in support of the petitioner include those from The American Academy of Pediatrics, The American Psychological Association, and the State of California with 19 other states, among others. Briefs filed in support of the respondents include those from the State of Kentucky with 21 other states, The Alliance Defending Freedom, and the Family Research Council, among others.
This brief provides background on gender affirming care and state bans, explains the legal challenge to the Tennessee law, and explores the potential Court ruling and impact on access across the country.
What is gender affirming care?
Gender-affirming care is a model of care which includes a spectrum of “medical, surgical, mental health, and non-medical services for transgender and nonbinary people” aimed at affirming and supporting an individual’s gender identity. Gender affirmation is highly individualized. Not all trans people seek the same types of gender affirming care or services and some people choose not to use medical services as a part of their transition.
Gender affirming medical care is a medically necessary evidence-based system of care that is supported by virtually all major U.S. medical associations. Decision making related to gender affirming care is a slow thoughtful process typically involving a team of providers, the patient, and in the case of minors, parents.
Among those who do seek medical care as a part of their transition, common services include puberty blockers, which temporarily delays puberty to allow a young person additional decision-making time, and hormone therapy, which enables individuals to develop physical traits that align with their gender identity. Surgeries are also sometimes a part of care but are relatively uncommon among adults and very rare among minors.
Research has found that adolescents with gender dysphoria who are denied access to medically necessary gender affirming care are at increased risk for significant behavioral health challenges including depression, eating disorders, substance use, self-harm, and suicidality.
What is the status of minor access to gender affirming care in the United States?
Access to gender affirming care for youth has been increasingly limited in the U.S. Arkansas became the first state to enact a youth gender affirming care ban in April 2021, with Arizona and Alabama following about a year later. Beginning in January 2023, the number of states enacting these policies rapidly proliferated and by August, it had reached 22 – a seven-fold increase in an eight-month period. As of November 2024, 26 states have such restrictions. While these laws mainly impact youth access to health care, some impact adult access too, and a majority of the laws include professional and/or civil penalties for health care practitioners who provide gender affirming care. Additionally, legal challenges are piling up, and laws in 17 of the 26 states are being challenged in court. The majority of cases are filed in federal courts and most have reached appellate courts. Like the Tennessee case before the Supreme Court, most other cases also challenge state laws on 14th Amendment Equal Protection grounds, though other grounds are common as well. All of the cases filed in federal court that bring 14th Amendment Equal Protection claims, also bring 14th Amendment Due Process claims, largely focused on parental autonomy rights (i.e., the rights of parents to make decisions for their children). In some cases, alternate grounds are tied to provisions specific to an individual state’s law (e.g., if the state law includes provisions restricting gender affirming care in Medicaid) and some cases filed in state courts base claims on violation of state constitutional provisions.
What are the key provisions in the Tennessee law (SB1)?
Tennessee law SB1 is the law prohibiting minor access to gender affirming care in the state that is being challenged at the Supreme Court. It was enacted on March 22, 2022, became effective July 1, 2023, and includes the following provisions:
- Prohibits health care providers from providing or offering gender affirming care — including puberty blockers, hormone therapy, and surgery — to minors. Additionally, “any person” is prohibited from providing puberty blockers or hormone prescriptions. The prohibition is inclusive of care provided via telehealth.
- Providers violating SB1 are subject to discipline under Title 63 of TN code regulating health professionals (class B misdemeanor).
- Creates a private right of action for minors/parents (when consent was not given) and outlines direct enforcement authority for the attorney general (regardless of consent given). Provides right to wrongful death action specifically when a minor’s death results from physical or emotional harm and there was no consent from parents.
- As with all states with similar restrictions, provides an exclusion for care “to treat a minor’s congenital defect, precocious puberty, disease, or physical injury” unrelated to gender affirming care.
- Provided a temporary period for minors to continue receiving care if they were already receiving prohibited care prior to the law’s enactment through March 31, 2024.
What happened with the case in the lower courts?
In the Spring of 2023, prior to the law’s effective date, three families and a provider challenged SB1 in federal court (U.S. District Court for the Middle District of Tennessee) on multiple grounds, including for violating the 14th Amendment Equal Protection Clause. The U.S. Department of Justice (DOJ) intervened in the case in support of the plaintiffs. The District Court granted in part and denied in part the plaintiffs request for a preliminary injunction, allowing minors in the state to retain access to gender affirming hormones and puberty blockers, but allowing the part of the law blocking surgeries and creating a right of action to be implemented. The state appealed the injunction to the 6th Circuit Court of Appeals and the appellate court reversed and remanded the District Court’s preliminary injunction, reinstating the ban in Tennessee (as well as the ban in Kentucky). In November 2023, both the plaintiffs and the US DOJ petitioned the Supreme Court to review their case. (As noted above, the Supreme Court took the case based on the DOJ request.)
What is before the Supreme Court?
While the plaintiffs raised several legal theories in the original filing, the Supreme Court will only be reviewing one question:
“Whether Tennessee Senate Bill 1 (SB1), which prohibits all medical treatments intended to allow “a minor to identify with, or live as, a purported identity inconsistent with the minor’s sex” or to treat “purported discomfort or distress from a discordance between the minor’s sex and asserted identity,” Tenn. Code Ann. § 68-33-103(a)(1), violates the Equal Protection Clause of the Fourteenth Amendment.” (Emphasis added.)
The U.S. government contends that the Tennessee’s law violates the 14th Amendment’s Equal Protections Clause because the law explicitly classifies minors based on sex and discriminates based on transgender status. The law prohibits treatment to minors classified as girls at birth that is available to minors classified as boys at birth and vice versa. For example, the government writes, “a teenager whose sex assigned at birth is male can be prescribed testosterone to conform to a male gender identity, but a teenager assigned female at birth cannot.“ The U.S. government cites the Tennessee law as evidence of the legislature’s intent: “SB1 bluntly declares that it draws those sex-based lines to “encourag[e] minors to appreciate their sex” assigned at birth.” Because the classification is based on sex, the law needs to be reviewed with heightened scrutiny and the U.S. government claims that the law does not pass this standard: “Tennessee has made no attempt to tailor the law to the State’s asserted health concerns.”
Tennessee contends that the ban does not constitute a sex-based classification: “SB1 includes no sex classification. It draws a line between minors seeking drugs for gender transition and minors seeking drugs for other medical purposes. And boys and girls fall on both sides of that line.” Tennessee draws an analogy to reproductive rights cases that distinguish pregnancy and abortion from a sex classification, including Geduldig v. Aiello (in which the Supreme Court found pregnancy is not a sex-based classification), Bray v. Alexandria Women’s Health Clinic (in which the Supreme Court found that anti-abortion protesters were not in violation of the Equal Protection Clause because animus was to abortion, not women), and Dobbs v. Jackson Women’s Health Organization (in which the court wrote that state regulation of abortion is not a sex-based classification, despite equal protection claims not being before the court). Leaning on these cases, the state argues the law regulates medical care and is not sex discrimination, and therefore is not in violation of the 14th Amendment equal protection clause.
What is at stake with a Supreme Court decision?
The Court’s ruling in this case will impact laws restricting gender affirming care across the country and any future legal challenge to bans, at least on Equal Protection Grounds. Allowing the ban to stand would effectively leave the current patchwork of access to gender affirming care for minors, with different states permitting different levels of access to care. The 26 states with bans currently in place would likely keep them and others may follow suit. Under this scenario, where a young person lives will continue to dictate the access they have to gender affirming care and the number of those with limited access could increase. If the Court rules this way, plaintiffs in other cases may continue to pursue legal challenges to the bans based on other grounds, such as the 14th Amendment Due Process clause.
If the Court rules that the Tennessee ban is unconstitutional, similar bans in other states would also be unconstitutional and minors would gain greater protections in accessing gender affirming care nationwide.
The court could also conceivably rule that the Tennessee law does classify minors based on sex and remand the case back to the district court for further review.
The Court’s decision is expected in June 2025.
What might the impact of the incoming Trump Administration be?
The Supreme Court is hearing the case challenging the Tennessee ban at a time when state and federal actions around gender affirming care have become increasingly politicized. The court took the case at the request of the Biden administration. However, just over a month after hearing the case, President-elect Trump will take office and the Trump-Vance team has made clear that it will seek to limit access to gender affirming care through multiple mechanisms.
If the Court rules the Tennessee law is constitutional, it may be harder to challenge any new federal restrictions the Trump administration imposes. Indeed, even if the Court rules the Tennessee law is unconstitutional because it is sex discrimination, the Trump administration may still put forward other restrictions to care, such as in Medicaid and Medicare, contending these are not addressed by the Tennessee case.