Opioid Overdose Deaths: National Trends and Variation by Demographics and States
Since the opioid epidemic was declared a public health emergency in 2017, it has claimed more than half a million lives. While the epidemic was initially driven by prescription opioids and heroin, it has evolved in recent years, to be dominated by illicit synthetic fentanyl—a substance significantly more potent than morphine. By 2023, most counterfeit opioid pills contained a deadly dose. As of 2022, nearly 1 in 3 adults reported in a KFF survey that they or a family member have been addicted to opioids (29%).
Leading up to and during the pandemic, opioid overdose deaths increased sharply. Deaths began to fall in mid-2023 and have continued to decline, though they remain above pre-pandemic levels. While it is not possible to identify a single driver of the decline, multiple policy actions may have contributed. These policies included efforts to expand access to treatment and overdose-reversal drugs and public awareness efforts about counterfeit opioid pills. They also included supply-side actions aimed at improving fentanyl detection at the ports and borders and limiting the flow of precursor chemicals used to manufacture illicit fentanyl abroad. These efforts coincided with indicators of shifting fentanyl supply, including DEA testing that suggested lower fentanyl potency in counterfeit pills.
Despite progress, a range of more recent federal policy actions may affect future trends, including federal budget cuts, federal staffing reductions, and cuts to federal grants that support state and local programs; reduced Medicaid and Marketplace coverage; and a shift toward a more enforcement-focused approach, including the designation of illicit fentanyl as a “Weapon of Mass Destruction.” This analysis examines opioid overdose deaths over time – including 2024 (the latest finalized data available through CDC WONDER data) – and trends across demographic groups and states. Additional data can be found on KFF’s State Health Facts.
Key Takeaways:
Overall trends: Opioid overdose deaths fell sharply from 2023 to 2024 (79,358 to 54,045), driven largely by decreases in fentanyl-involved deaths. Even after these declines, deaths remained above 2019, the year before opioid deaths increased sharply during the pandemic.
Demographic variation: In 2024, opioid death rates were the highest among those aged 26-64, AIAN people, Black people, and males. All demographic groups saw declines in opioid death rates from 2023 to 2024. However, most groups still had higher rates in 2024 than in 2019.
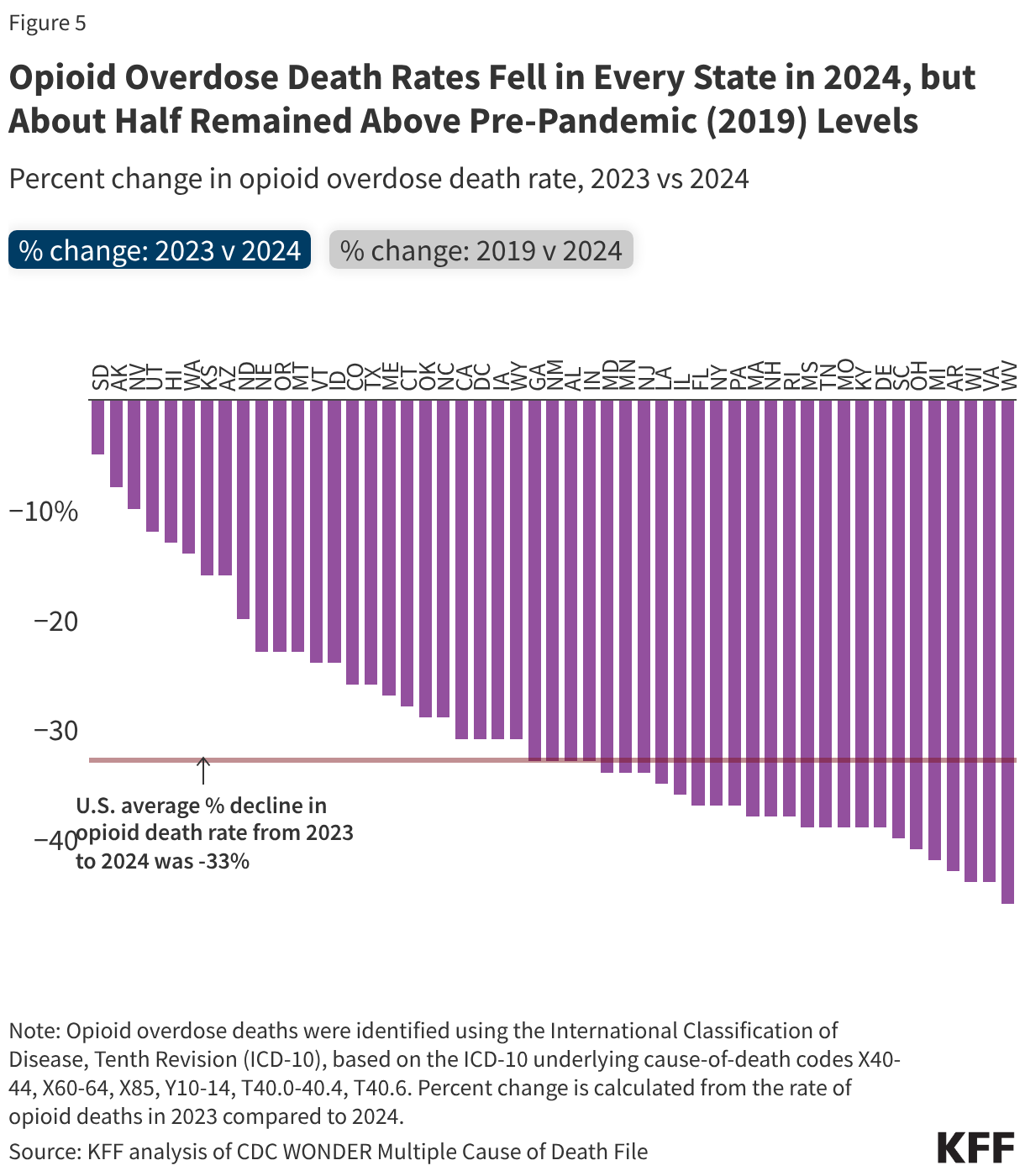
State variation: State rates in 2024 ranged from 3.3 per 100,000 in Nebraska to 38.6 per 100,000 in West Virginia. From 2023 to 2024, opioid death rates fell across all states, with the largest drops in Virginia (-44%), Wisconsin (-44%), and West Virginia (-46%). About half of states remained above 2019 levels, which may reflect differences in the timing of fentanyl’s spread and state policy.
What are the trends in opioid deaths?
Opioid overdose deaths fell sharply in 2024, nearing pre-pandemic levels but remaining above 2019 (Figure 1). Total drug overdose deaths dropped from 105,007 in 2023 to 79,384 in 2024 (-24%), while opioid deaths fell from 79,358 to 54,045. Provisional CDC data suggest opioid deaths have continued to decline through 2025. By 2024, opioid deaths were near but still above pre-pandemic (2019) levels, about 4,200 higher than in 2019, the year before the sharp pandemic-era rise in opioid deaths.
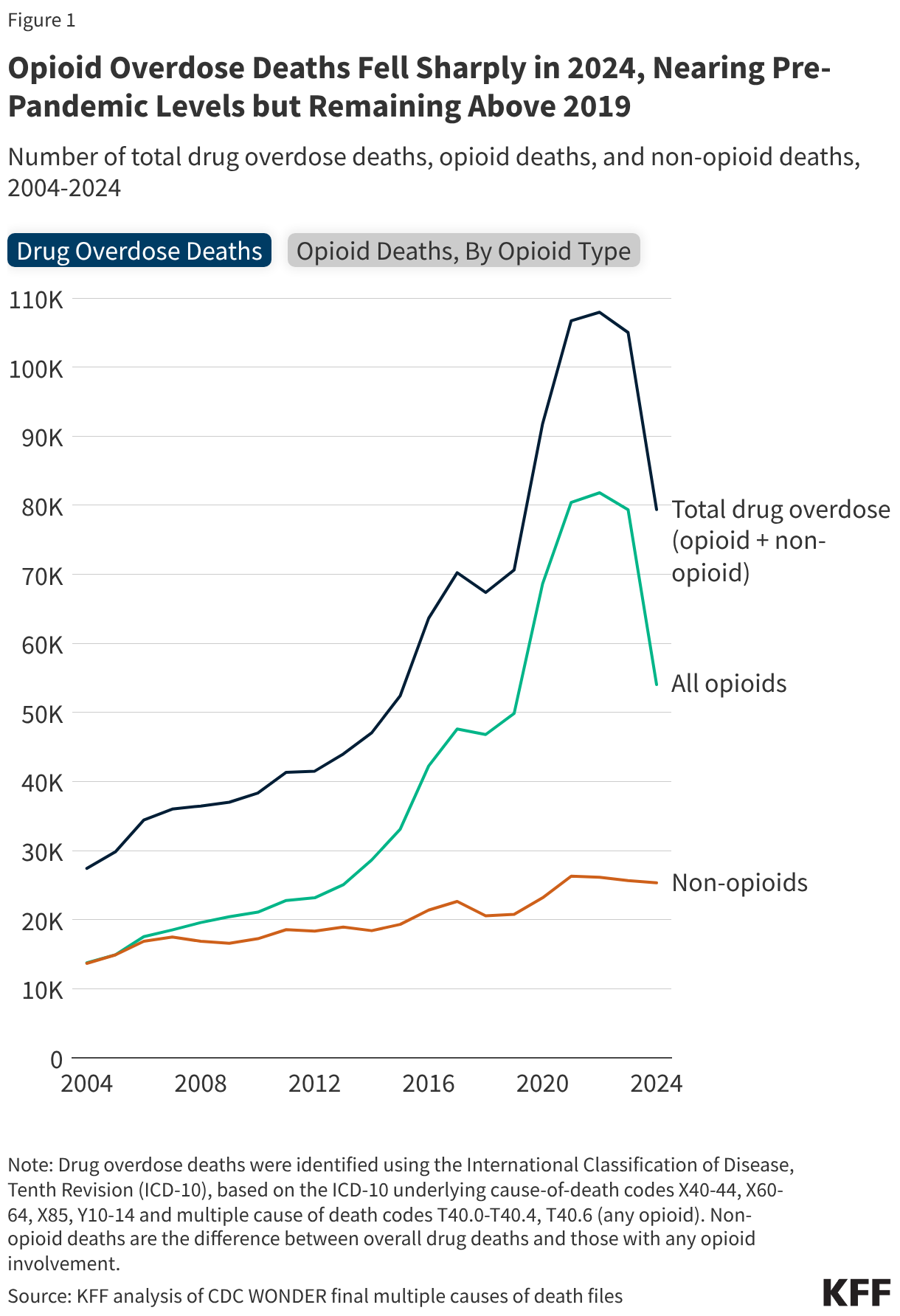
Fentanyl was involved in most opioid overdose deaths in 2024 (Figure 1). Declines in fentanyl-involved deaths drove the overall drop in opioid deaths. Deaths involving other opioids, including prescription opioids and heroin, also declined but to a lesser extent. Opioid overdose deaths include fatalities of unintentional, intentional (suicide or homicide), and unknown intent. Any drug overdose death involving opioids is counted as an opioid overdose death. Because more than one opioid can be involved in a single death, opioid subcategories do not sum to total opioid deaths.
How do opioid deaths vary across demographics?
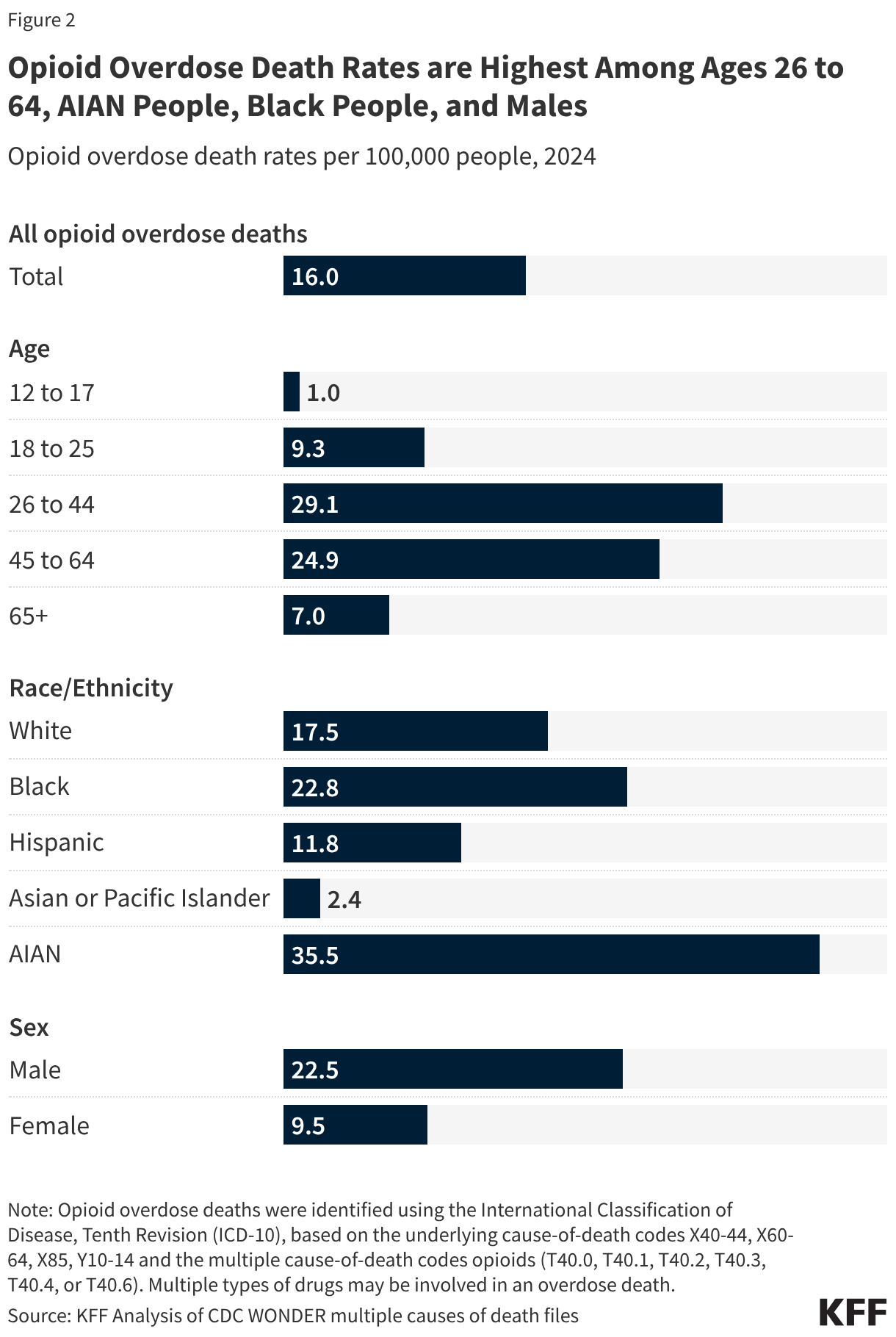
In 2024, opioid death rates were highest among adults ages 26 to 64, American Indian/Alaska Native (AIAN) people, Black people, and males (Figure 2). Rates were highest among adults ages 26 to 44 and 45 to 64 (29.1 and 24.9 per 100,000, respectively), well above other age groups. By race and ethnicity, AIAN people had the highest opioid death rate (35.5 per 100,000), and Black people had somewhat higher rates than White people (22.8 vs. 17.5 per 100,000), a reversal from earlier in the opioid epidemic when rates were higher among White people. Because White people make up a much larger share of the population, the number of deaths was highest among White people (33,105), followed by Black people (10,202) and AIAN people (845), even though rates were higher among Black and AIAN people. Opioid death rates among males were more than double those of females.
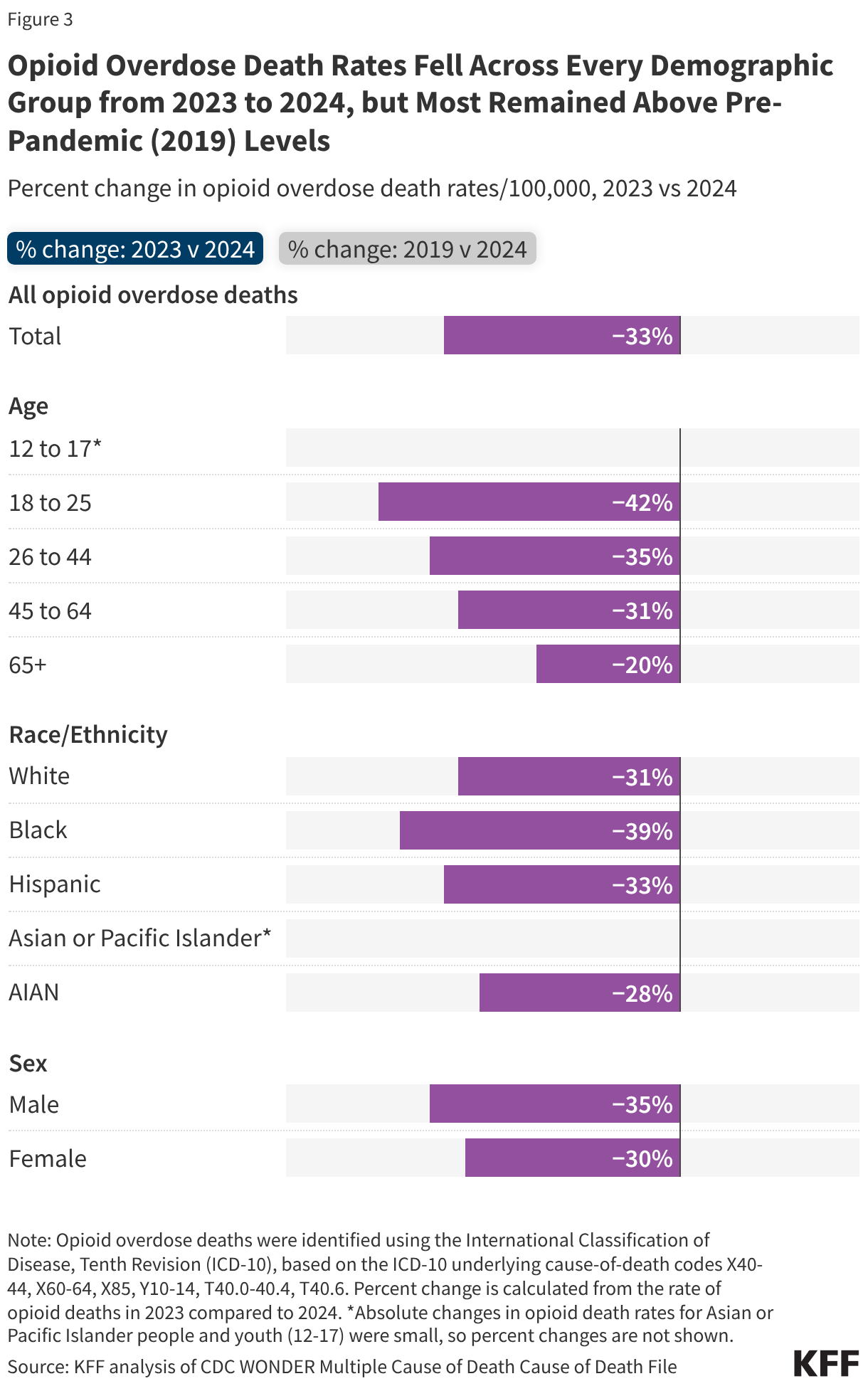
From 2023 to 2024, opioid overdose death rates declined across all demographic groups (Figure 3). Young adults (ages 18 to 25) saw the largest decline (-42%), while adults ages 65+, saw the smallest (-20%). Declines by race and ethnicity ranged from -28% among AIAN people to -39% among Black people, and rates fell for both males and females.
Most demographic groups continued to have higher opioid death rates in 2024 than in 2019 (Figure 3). Rates remained especially elevated among AIAN people (+101%) and adults ages 65+ (+63%). Slower declines among older adults may reflect that SUD can be harder to detect and treat and that few treatment programs are tailored to older adults. Two groups had lower rates in 2024 than in 2019: White people (-9%) and young adults ages 18-25 (-30%). Declines among White people relative to other race and ethnicity groups may partly reflect better access to opioid use disorder treatment.
How do opioid deaths vary across states?
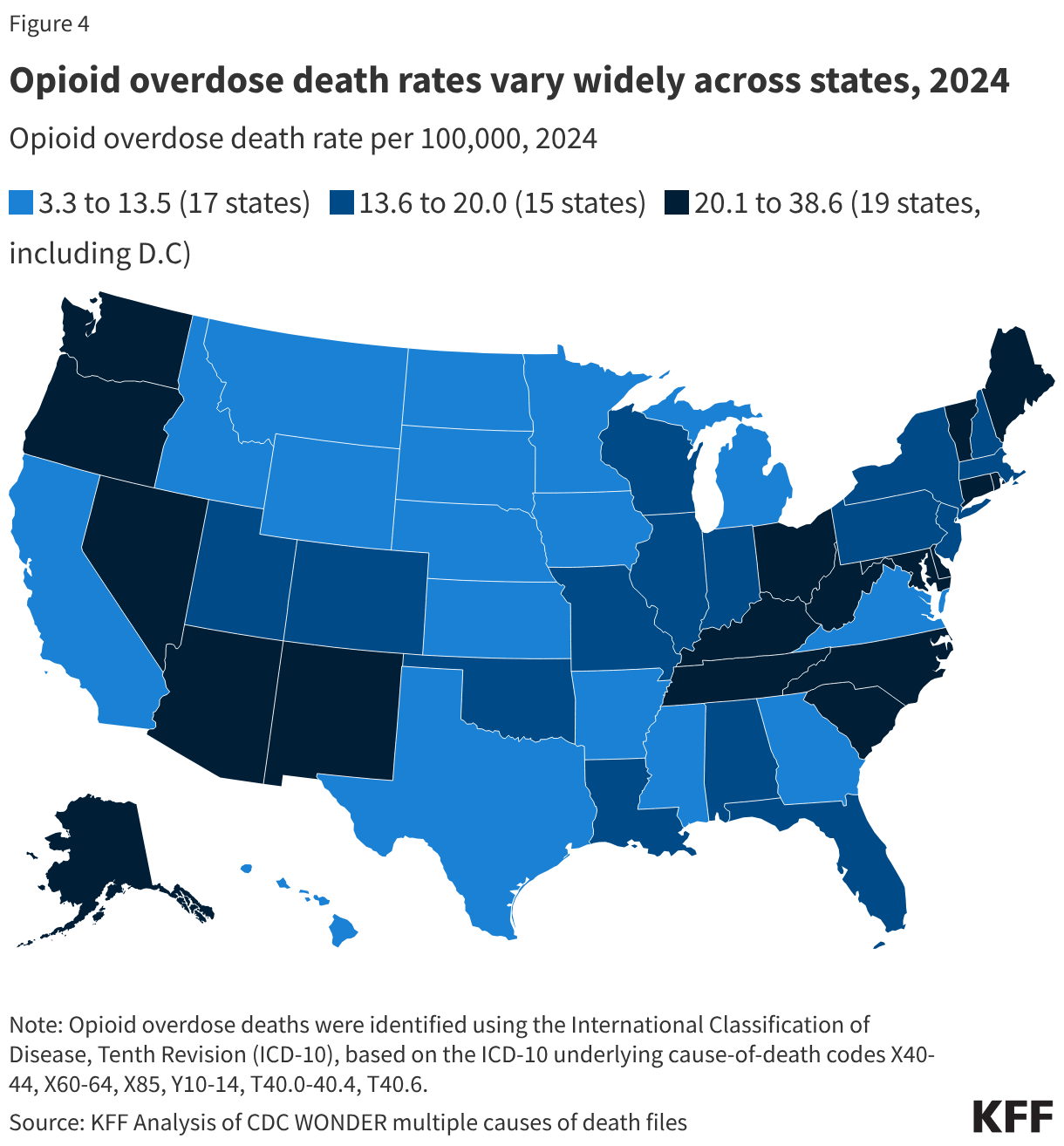
Opioid overdose death rates varied across states in 2024, ranging from 3.3 per 100,000 in Nebraska to 38.6 in West Virginia (Figure 4). Nebraska, South Dakota, and Iowa had the lowest opioid death rates, (3.3, 5.4, and 5.8 deaths per 100,000 people, respectively). Rates were the highest in the District of Columbia (34.1 per 100,000), Alaska (37.0), and West Virginia (38.6).
All states had declines in opioid overdose death rates from 2023 to 2024, but the size of the decline varied widely. Rates fell by 5% in South Dakota and 8% in Alaska, compared with larger drops of 44% in Wisconsin and Virginia and 46% in West Virginia (Figure 5). KFF State Health Facts provides opioid overdose rates by state for 1999-2024.
By 2024, about half of states continued to have opioid overdose rates above 2019 levels. Several states were close to pre-pandemic levels, including D.C. and Utah (+1%, +2%, respectively). Over one-third of states (39%) had rates that dipped below 2019 levels, with the largest declines in NJ (-42%), Ohio and Massachusetts (each -36%). Alaska and Oregon had the largest increases relative to 2019 (+239% and +226%) (Figure 5).
State differences in opioid-related policy and the timing of fentanyl spread may help explain variation in opioid overdose death trends. Differences in how states use state opioid response grants and settlement funds, and how states structure Medicaid coverage for substance use services, including whether they adopt federal opportunities to expand treatment access may affect outcomes. Fentanyl spread unevenly across states over time, generally moving from east to west. As a result, some states experienced earlier increases, often before the pandemic, while others saw their steepest growth later. These policy and timing differences can affect how states’ 2024 rates compare with 2019.