A Look at Substance Use and Mental Health Treatment Facilities Across the U.S.
Most Americans (90%) think we are in the midst of a mental health crisis, and trends in data support these opinions. Provisional data from 2022 indicate record numbers of suicides and drug overdose deaths—marking substantial growth in both over the past decade. Despite the escalation of mental health needs and the increasing and evolving opioid epidemic, accessing treatment continues to be difficult–as indicated by consumer surveys and national data. Factors like the decline in psychiatric beds, financing barriers, difficulty accessing outpatient treatment, and the growing workforce shortages have led to more reports of unmet needs and psychiatric boarding in emergency departments. This issue may be particularly acute among certain groups needing targeted care, such as youth and adolescents. Given that a growing number of youth and over one-third of US adults have mental health or substance use conditions (half of which are moderate or severe) there will likely continue to be discussions aimed at aligning treatment infrastructure, workforce, and financing to meet the outpatient and intensive needs of this population. Further, the effectiveness of the recently launched 988 hotline and crisis services may depend on the availability of a robust behavioral health infrastructure that allows crisis workers to link people into care, including outpatient care and more intensive services.
This brief uses 2022 data from the National Substance Use and Mental Health Services Survey (N-SUMHSS). The N-SUMHSS is an annual survey sent to all substance use and mental health treatment facilities to assess the supply and characteristics of these facilities at a national and state level. Key N-SUMHSS indicators are available at a national and state level on KFF State Health Facts (SHF).
Number of facilities and beds
Substance use and mental health treatment facilities vary in their settings and services. Some provide hospital inpatient care, involving overnight stays and medical monitoring, and others offer outpatient services where patients visit for treatment sessions but do not stay overnight. Facilities sometimes provide multiple types of care; for example, a residential facility might also offer outpatient care. Most facilities typically specialize in either mental health or substance use treatment, but about 15% specialize in both. Consumer difficulties in accessing care have been linked to a shortage or uneven distribution of facilities and beds, and although these facility shortages are acknowledged as contributing factors, there is no established consensus or best practices for estimating bed needs. In this report, and for KFF SHF indicators, substance use and mental health facilities are reported separately to give a detailed state-level look at treatment settings and characteristics. Types of care provided at facilities are typically grouped into the following categories:
- Outpatient care is usually less intensive treatment, typically consisting of sessions that last 3 hours or less and take place 1 or 2 days per week.
- Partial Hospitalization or Day Treatment is a form of outpatient treatment that is typically less intensive than residential care, but more intensive than outpatient. It typically occurs over 3 hours a day and more than 2 days a week and can sometimes be an alternative to inpatient or residential care services.
- Residential care is typically provided outside of hospitals and can involve longer overnight stays with supervised living and supportive services. Its intensity varies but it is considered a higher level of care than outpatient, typically reserved for those with more acute needs.
- Inpatient care involves overnight hospital stays with medical management or monitoring, typically for emergency situations or cases needing intensive medical supervision.
Overall, there are approximately 14,700 facilities providing substance use treatment services and about 9,500 facilities that offer mental health services. This data primarily reflects registered facilities and may not include smaller practices or solo practitioners that provide substance use or mental health treatment services. Additionally, the data might not include facilities that provide treatment in settings or physician practices not specifically registered as substance use or mental health treatment facilities. For instance, general practitioners prescribing antidepressants in primary care settings that are not dedicated to mental health or substance use treatment may not be reflected in this data.
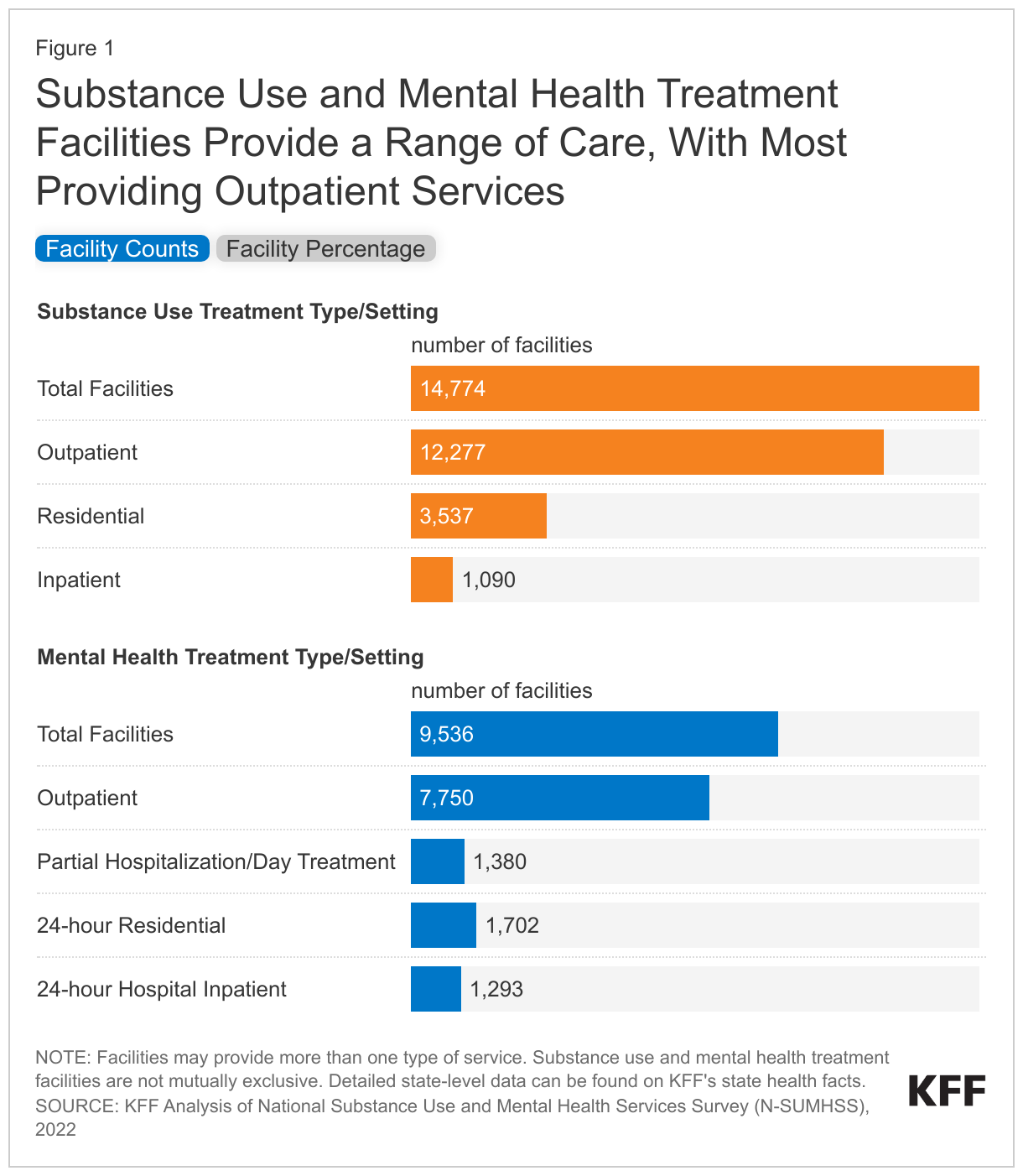
More than eight in ten substance use treatment facilities and mental health facilities provide outpatient services; smaller shares offer more intensive inpatient services. The American Academy of Addiction Medicine categorizes substance use treatment into levels of care, ranging from screening and less intensive outpatient services to the most intensive, medically managed inpatient services. Nationally, 83% of substance use treatment facilities offer outpatient care, 24% offer residential care, and 7% offer inpatient care. About 81% of mental health facilities offer outpatient services, which are less intense than higher levels of care—like 24-hour hospital inpatient or 24-hour residential services. The availability and type of treatment services vary by state. In some cases, states with a lower share of one type of intense treatment will be offset by a higher share of facilities offering a different type of higher intensity treatment.
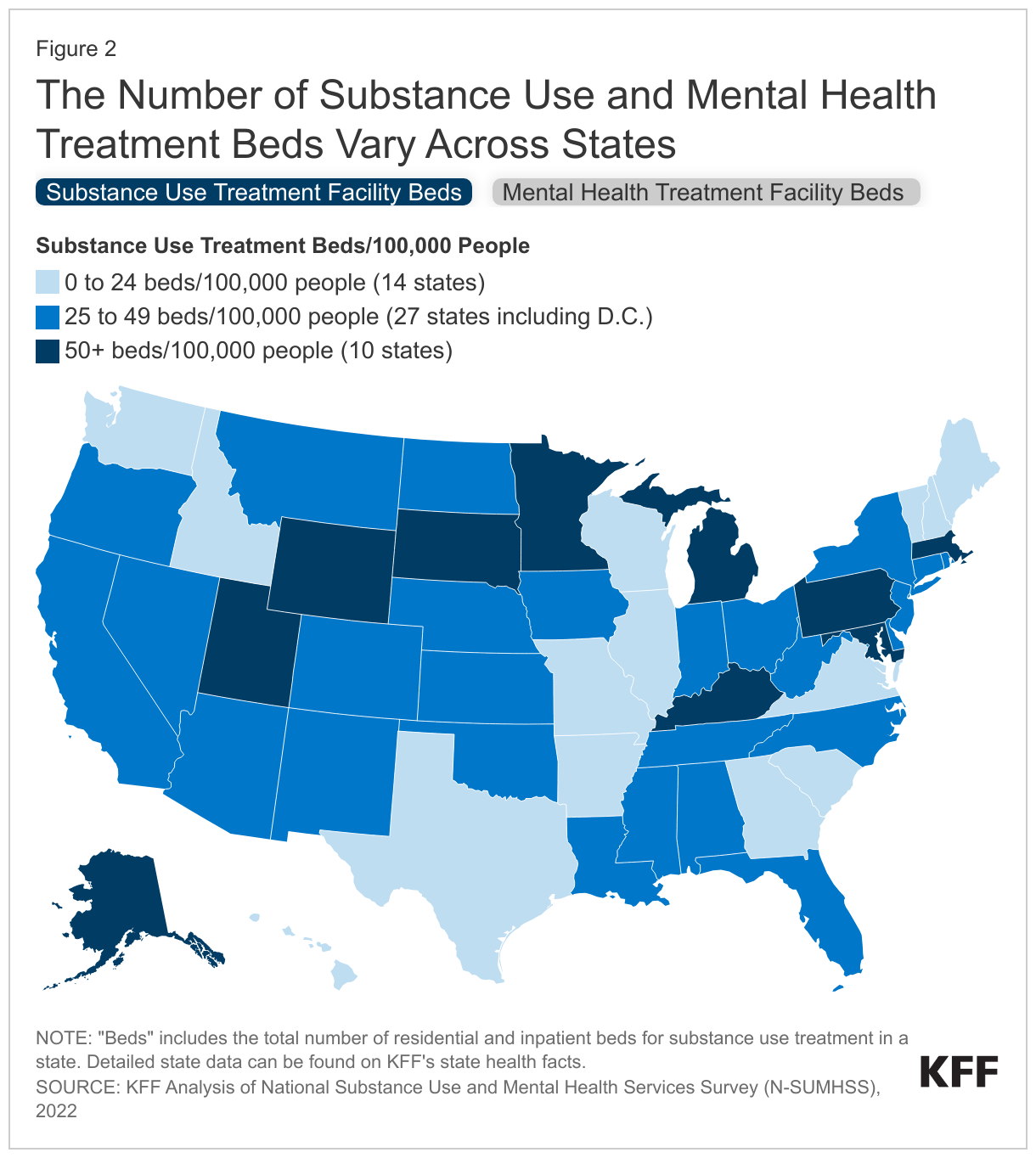
Substance use treatment and mental health bed availability varies across states. Nationally, substance use treatment beds average 34 beds per 100,000 and mental health beds average 29 beds per 100,000 people. These rates include both residential and outpatient beds. Across states, substance use treatment beds range from a low of 8 beds up to 79 beds per 100,000 people, and approximately one-third of states have less than 25 beds per 100,000 people for substance use treatment. For mental health treatment, the number of mental health treatment beds ranges from 14 beds to 69 beds per 100,000 people.
Ownership models
Facilities operate under different ownership models, including private for-profit, non-profit, and public or government ownership. These ownership models may influence facility management, including in areas such as staffing decisions and types of services offered, which can in turn affect the quality of care and patient outcomes. Ownership models have received particular attention in recent years due to the growth of for-profit private equity firms acquiring healthcare practices, which some research has linked to changes in quality and outcomes. There is increasing evidence that for-profit ownership in certain behavioral health facilities is growing, and private equity firms are showing greater interest in and acquiring more behavioral health facilities.
Most substance use and mental health treatment facilities are non-profit; however, for-profit ownership is more common among substance use treatment facilities, whereas public ownership is more common among mental health facilities. The share of for-profit substance use treatment facilities was double that of mental health facilities (43% compared to 19%) while the share of public or government-owned mental health facilities was double compared to substance use treatment (18% compared to 9%). For substance use treatment facilities, about 48% of facilities operate under non-profit ownership models and 43% operate under for-profit ownership models. Additionally, about 9% of substance use treatment facilities are owned and operated by a government or public agency. In health care, more broadly, hospitals have a 24% for-profit, 58% non-profit, and 18% government ownership distribution, a pattern that aligns closely with mental health facility ownership distribution but diverges from the ownership distribution of substance use treatment facilities.
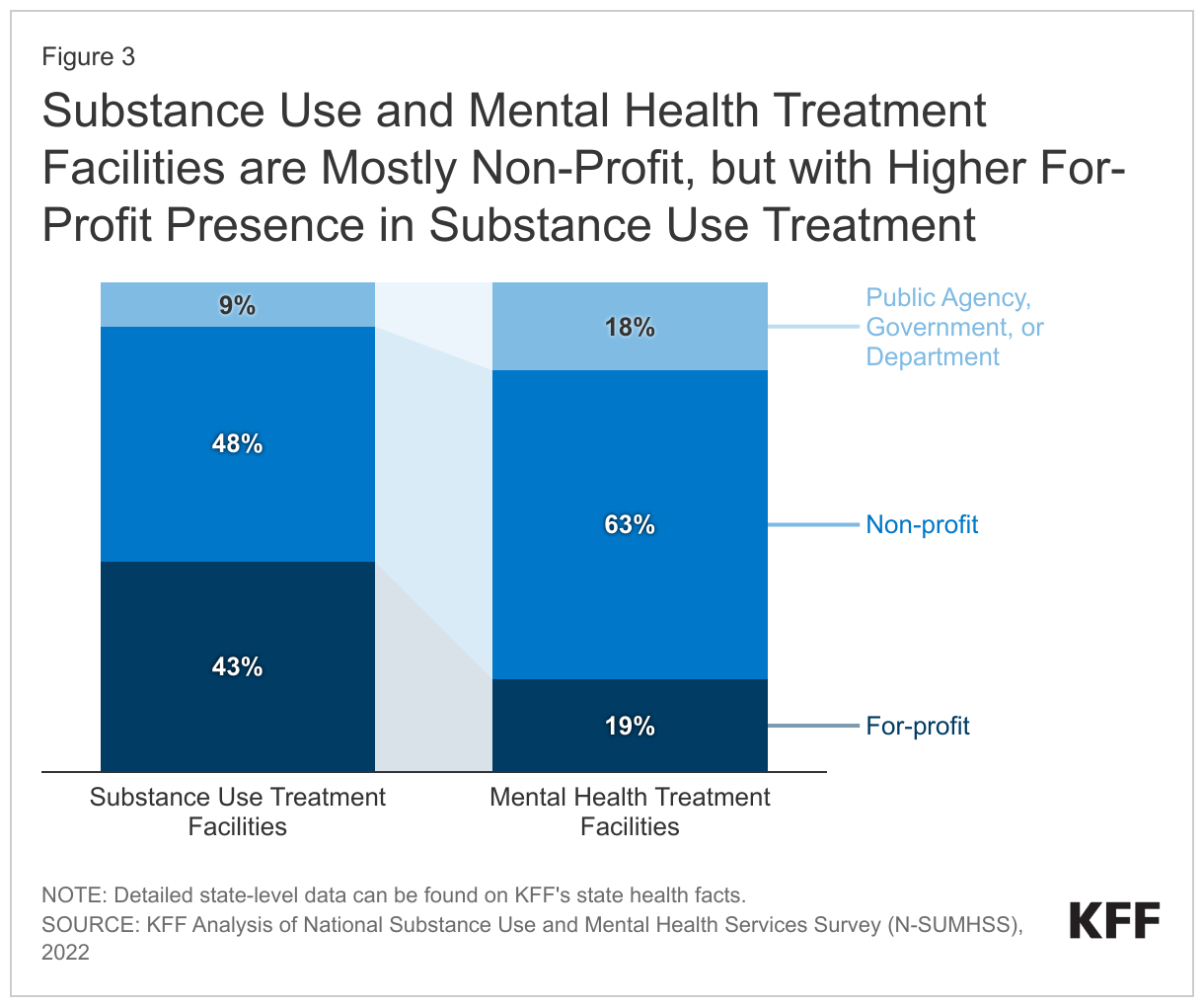
Notably, the distribution of ownership type varies substantially at a state level. For-profit ownership ranges from 10% in Alaska to 75% in Idaho. Among mental health treatment facilities, 63% are non-profit, while 19% are for-profit, and government or public agencies own about 18% of these facilities. At a state level, government or public ownership itself varies across states, from a low of 2% in Maine up to 82% in South Carolina.
Participation with insurers
Substance use and mental health treatment facilities choose to participate with specific insurance types and health plans, which directly impacts patient access to services. Most patients cannot afford to pay for care out-of-pocket and rely on health insurance, making the acceptance of their insurance a key factor in access to care. Medicaid enrollees may be particularly affected, as they often have behavioral health conditions coupled with low incomes, making out-of-pocket payments unfeasible. However, a facility’s stated insurance participation doesn’t always guarantee access. Some facilities might not accept new patients or may limit the number they accept based on their insurance type, such as Medicare or Medicaid, which may offer lower payment rates for care than private insurance.
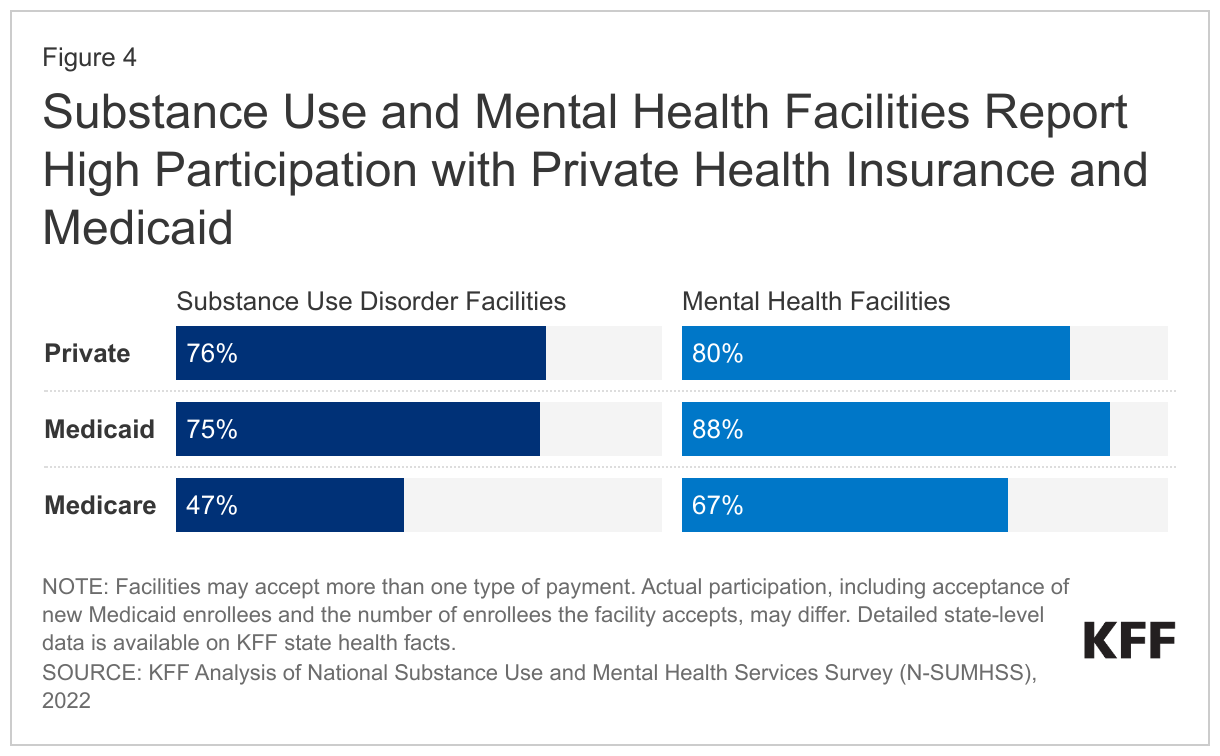
Most facilities report high participation with private insurance and Medicaid, but lower for Medicare and there is variation across states. Smaller shares of facilities report participation with Tricare or Indian Health Service. Nationally, 41% of substance use treatment facilities and 46% of mental health treatment facilities report participation with federal military insurance (such as Tricare), and 12% of substance use treatment facilities and 8% of mental health treatment facilities indicate acceptance of Indian Health Service/Tribal/Urban funds. However, since these payers represent a much smaller share of overall coverage and payments and there is considerable geographic variation in populations covered by these insurance types, these data are not shown in the figure. Across payer types, these data show the facility’s reported participation, but this might not be an accurate measure of access, as some facilities may not take new patients or limit the number of patients by payer (like Medicare or Medicaid).
Notably, 5% of substance use treatment facilities operate on a self-pay basis only, not participating in any insurance.
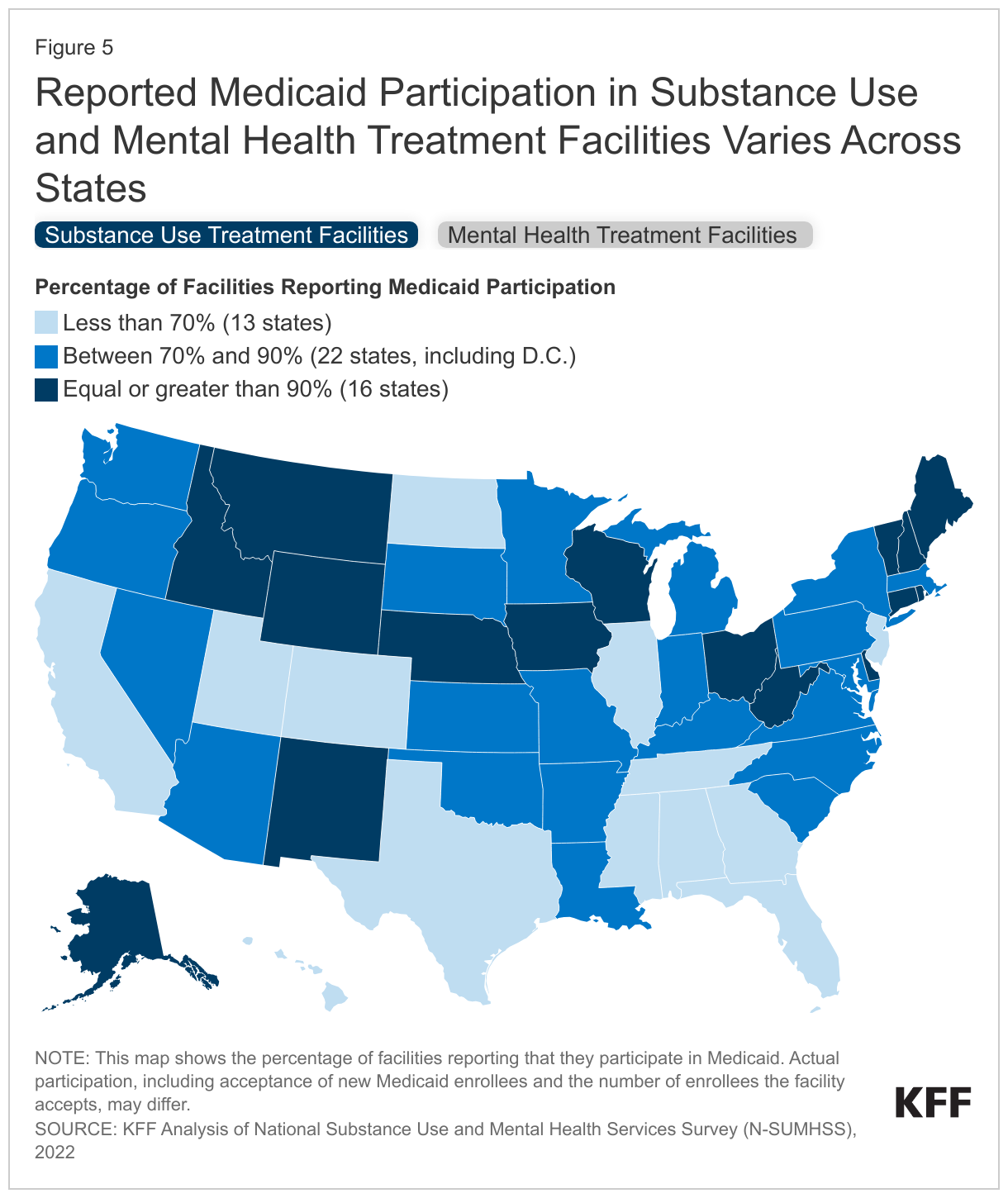
Reported Medicaid participation by substance use treatment facilities varies across states. In thirteen states, less than 70% of the state’s substance use treatment facilities report participation in Medicaid. Conversely, 16 states report that 90% or more of their substance use treatment facilities participate in Medicaid. The share of mental health treatment facilities reporting Medicaid participation is generally higher than for substance use treatment facilities. There may be a number of factors that affect the variation in Medicaid participation rates across states, including varying rules around Medicaid reimbursement for residential and inpatient care provided in facilities considered “Institutions of Mental Disease.”
Looking Ahead
Substance use and mental health treatment facilities vary in the services they offer, their ownership structures, and the insurance plans in which they participate. These differences may be influenced by the unique policies in each state and the specific needs of their populations. Currently, there’s no agreement on the ideal mix of these factors for these facilities, but wide reports of difficulty accessing care fuel policy conversations in this area. As understanding grows and new delivery methods and standards are introduced, the types of services and characteristics of these facilities may also change. For example, implementation of 988 and a robust crisis response system may reduce reliance on inpatient psychiatric facilities. Access to services not only relies on the availability of facilities and beds but also on the presence of a behavioral health workforce to keep facilities operational and to provide treatment services.
| Methods |
| This analysis uses data from the 2022 National Substance Use and Mental Health Services Survey (N-SUMHSS). N-SUMHSS is an annual survey of all substance use and mental health treatment facilities in the United States, its territories, and the District of Columbia, administered by the Substance Abuse and Mental Health Services Administration (SAMHSA). It provides information on the number, characteristics and utilization of approximately 14,850 substance use treatment facilities and 9,580 mental health treatment facilities that are eligible for the SAMHSA N-SUMHSS reports, which excludes Department of Defense military mental health treatment facilities, individual private practitioners or small group practices not licensed as a substance use and/or mental health clinic, and jails/prisons. This analysis drops facilities located in the U.S. territories, for a total analytic sample of 14,774 substance use facilities and 9,536 mental health facilities. VA facilities are included in this analysis (n=392).
The national response rate for substance use treatment facilities in the 2022 N-SUMHSS is 86.8%. However, this varies by state. The state with the lowest response rate for substance use treatment facilities is Idaho, with 75.2% of facilities responding. West Virginia has the highest response rate with 94% of its substance use treatment facilities responding to the survey. Among mental health treatment facilities, the nationwide response rate is 82.9%. States range from a response rate of 67.9% in the District of Columbia to 94.5% in New Mexico for their mental health treatment facilities. The overall response rate for both substance use and mental health treatment facilities was 88.0%. |