5 Key Facts About Medicaid Coverage for Adults with Mental Illness
 Options under consideration in Congress to significantly reduce Medicaid spending could have major implications for adults who live with mental illness. Nationwide, an estimated 52 million nonelderly adults live with mental illness, and Medicaid covers nearly one in three (29%) of them, or about 15 million adults. Changes to Medicaid under consideration include imposing a per capita cap on federal spending, reducing the federal government’s share of costs for the ACA expansion group, and imposing work requirements. Such policy changes would fundamentally alter how Medicaid financing works and large federal spending reductions would force states to make tough choices on whether to raise new revenue, restrict the number of people covered, cover fewer benefits, or cut payment rates for physicians, hospitals, and other providers. For people with mental illness, losing Medicaid coverage would reduce access to mental health treatment and other health care, which could have negative implications for their mental and physical health.
Options under consideration in Congress to significantly reduce Medicaid spending could have major implications for adults who live with mental illness. Nationwide, an estimated 52 million nonelderly adults live with mental illness, and Medicaid covers nearly one in three (29%) of them, or about 15 million adults. Changes to Medicaid under consideration include imposing a per capita cap on federal spending, reducing the federal government’s share of costs for the ACA expansion group, and imposing work requirements. Such policy changes would fundamentally alter how Medicaid financing works and large federal spending reductions would force states to make tough choices on whether to raise new revenue, restrict the number of people covered, cover fewer benefits, or cut payment rates for physicians, hospitals, and other providers. For people with mental illness, losing Medicaid coverage would reduce access to mental health treatment and other health care, which could have negative implications for their mental and physical health.
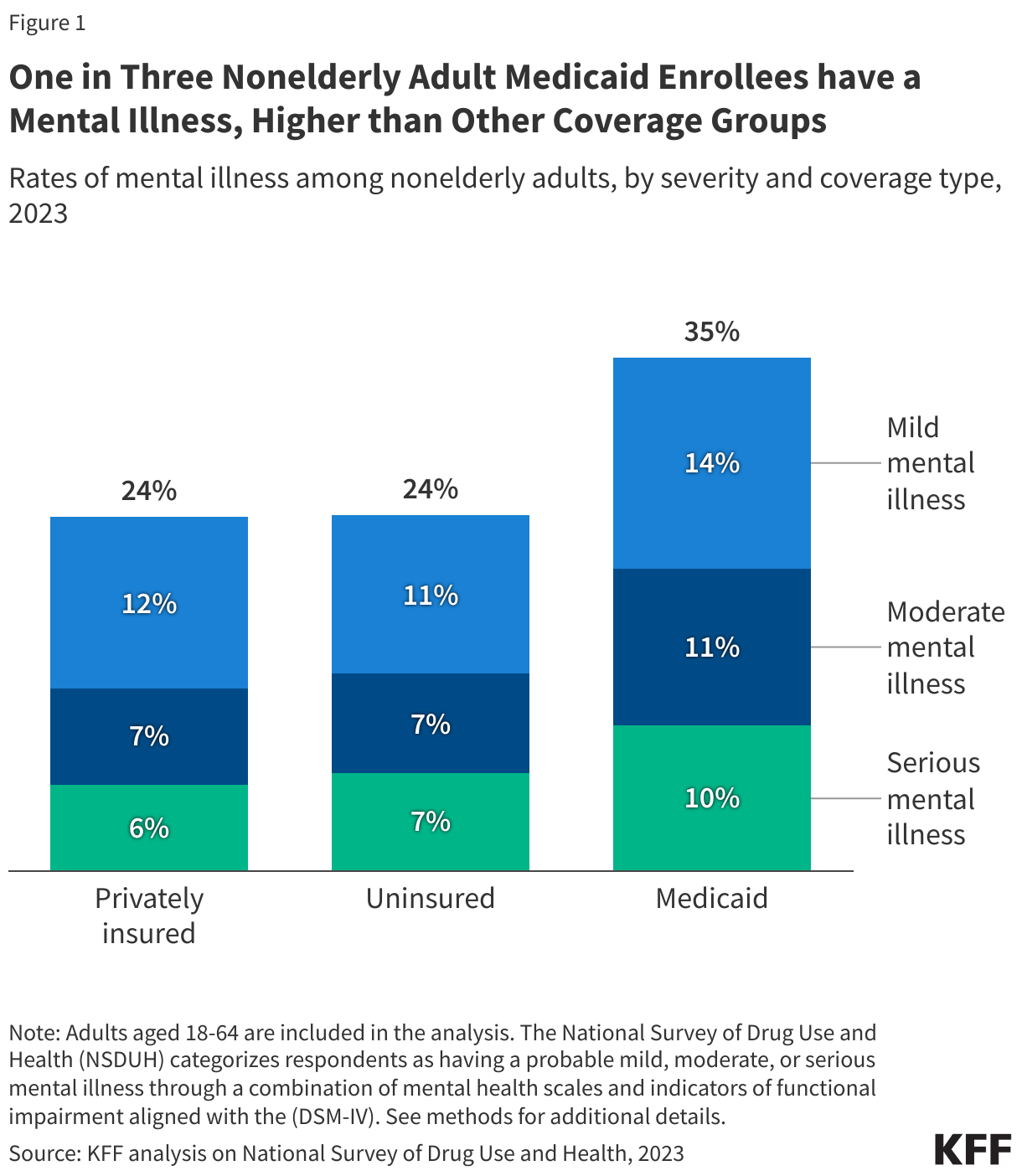
1. More than one in three adult Medicaid enrollees have a mental illness.
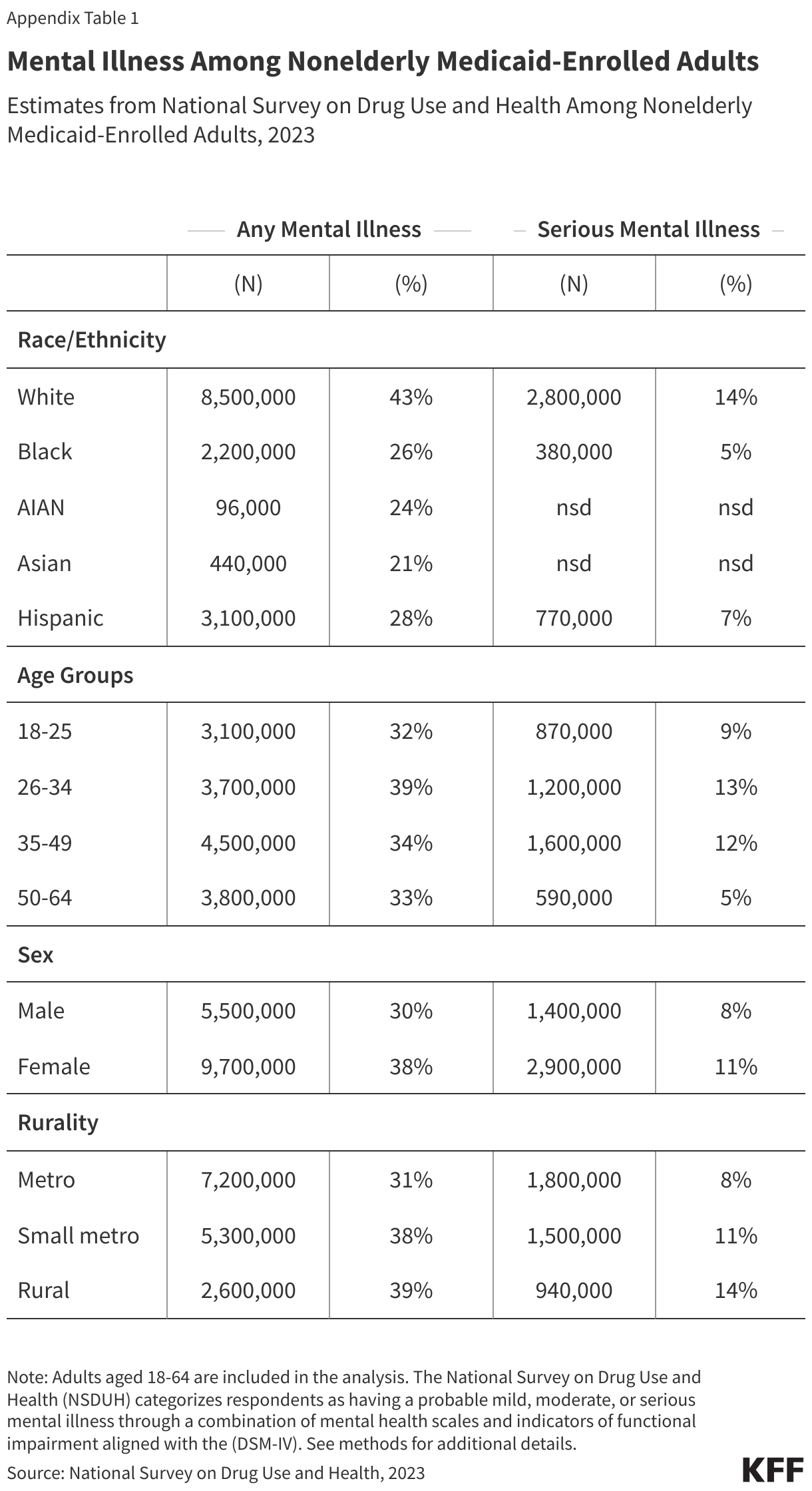
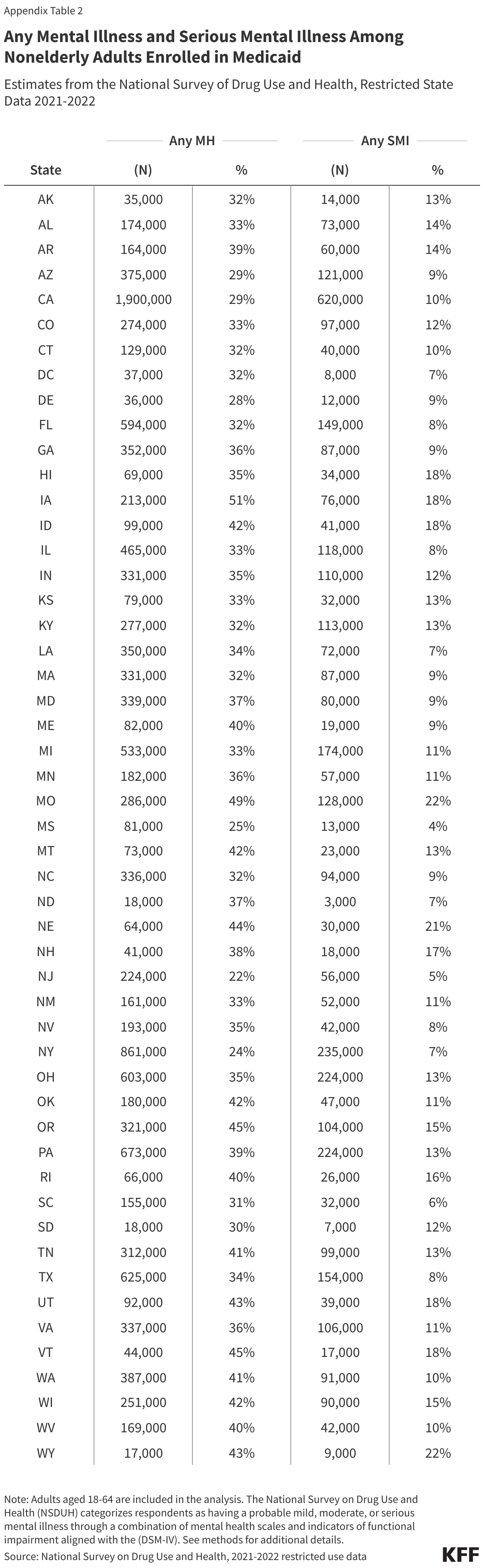
More than one in three nonelderly adults enrolled in Medicaid have a mental illness (35%), including 10% with a serious mental illness. These rates are higher than the rates among adults with private insurance or no coverage (Figure 1). Serious mental illness generally involves more severe symptoms and may include other neurological factors, both of which can complicate treatment and impact daily functioning. Data in Figure 1 come from the National Survey on Drug Use and Health (NSDUH), which categorizes respondents as having a probable mild, moderate, or serious mental illness through a combination of mental health scales and indicators of functional impairment. Generally, adults with severe symptoms and with greater impairments in daily functioning would meet the threshold for serious mental illness, while “any mental illness” includes adults who meet criteria for mild, moderate or serious mental illness (see methods). Among Medicaid adults, any mental illness is most prevalent among White adults, rural or small metro residents, those aged 26-34, and females (Appendix Table 1). Rates of any mental illness among adult Medicaid enrollees vary widely by state, from 22% in New Jersey to 51% in Iowa. Similarly, the percentage of adult Medicaid enrollees with a serious mental illness ranges from 4% in Mississippi to 22% in Wyoming and Missouri (Appendix Table 2).
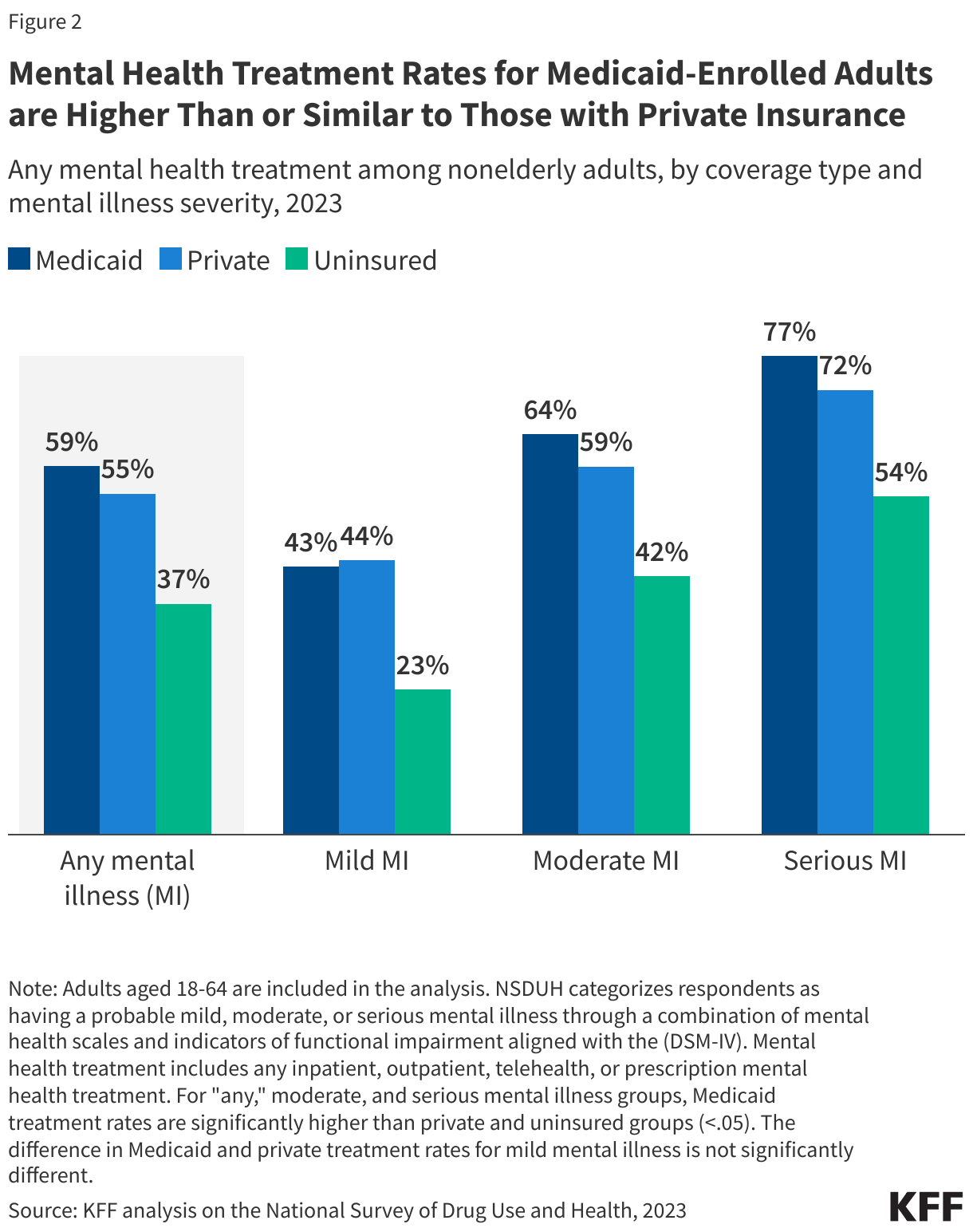
2. Mental health treatment rates for Medicaid-enrolled adults are higher or similar to those with private insurance.
Nonelderly adults in Medicaid receive mental health treatment at rates that are higher or similar to those with private insurance, and much more often than those who are uninsured. In 2023, 59% of adult Medicaid enrollees with any mental illness received treatment – somewhat above the rate for privately insured adults (55%) and far higher than for those who are uninsured (37%). Across all coverage types, treatment rates increased with the illness severity, with adults diagnosed with serious mental illness reporting the highest rates of treatment. Although adults with mild mental illness covered by Medicaid or private insurance report similar treatment rates, Medicaid-enrolled adults with moderate and serious mental illnesses report higher treatment rates than those with private coverage. In every category, adults with either Medicaid or private insurance receive treatment at much higher rates than those who lack health coverage. These data indicate only that care was accessed, not the adequacy or quality of that care. In an effort to increase access to care, many state Medicaid programs have expanded covered services and adopted policies to address workforce shortages.
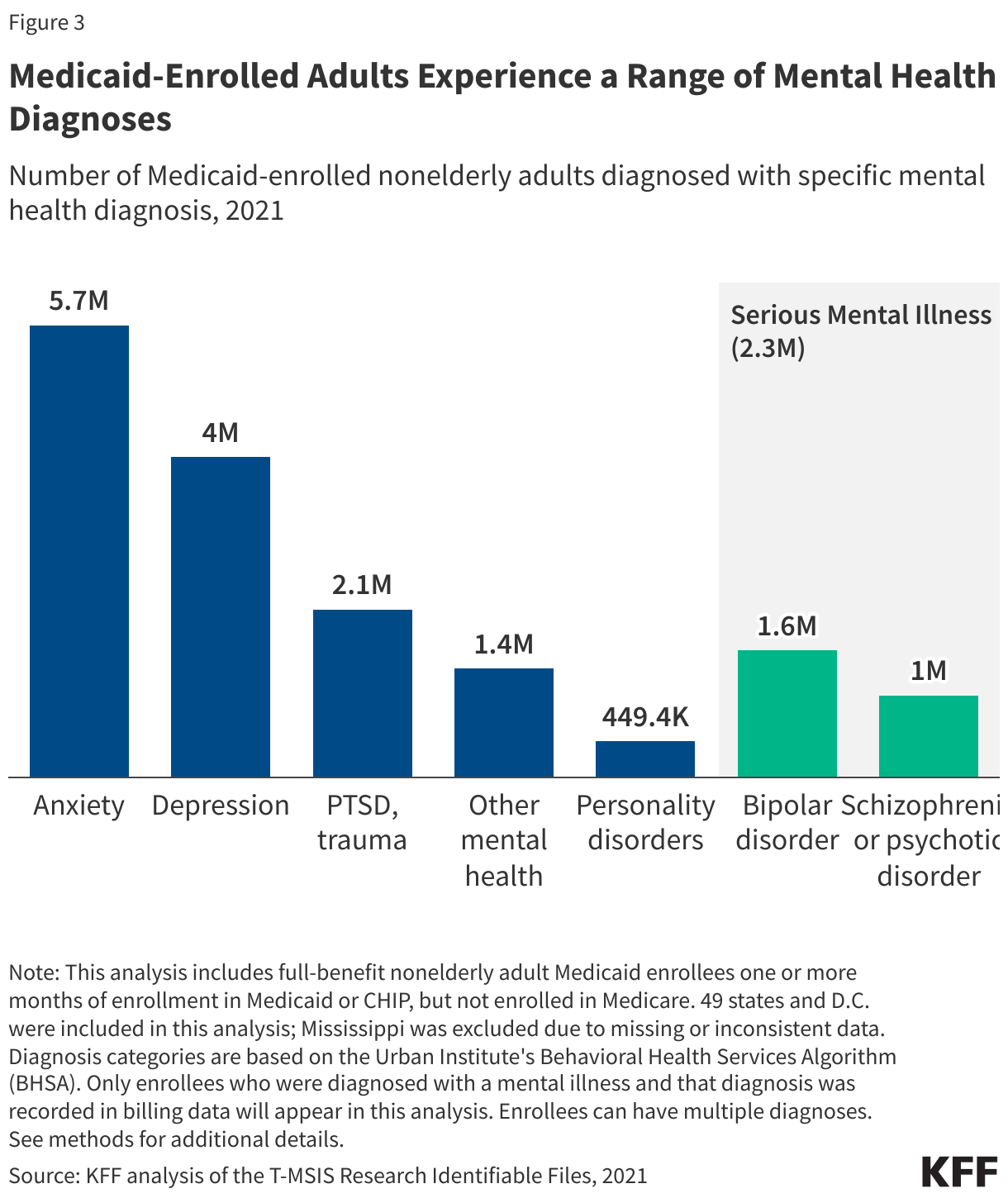
3. Adults enrolled in Medicaid experience a range of mental health diagnoses.
Anxiety and depressive disorders are the most frequently diagnosed mental illnesses among nonelderly Medicaid-enrolled adults (over 5 million diagnoses for anxiety alone). Serious mental illnesses – such as bipolar disorder and schizophrenia or other psychotic disorders – were diagnosed in over 2.3 million adult Medicaid enrollees (Figure 3). Many people experience overlapping mental health conditions (e.g., a person with depression may also have anxiety). Estimates of the number of people with specific types of mental illnesses come from Medicaid administrative data (i.e. claims data) which only capture diagnoses for people with a mental illness diagnosis recorded in their medical claims. This is not a measure of overall prevalence of mental illness because not everyone is screened, and diagnoses are not always recorded. Prevalence rates estimated through surveys are generally higher than the prevalence rates observed in claims data.
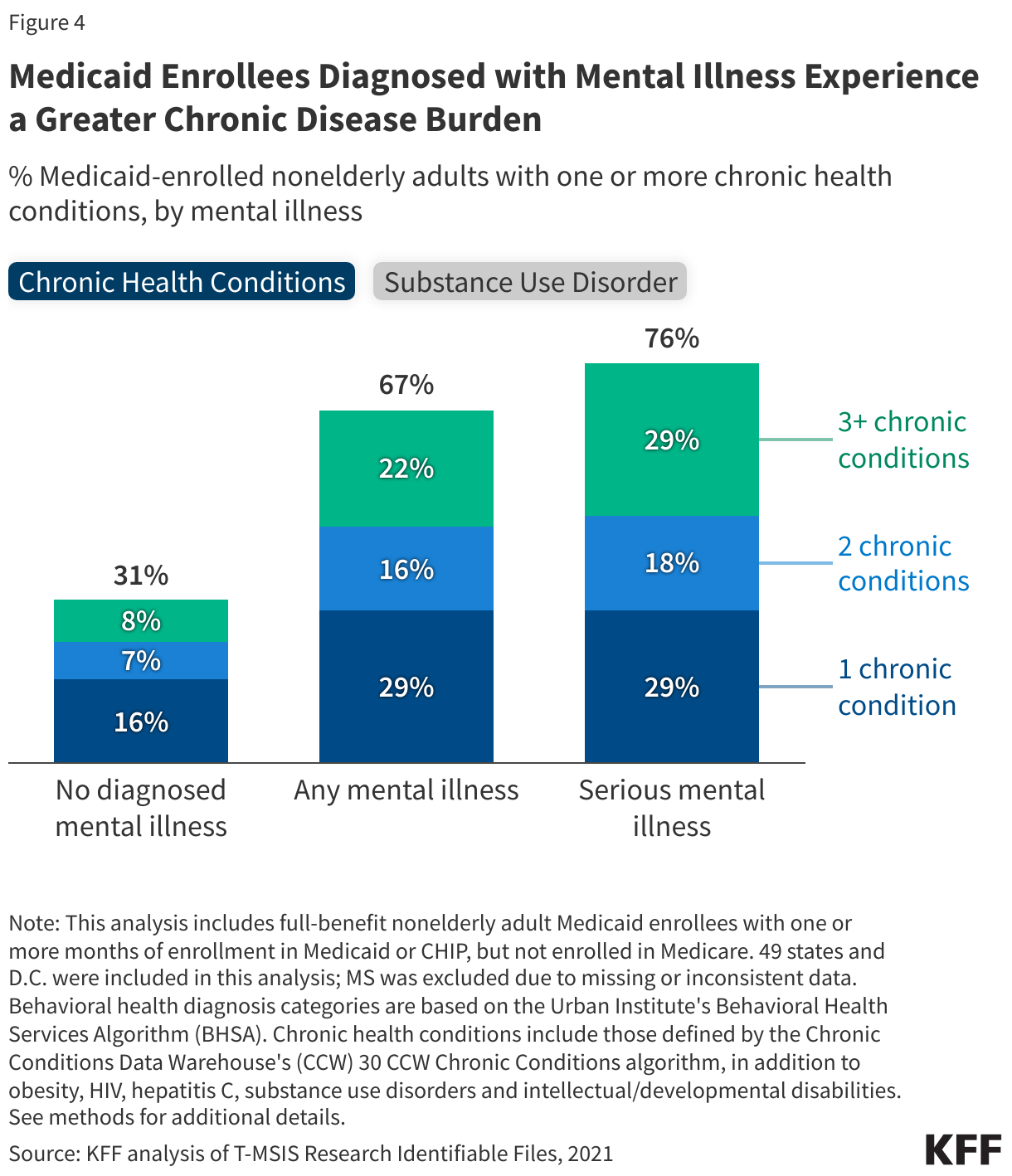
4. Medicaid enrollees with mental illness have higher rates of chronic conditions.
Medicaid enrollees diagnosed with mental illness have higher rates of chronic conditions and substance use disorder compared to those without a mental health diagnosis. Approximately two-thirds of adult enrollees with any mental illness have at least one other chronic condition – twice the rate of those without a diagnosed mental illness (Figure 4). Enrollees with serious mental illness have the highest rates of chronic conditions with 76% having at least one chronic condition. Chronic conditions are those that last at least a year and require ongoing medical care or limit daily activities, such as heart disease, diabetes, cancer, and mental illnesses. The most common chronic condition among Medicaid enrollees with mental illness is substance use disorder. These often overlap with mental illness, potentially due to shared risk factors. One in four enrollees diagnosed with any mental illness also have a diagnosed substance use disorder, and about 40% of those diagnosed with SMI do, compared to 5% of enrollees without a mental health diagnosis (Figure 4).
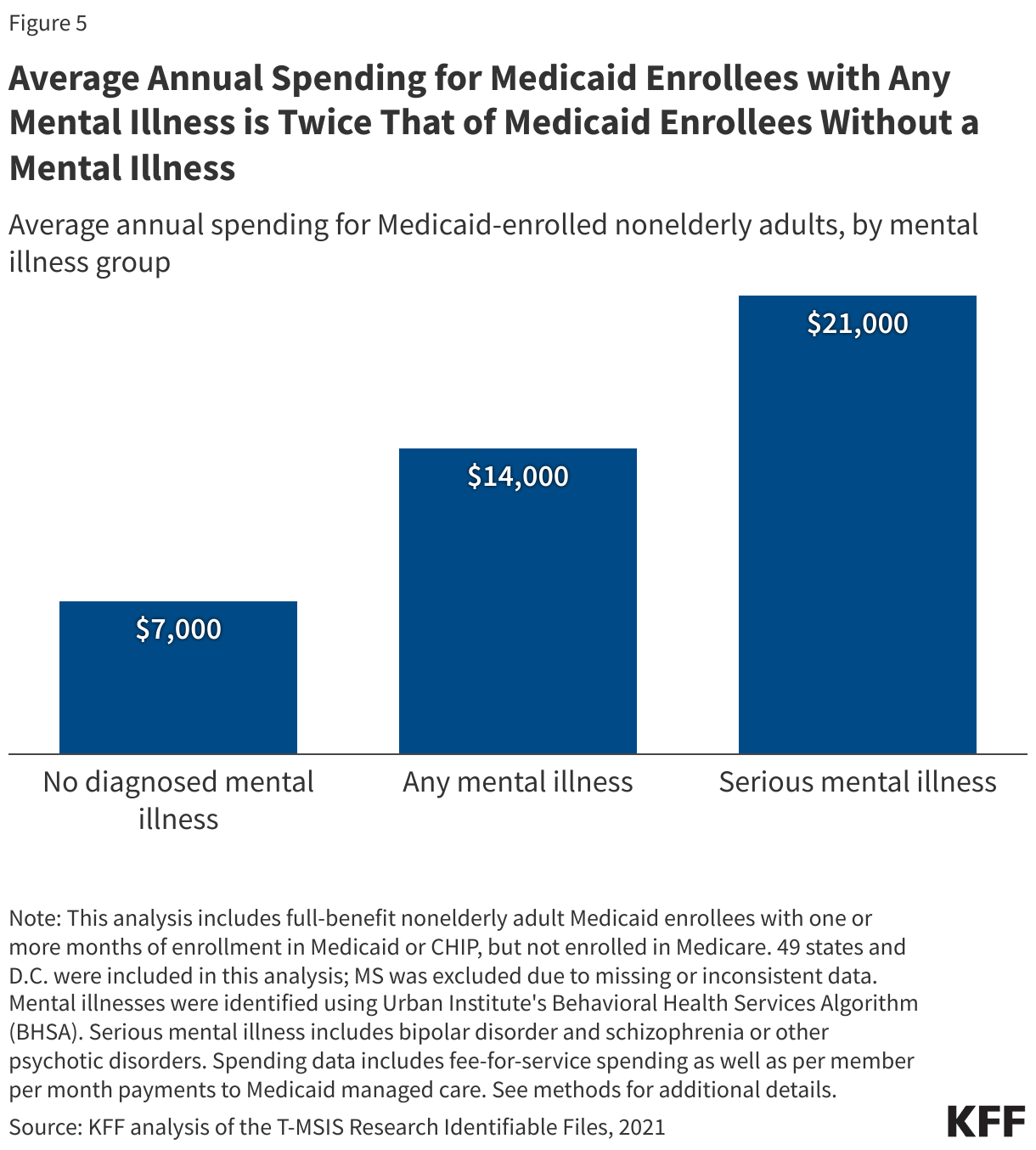
5. Average annual spending for enrollees with a mental illness is twice that of those without.
Average annual Medicaid spending per nonelderly adult enrollee is twice as high for those with any mental health diagnosis—about $14,000 per year—compared to roughly $7,000 for those without a mental health diagnosis. Spending is highest among adults diagnosed with a serious mental illness, at approximately $21,000 per enrollee per year—three times higher than the annual spending for those without a mental illness (Figure 5). Medicaid spending for adults with any mental illness accounts for one-third of the total Medicaid spending for non-elderly adults enrolled only in Medicaid. Higher rates of other chronic diseases among adults with mental illness may contribute to higher spending (Figure 3).
Appendix Tables
Methods |
| Medicaid Claims Data: This analysis used the 2021 T-MSIS Research Identifiable Files including the inpatient (IP), long-term care (LT), other services (OT), and pharmacy (RX) claims files merged with the demographic-eligibility (DE) files from the Chronic Condition Warehouse (CCW).
Identifying Mental Health, Serious Mental Health and Substance Use Disorder Diagnoses in Medicaid Claims Data:Mental illness, serious mental illness (SMI) and substance use disorder (SUD) diagnoses were identified using an algorithm adapted from the Behavioral Health Service Algorithm (BHSA) reference codes provided by The Urban Institute. The BHSA identifies these conditions with ICD-10 diagnosis codes, procedure codes, service codes, and National Drug Codes (NDCs). “Any mental illness” is a comprehensive category that includes the diagnosis of anxiety, depression, post-traumatic stress (PTSD) or other trauma disorders, personality disorders, bipolar disorders, schizophrenia/psychotic disorders, and/or other mental illnesses not fitting within these categories. “Any SMI” is a subcategory of any mental illness that specifies mental disorders that result in severe functional impairment. This analysis follows other literature and includes bipolar disorders and schizophrenia/psychotic disorders in the definition of SMI. “Any SUD” is a comprehensive category that includes alcohol, opioids, marijuana, inhalants, sedatives, hallucinogens, psychostimulants, and/or substances labeled as “other” or “unspecified” in claims data. See: Victoria Lynch, Lisa Clemans-Cope, Doug Wissoker, and Paul Johnson. Behavioral Health Services Algorithm. Version 4. Washington, DC: Urban Institute, 2024. Defining Chronic Conditions in Medicaid Claims Data: This analysis used the CCW algorithm for identifying chronic conditions (updated in 2020). This analysis also included in its definition of chronic conditions substance use disorder, obesity, HIV, hepatitis C, and intellectual and developmental disabilities (ASPE definition). Mental illness was not included the in the count of chronic conditions in Figure 4 since the analysis is stratified by mental illness. Enrollee Inclusion Criteria in Medicaid Claims Data:Enrollees were included if they were ages 18-64, had full Medicaid or CHIP coverage for at least one month, and were not dually eligible for Medicare. State Inclusion Criteria in Medicaid Claims Data: To assess the usability of states’ data, the analysis examined quality assessments from the DQ Atlas for OT claims volume and OT managed care encounters and compared the share of adults diagnosed with any mental illness (AMI) in each states’ Medicaid data to estimates for adult Medicaid enrollees from the 2021-2022 restricted National Survey on Drug Use and Health (NSDUH). States were excluded if: (1) they received a “High Concern/ Unusable” rating on the relevant DQ Atlas assessment measure, and (2) their Medicaid estimate of AMI differed from the NSDUH estimate by more than 15.1 percentage points (the 75th percentile of all differences). If at least 70% of a state’s Medicaid enrollees were covered by either managed care or by fee for service, only the corresponding DQ Atlas indicator was considered (i.e. managed care encounters volume or claims volume (FFS)). For states with more mixed delivery systems, both sets of indicators were considered; in these cases; a “High Concern/Unusable” rating on either measure, combined with a difference above 15.1 percentage points, led to exclusion. Based on these criteria, Mississippi was excluded, leaving 49 states and D.C. in the analysis. National Survey on Drug Use and Health. The National Survey on Drug Use and Health (NSDUH) is a nationally representative survey that, among other topics, collects information about symptoms of mental illness and related functional impairments from adult respondents. It uses a combination of mental health scales, suicidality symptoms, functional impairments and other indicators to classify respondents as having a probable mild, moderate, or serious mental illness. Thresholds for each category were developed by NSUDH through methodological work comparing survey responses with psychiatric clinical interviews using the DSM-IV diagnostic criteria. Adults whose responses meet or exceed the highest severity threshold are categorized as having a probable serious mental illness, which reflects greater functional impairment due to more severe mental illness symptoms. National data reported in this analysis uses the most recent NSDUH data (2023) to identify Medicaid enrollees ages 18-64 who meet DSM-IV criteria for any or serious mental illness. State-level data reported in Appendix Table 2 is drawn from the most recent state-level data publicly available (2021-2022 restricted NSDUH files). NSDUH generally reports higher rates of mental illness than claims-based data, as it includes people who have not received a formal diagnosis. Still, NSDUH may underestimate prevalence because it excludes people without an address (such as those who are unhoused, institutionalized, or incarcerated)–groups likely to have higher rates of mental illness. |