Recent Trends in Mental Health and Substance Use Concerns Among Adolescents
In light of growing mental health concerns among adolescents in the United States, a National State of Emergency in Child and Adolescent Mental Health was issued in 2021, followed by advisories from the U.S. Surgeon General in 2021 and 2023. This comes at a time when many adolescents have reported adverse experiences, youth drug overdose deaths have spiked, and gun violence has increased. In 2021, 42% of adolescents reported feelings of sadness and hopelessness – which can be indicative of depressive disorder – up from 28% in 2011. Further, a recent KFF poll found that 55% of the public see youth mental health issues as a crisis in the U.S.; and that many children and teenagers are not able to get the mental health services they need.
Data on youth mental health is limited and when it is available, parents or guardians often complete survey questionnaires on behalf of youth in their household. However, the recently released Teen National Health Interview Survey (NHIS-Teen) surveyed adolescents (ages 12-17) directly, which allows for a more direct representation of adolescent mental health. This brief uses the NHIS-Teen data – which was collected for an 18 month period from 2021 to 2022 – to provide an up-to-date analysis of adolescent mental health, utilization of mental health care, and unmet needs and how they vary across demographics, including sex and sexual identity.1 Other survey data collected directly from adolescent populations, including the Youth Risk Behavior Surveillance System (YRBSS) and the National Survey on Drug Use and Health (NSDUH), are included to supplement and provide more context.
Key takeaways include:
- In 2021 and 2022, 21% of adolescents reported experiencing symptoms of anxiety in the past two weeks and 17% reported experiencing symptoms of depression. Female and LGBT+ adolescents were more likely than their counterparts to report experiencing anxiety or depression.
- Deaths due to drug overdose among adolescents more than doubled from 2018 (253 deaths) to 2022 (723 deaths). The largest increases in these deaths were among Hispanic and Black adolescents.
- Suicides are the second leading cause of death among adolescents. These deaths peaked in 2018 but have declined in recent years. In 2022, suicide death rates were highest among American Indian and Alaska Native adolescents (22.2 per 100,000) followed by White adolescents (7.2 per 100,000). Adolescent males had higher rates of suicide compared to their female peers (8.1 vs. 3.8 per 100,000) in 2022; however, thoughts of suicide and suicide attempts were higher (and increased faster) for females.
- In 2021 and 2022, 20% of adolescents reported receiving mental health therapy and 14% reported taking prescription medication. In general, LGBT+ and female adolescents were more likely to report receiving treatment than their counterparts.
- Many adolescents reported adverse experiences, including bullying (34%), emotional abuse by a parent (17%), and neighborhood violence (15%) in 2021 and 2022. Ninety-two percent of adolescents reported extended use of screens, which can also negatively impact mental health and well-being.
What share of adolescents experience poor mental health and how does that vary?
Approximately one in five adolescents reported experiencing symptoms of anxiety or depression (Figure 1). In 2021 and 2022, 21% of adolescents reported experiencing symptoms of anxiety in the past two weeks and 17% reported experiencing symptoms of depression. Anxiety and depression can co-occur with other mental health disorders and are associated with suicide and substance use. Additionally, these conditions can impact school attendance and performance among youth.
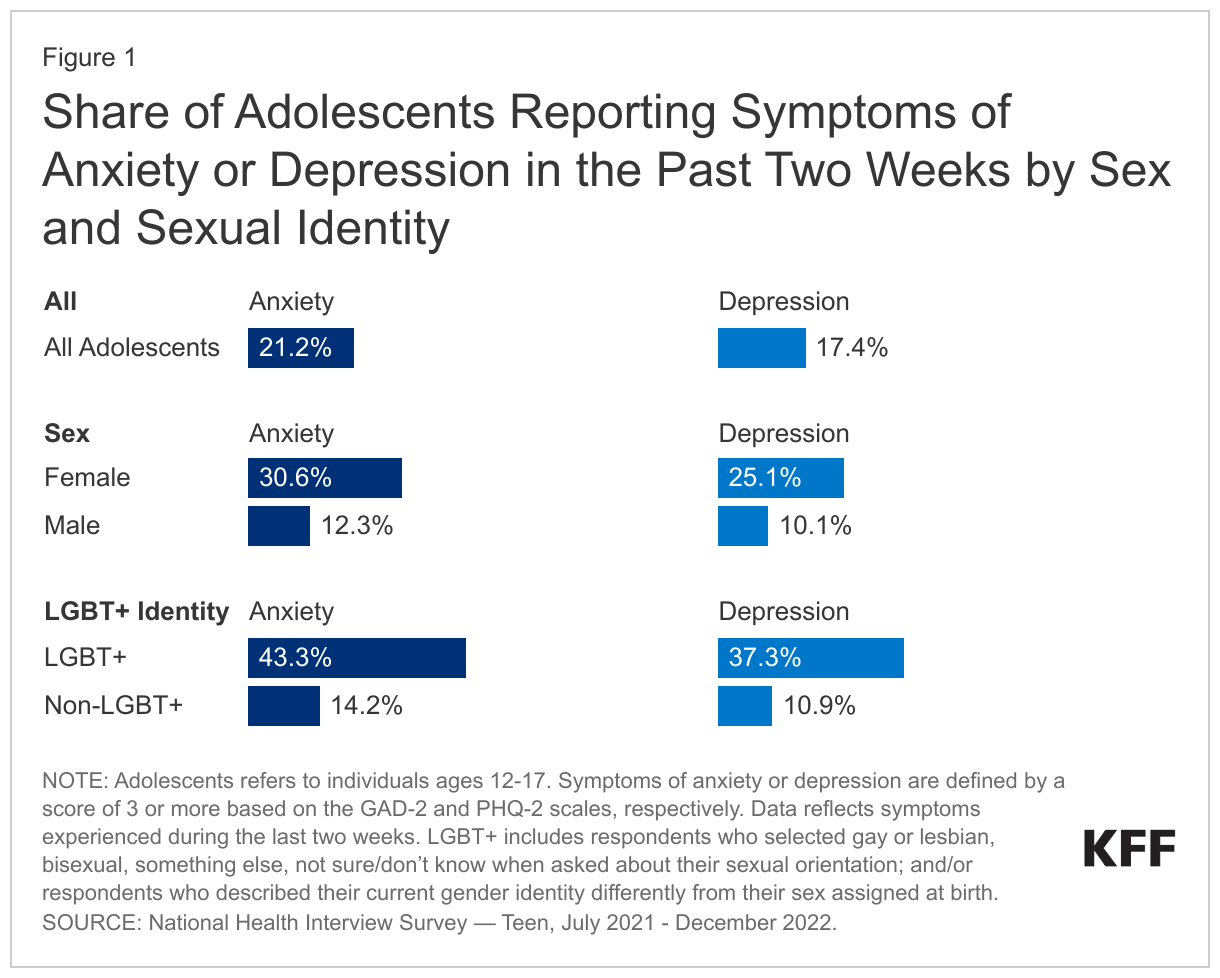
Female adolescents were more likely than their male peers to report anxiety (31% vs. 12%) and depression (25% vs. 10%) in 2021 and 2022 (Figure 1). These differences among adolescents by sex are consistent with other historical survey data on experiences of poor mental health. In recent years, other indicators of poor mental health, including self-harm and eating disorders, which commonly co-occur with anxiety, have increased, particularly among adolescent females. Analyses of emergency department visits, hospital admissions, and privately-insured youth found that, compared to prior to the pandemic, the presentation of eating disorders increased sharply for adolescent females. Historically, eating disorders affect females more than males. Eating disorders can be very harmful for physical health and even result in death.
In 2021 and 2022, LGBT+ adolescents were more likely than their non-LGBT+ peers to report anxiety (43% vs. 14%) and depression (37% vs. 11%) (Figure 1). Prior survey data has found similar differences in experiences of poor mental health between LGBT+ and non-LGBT+ adolescents.
While data on racial and ethnic groups from NHIS-Teen is not included in this analysis, data from NSDUH and YRBSS shows little variation in mental health conditions among adolescents by racial and ethnic groups. For example, in 2022, 20% of adolescents experienced a major depressive episode in the past year, with no significant differences across racial and ethnic groups. The 2021 YRBSS survey found that the share of Hispanic high school students that reported persistent feelings of sadness and hopelessness (46%) – which can be indicative of depressive disorder – was slightly higher than the share reported by their White (41%), Black (39%), and Asian peers (35%). However, mental health conditions among adolescents of color may be underreported as a result of underdiagnosis, gaps in culturally sensitive mental health care, structural barriers, and stigma associated with accessing care. Note that the NHIS-Teen survey data does not disaggregate data on non-Hispanic adolescents by racial groups and, therefore, was not included in this analysis.
How have substance use and related deaths among adolescents changed in recent years?
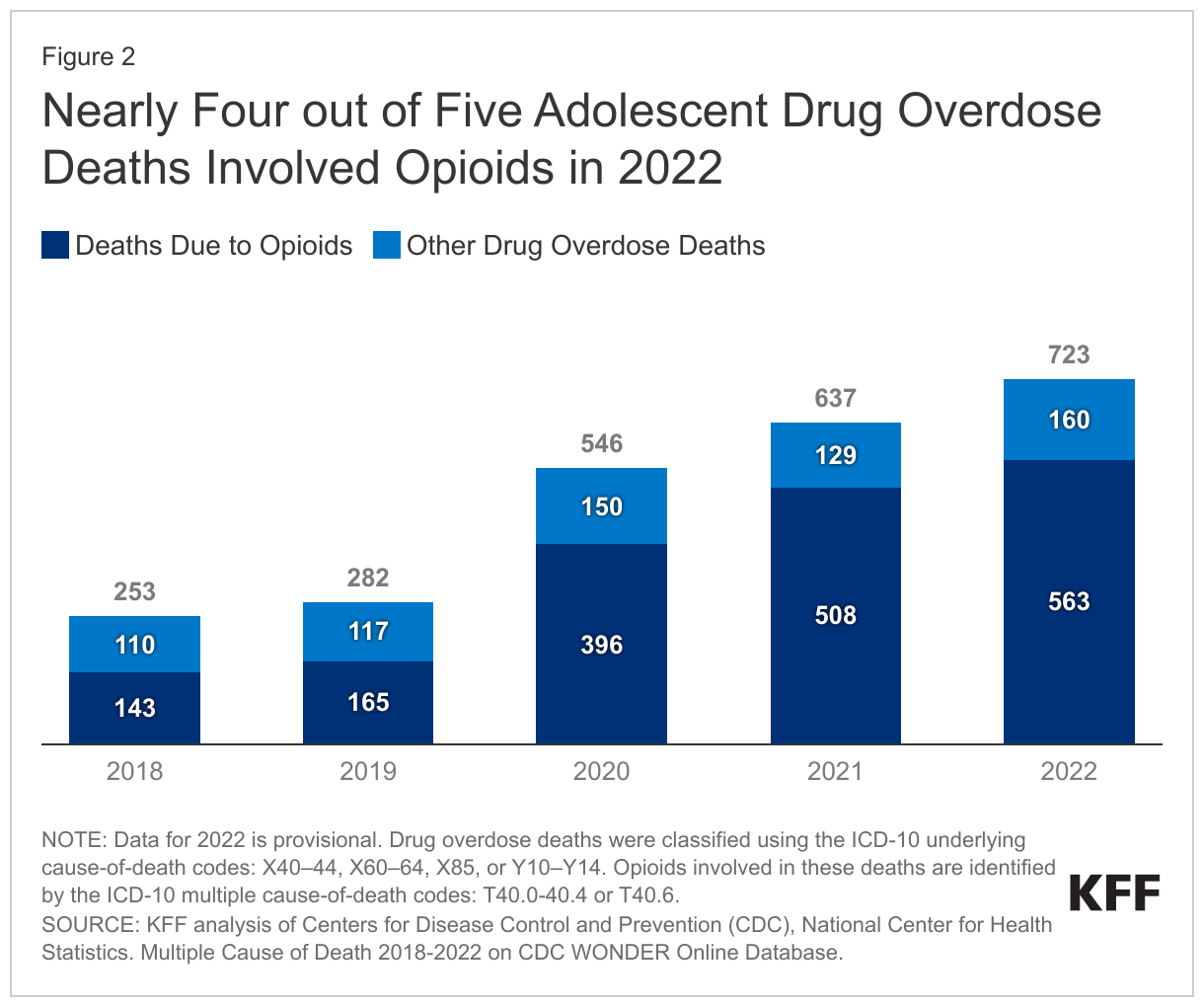
Deaths due to drug overdose among adolescents more than doubled since the onset of the COVID-19 pandemic, largely driven by the synthetic opioid, fentanyl. After remaining stable for several years, KFF analysis of CDC WONDER data found that drug overdose deaths among adolescents increased from 253 deaths in 2018 to 723 deaths in 2022 (Figure 2). During the same period, the share of these overdose deaths involving opioids increased from 57% to 78%.
Although White adolescents continue to account for the largest share of adolescent drug overdose deaths, Black and Hispanic adolescents have experienced the fastest increase in these deaths in recent years. In 2022, White adolescents accounted for 49% of total adolescent drug overdose deaths, down from 63% in 2018.2 This decrease reflects the rapid increase in drug overdose deaths among adolescents of color since the onset of the pandemic. By 2022, the drug overdose death rate of both Hispanic and Black adolescents (3.3 and 2.8 per 100,000) surpassed the overdose death rate of White adolescents (2.7 per 100,000) (Figure 3). Further, these drug overdose death rates increased more than fourfold among Hispanic and Black adolescents compared to prior to the pandemic.
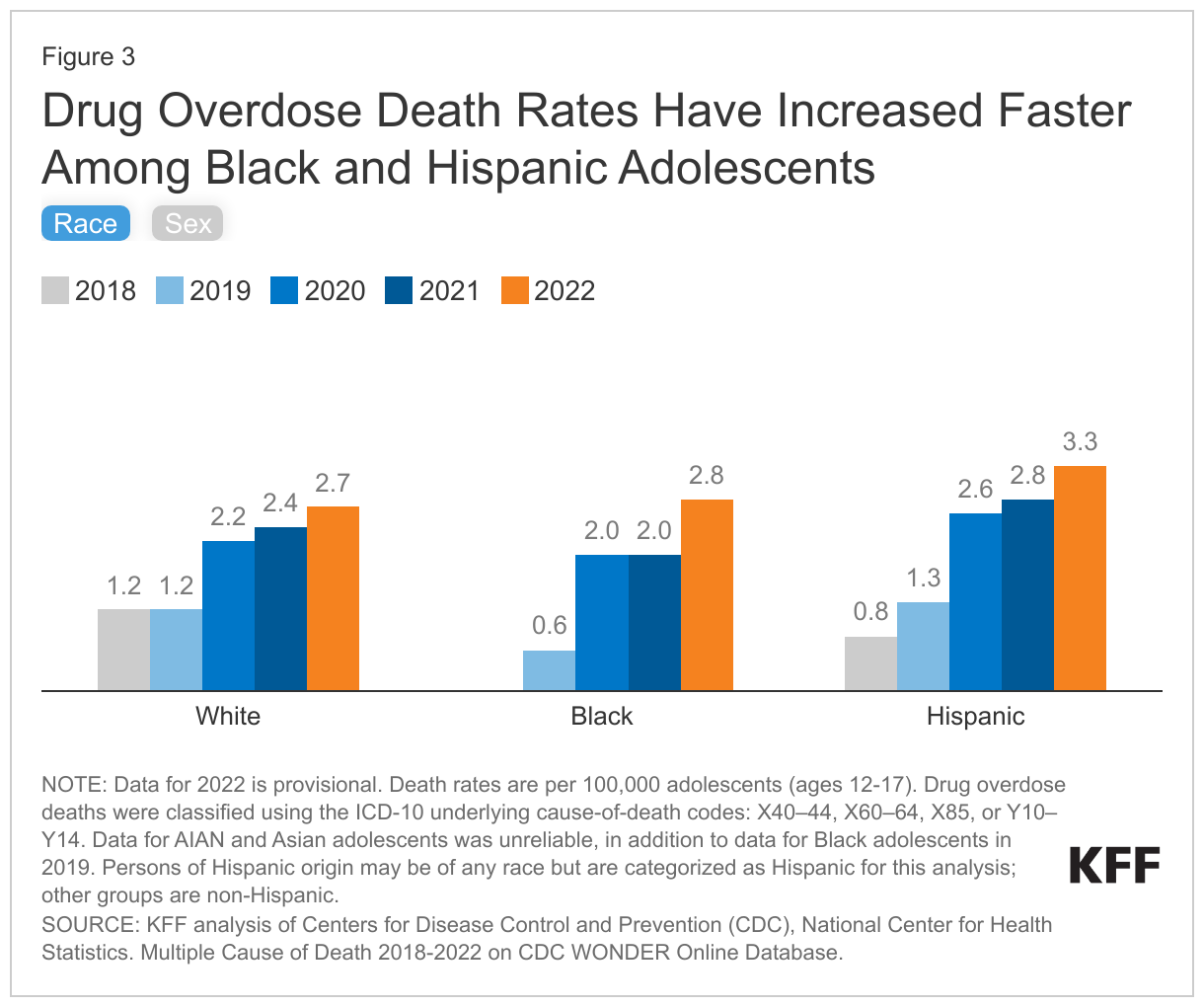
Since the COVID-19 pandemic began, drug overdose deaths increased for both adolescent males and females, with an initial spike among males. From 2018 to 2022, the drug overdose death rate more than doubled among adolescent males (from 1.1 to 3.0 per 100,000) and females (from 1.0 to 2.5 per 100,000) (Figure 3).
Although drug overdose deaths among adolescents have increased, their use of some substances has declined over time. YRBSS data from 2011 to 2021 shows declines in adolescent use of several substances, including current alcohol use (from 39% to 23%), current marijuana use (from 23% to 16%), and ever used illicit drugs (from 19% to 13%). However, findings on whether substance use has increased among adolescents during the pandemic are mixed. Some research has shown that substance use decreased in 2021 among adolescents and then largely held steady in 2022. Other research found that among high school students who used substances prior to the pandemic, nearly one in three reported increases in substance use in 2021. Early initiation of substance use is associated with increased risk of addiction later in life.
Mental health and substance use issues can often co-occur among adolescents. Data from NSDUH found that adolescents experiencing a past year major depressive episode in 2022 were more likely than peers to have used illicit drugs (26% vs 12%) and marijuana (22% vs 9%) in the past year, misused opioids (3% vs 1%) in the past year, and engaged in binge drinking (6% vs 3%) in the past month. In total, 4% of adolescents reported both a past year major depressive episode and substance use disorder in 2022. A recent analysis found that 41% of youth ages 10-19 that died from a drug overdose between 2019 and 2021 had a documented mental health condition.
How have suicide and self-harm among adolescents changed in recent years?
In the past decade, CDC data show that adolescent deaths due to suicide increased and peaked in 2018 (1,750 deaths) before slowing and declining by 2022 (1,540 deaths). Suicide remains the second leading cause of death among adolescents.3 However, from 2021 to 2022, the adolescent suicide death rate decreased by 8% (from 6.5 to 6.0 per 100,000) while the total population suicide death rate slightly increased. It is possible that some suicides are misclassified as drug overdose deaths since it can be difficult to determine whether drug overdoses are intentional. Forty-four percent of adolescent suicides were by firearm in 2022, compared to 40% in 2012.4
The rate of suicide deaths is increasing faster among adolescents of color compared to their White peers. Suicide death rates remain highest among American Indian and Alaska Native (AIAN) adolescents; in 2022, the death rate for AIAN youth was three times higher than White youth (22.2 vs. 7.2 per 100,000, respectively; Figure 4). Although their suicide death rates were lower than White adolescents, Black, Asian, and Hispanic adolescents experienced larger increases in these death rates from 2012 to 2022 (129%, 48%, 30%, respectively; Figure 4) compared to their White peers (26%). Further, in 2021, Black high school students were more likely to report attempting suicide than their Asian, Hispanic, and White peers.
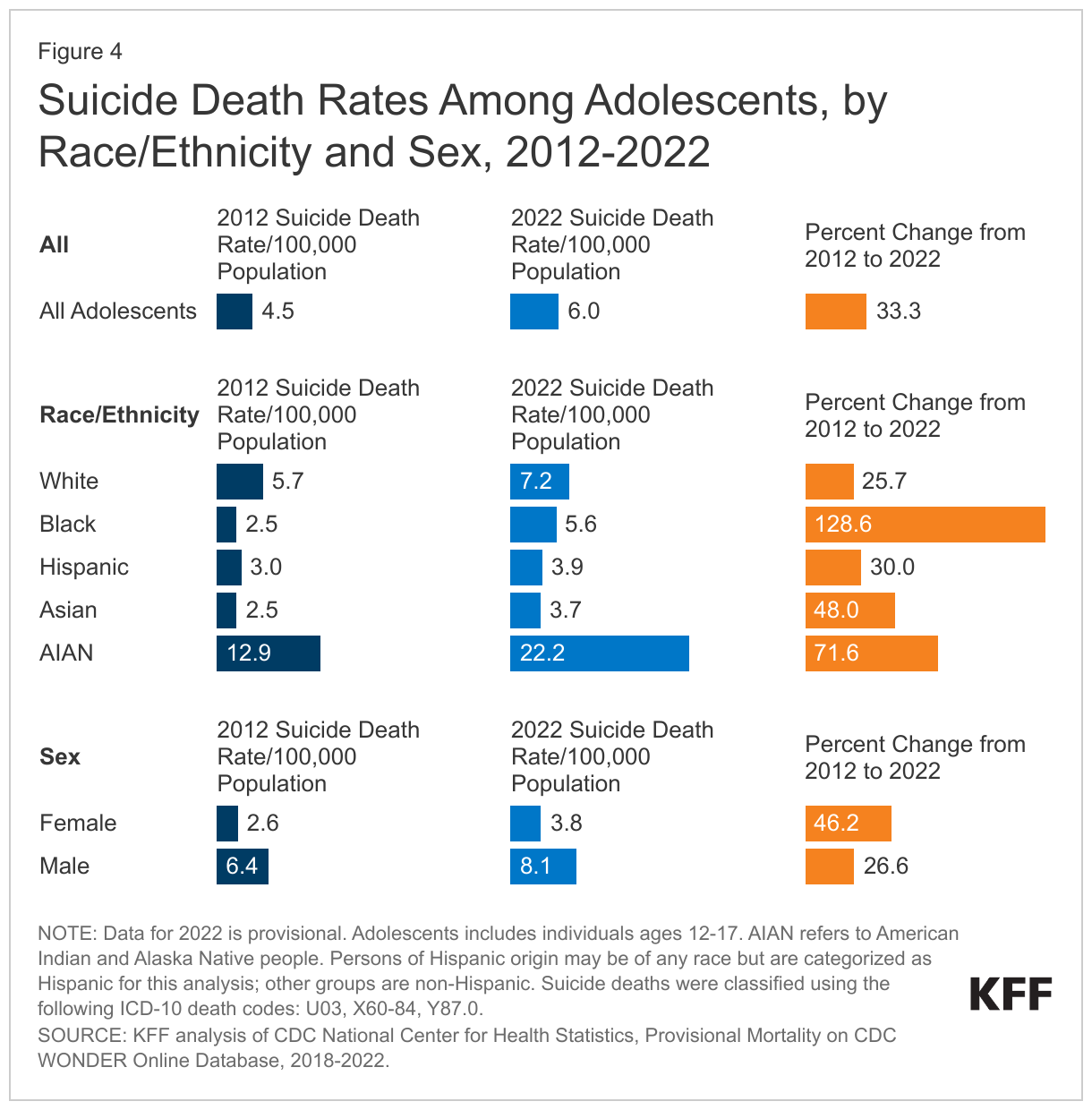
Among adolescents, male suicide rates are more than double the rates among females. Although the suicide death rate among adolescent females has increased faster than their male counterparts over the past decade, the adolescent female suicide death rate remains significantly lower than the death rate of their male peers (3.8 vs. 8.1 per 100,000 in 2022) (Figure 4). However, the share of adolescent females reporting serious thoughts of suicide remains higher and has increased faster over time (from 19% in 2011 to 30% in 2021) compared to adolescent males (from 13% in 2011 to 14% in 2021). Similar trends were seen in suicide attempts: from 10% in 2011 to 13% in 2021 among adolescent females, and from 6% to 7% over the same period for adolescent males. Additionally, as the pandemic progressed, emergency department visits for suicide attempts increased among adolescents, primarily driven by females.
LGBQ+ adolescents are more likely to experience suicidal thoughts compared to their heterosexual peers. Data from YRBSS found that in 2021, higher shares of LGBQ+ adolescents reported serious thoughts of suicide (45% vs. 15%) and suicide attempts (22% vs. 6%) compared to heterosexual adolescents.5 Data on suicide deaths by LGBQ+ identity were not available.
What share of adolescents report receiving mental health treatment in the past year and how does that vary?
Access to and sources of mental health services
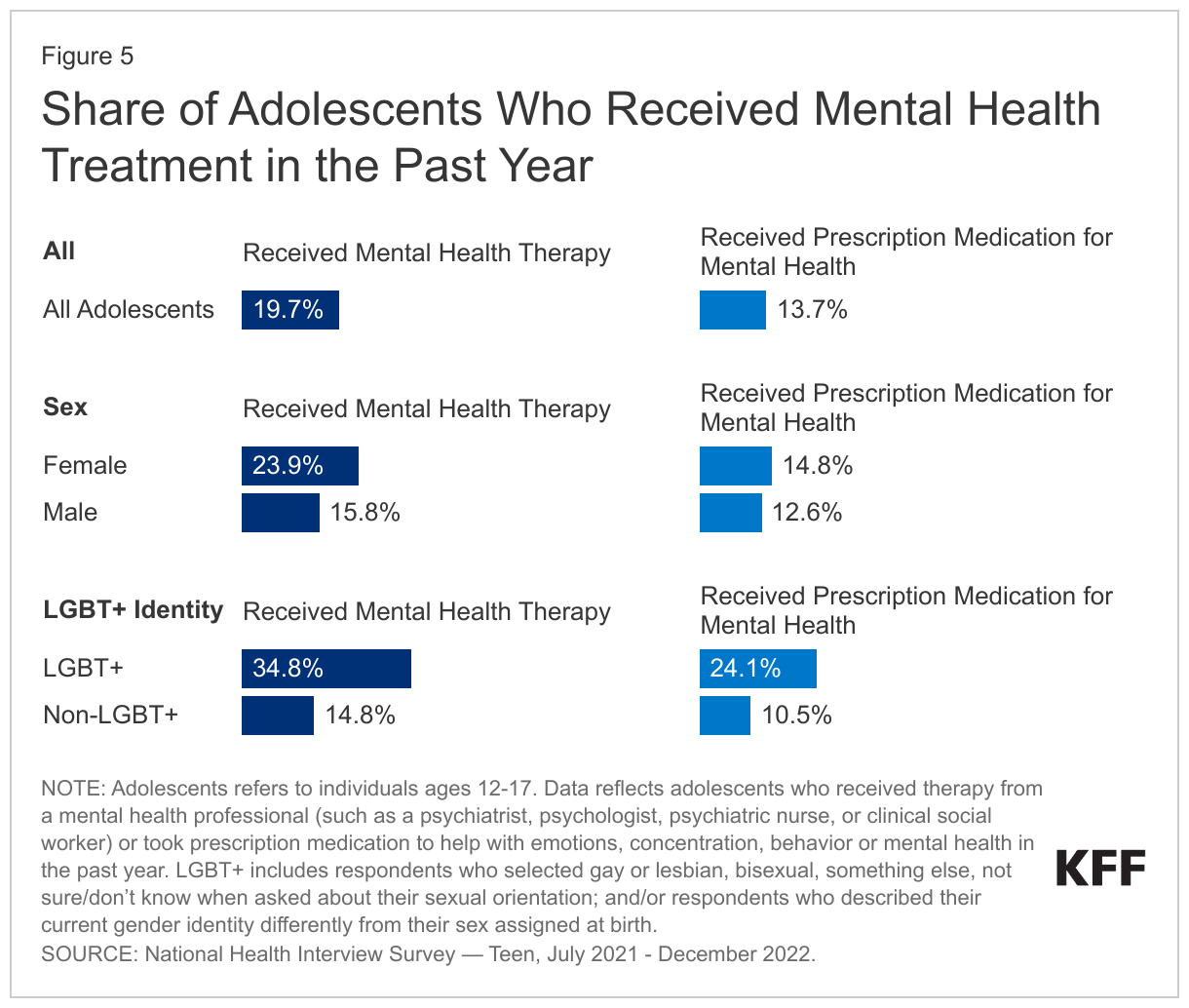
Among all adolescents, 20% reported receiving mental health therapy or counseling and 14% reported taking prescription medication for mental health in the past year (Figure 5). LGBT+ adolescents were more likely to report receiving mental health therapy or counseling (35%) and prescription medication (24%) for mental health in the past year than their counterparts (15% and 11%, respectively). Higher shares of female adolescents reported receiving mental health therapy or counseling compared to their male peers (24% vs. 16%).
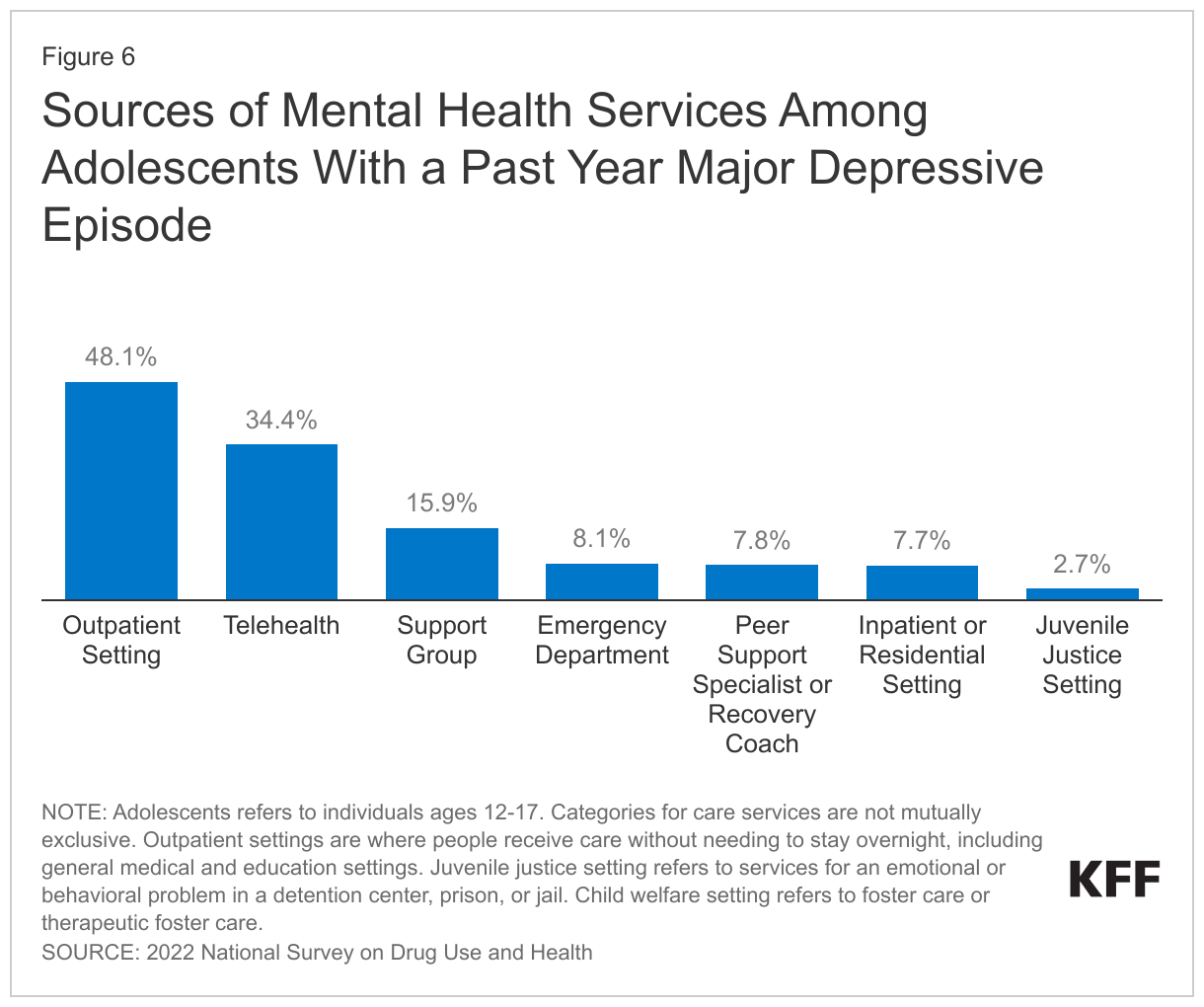
Among adolescents with a past year major depressive episode, mental health services were most often accessed through outpatient care and telehealth. Data from NSDUH found that in 2022, 19.5% of adolescents (or 4.8 million) had a past year major depressive episode. Major depressive episode refers to a period of at least two weeks when an individual experienced a depressed mood or loss of interest or pleasure in daily activities and had a majority of specified depression symptoms. Among these adolescents with a past year major depressive episode, 48% received mental health services in an outpatient setting, which includes general medical and education settings (Figure 6). Thirty-four percent of adolescents with a past year major depressive episode received mental health care via telehealth (care received via phone or video from a therapist or other health care professional) in 2022. Additionally, 8% of adolescents with a past year major depressive episode accessed mental health care at emergency departments. There has been an uptick in mental health-related emergency visits in recent years; however, emergency departments may have limited capacity to address psychiatric illnesses.
Unmet need for mental health services
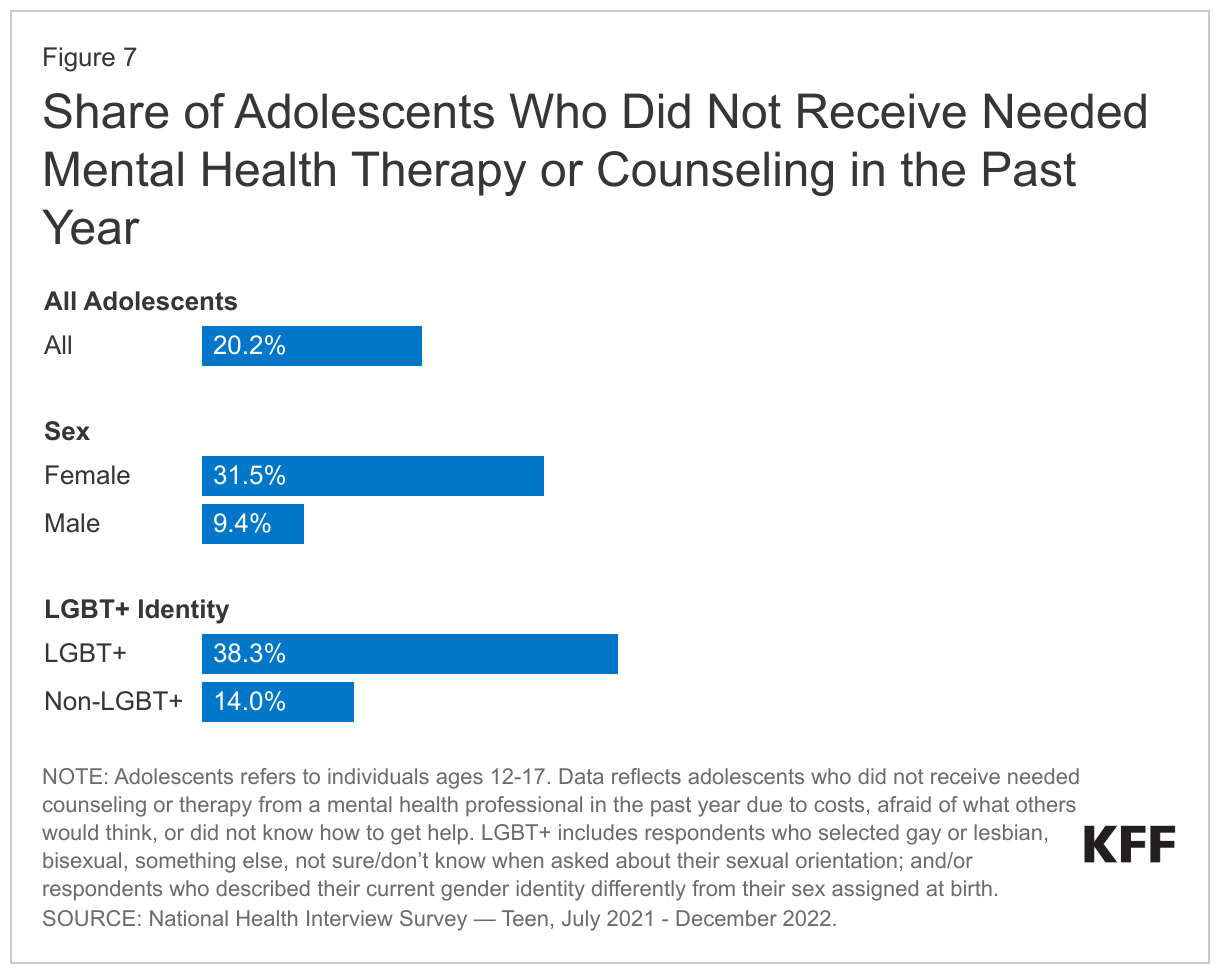
Although some adolescents received mental health care, 20% reported not receiving the mental health therapy they needed because of cost, fear of what others would think, and/or they did not know how to get help (Figure 7). This lack of needed therapy or counseling was more pronounced among female (32%) and LGBT+ adolescents (38%). While data on racial and ethnic groups from NHIS-Teen is not included in this analysis, other KFF analyses have found that receipt of mental health treatment is generally lower among people of color compared to their White peers.
Other factors that may contribute to limited mental health care access among adolescents include insurance barriers, a lack of providers, and the absence of culturally competent care. Additionally, in light of the COVID-19 pandemic, access and utilization of mental health care may have worsened. Among Medicaid and CHIP beneficiaries, utilization of mental health services declined by 25% for beneficiaries 18 and younger from March 2020 to July 2022 compared to prior to the pandemic; and utilization of substance use disorder services declined by 31% for beneficiaries ages 15-18 during the same period. Nearly two out of five children under the age of 18 in the U.S. are Medicaid or CHIP beneficiaries.
Although adolescent drug overdose deaths have increased, access to buprenorphine and residential addiction treatment facilities is limited. The dispensing of buprenorphine, a medication approved to treat opioid use disorder, is low among adolescents. Additionally, many residential addiction treatment facilities do not have availability for adolescents and are costly. These facilities often do not provide buprenorphine to adolescents with opioid use disorder.
If untreated, mental health conditions can persist into adulthood and limit quality of life. In 2021 and 2022, just over half of teens (55%) reported discussing their mental or emotional health with their health care provider in the past year; and only 20% reported discussing transitions in their health care services that will go into effect when they turn 18.
What experiences among adolescents may negatively impact their mental health and well-being?
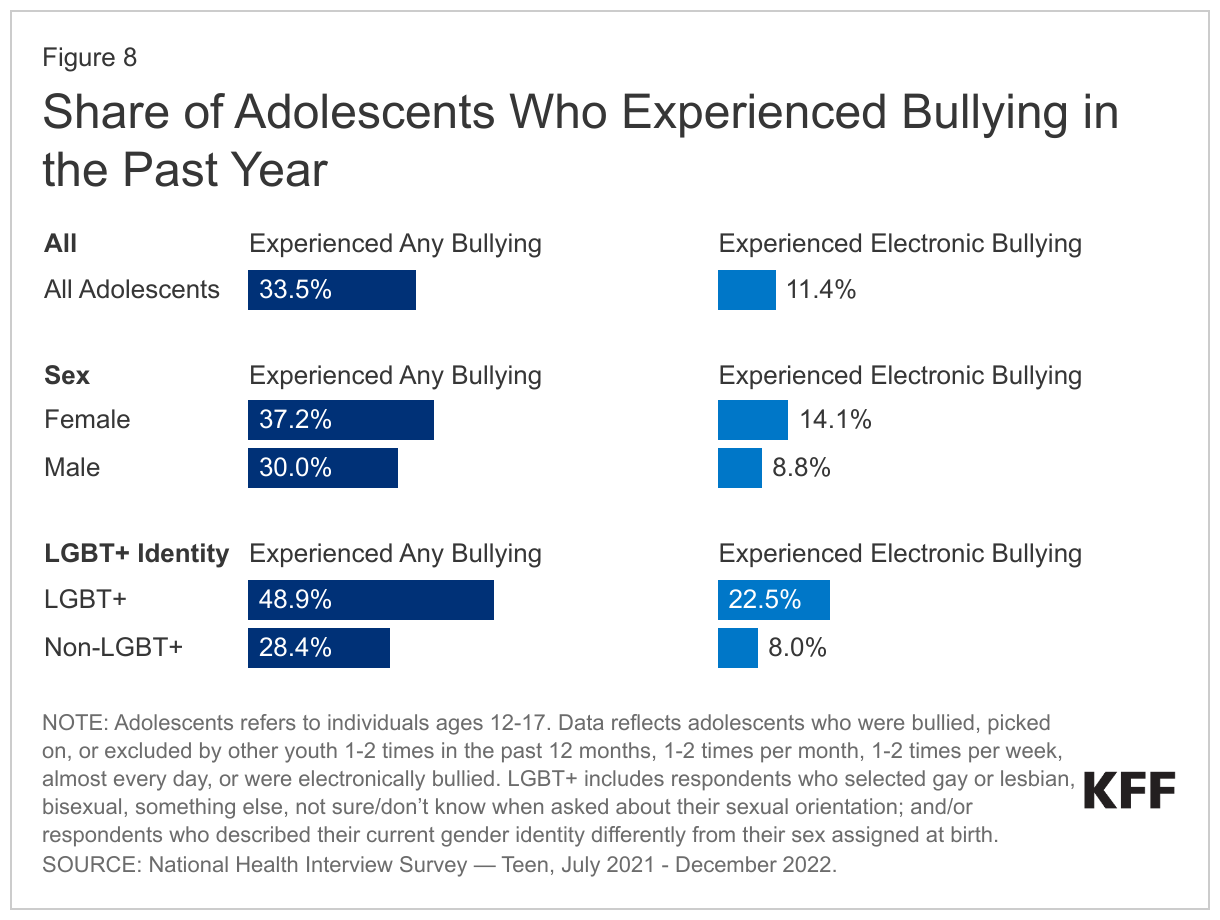
Many adolescents report negative experiences that can impact their mental health and well-being, including bullying (34%) and, specifically, electronic bullying (11%) (Figure 8). Higher shares of LGBT+ adolescents reported experiencing bullying (49%), and electronic bullying (23%), compared to their peers (28% and 8%, respectively). Bullying can increase the risk of mental health conditions, substance use, and self-harm. Electronic bullying may be associated with depression among youth and is more often experienced by female and sexual minority youth compared to their peers.
Adolescents are also spending more time on screens, including social media, which may lead to depression and poor well-being. Ninety-two percent of adolescents reported at least two hours of weekday screentime not associated with schoolwork. Emerging research has found that both smartphone use and social media use may be associated with poor well-being among youth, with a higher risk of depression for female adolescents. Social media use can also lead to difficulties with sleep and maintaining attention.
Many adolescents report adverse experiences which can lead to both mental and physical health concerns. In 2021 and 2022, 21% and 18% of adolescents reported living with a household member experiencing mental illness or substance use issues, respectively; 17% reported emotional abuse by a parent or adult in their household; 15% reported neighborhood violence; and 11% reported having a parent in jail or prison. Adverse childhood experiences are linked to mental illness, substance use, and chronic physical health problems in adolescence and can extend into adulthood. Social supports, including relationships with peers, can be a protective factor among adolescents in the face of adverse experiences. However, only 50% of adolescents reported having peer support “a lot of the time” in 2021 and 2022.
Gun violence continues to rise and may lead to negative mental health impacts among children and adolescents. An increasing number of children and adolescents have been exposed to gun violence in recent years. School shootings have increased and, beginning in 2020, firearms became the leading cause of death among children and teens ages 19 and below. Children and adolescents may experience negative mental health impacts, including symptoms of anxiety, in response to school shootings and gun-related injuries or deaths in their communities. Youth antidepressant use has also been shown to increase following exposures to fatal school shootings.
Looking Ahead
National efforts to address youth mental health concerns include recommendations for mental health screenings and strengthening social media safety protocols, and federal legislation to expand school-based mental health services. The U.S. Preventive Services Task Force put forth recommendations for youth anxiety and depression screenings and the U.S. Surgeon General also issued several advisories, including an advisory on youth mental health and social media that highlights potential solutions for strengthening social media safety protocols and encouraging digital and media literacy. Recently, the U.S. Senate Judiciary Subcommittee held a hearing on the impact of social media on youth mental health and well-being. In light of the increase in mental health-related pediatric ED visits, the American Academy of Pediatrics, the American College of Emergency Physicians and the Emergency Nurses Association released a statement including recommendations to improve care for mental health emergencies. Recent legislation allows for the expansion of school-based mental health care through a number of strategies, including growing the number of school-based mental health providers, leveraging Medicaid to further build out services, and providing trauma care to students.
At the state and local level, initiatives to improve access to youth mental health care include promoting school-based Medicaid behavioral health services and connecting youth to virtual care at no cost. State Medicaid programs have taken a variety of approaches to promote access to Medicaid behavioral health services provided in schools. These include working closely with local education agencies, taking advantage of the reversal of the free care policy, and increasing reimbursements for school-based providers. Local initiatives have also been proposed, including a partnership with New York City’s Department of Health and Mental Hygiene and the mental health app Talkspace to allow for teenagers to connect virtually with licensed therapists at no cost. However, the quality and clinical effectiveness of emerging mental health apps remains unclear. Looking ahead, data on adolescent populations will be pivotal in understanding how to further address and mitigate rising mental health and substance use concerns.
This work was supported in part by the Well Being Trust. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Endnotes
The NHIS-Teen data does not disaggregate data on non-Hispanic adolescents by racial groups and, therefore, was not included in this analysis.
Drug overdose death distributions by race and ethnicity do not include non-Hispanic individuals of more than one race. KFF analysis of CDC WONDER. Accessed at: https://wonder.cdc.gov/mcd-icd10-provisional.html
KFF analysis of Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS). Accessed at: https://webappa.cdc.gov/sasweb/ncipc/leadcause.html
KFF analysis of Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS). Accessed at: https://wisqars.cdc.gov/fatal-reports
The 2021 YRBSS did not include questions on gender identity.