10 Things to Know About Medicaid
 Medicaid is the primary program providing comprehensive coverage of health and long-term care to 83 million low-income people in the United States. Medicaid accounts for one-fifth of health care spending, more than half of spending for long-term care, and a large share of state budgets. Medicaid is jointly financed by states and the federal government but administered by states within broad federal rules. Because states have a degree of flexibility to determine what populations and services to cover, how to deliver care, and how much to reimburse providers, there is significant variation across states in program spending and the share of state residents covered by the program.
Medicaid is the primary program providing comprehensive coverage of health and long-term care to 83 million low-income people in the United States. Medicaid accounts for one-fifth of health care spending, more than half of spending for long-term care, and a large share of state budgets. Medicaid is jointly financed by states and the federal government but administered by states within broad federal rules. Because states have a degree of flexibility to determine what populations and services to cover, how to deliver care, and how much to reimburse providers, there is significant variation across states in program spending and the share of state residents covered by the program.
At the start of 2025, many issues are at play that will affect Medicaid coverage, financing, and access to care. While Medicaid was not discussed much on the campaign trail, Congress may consider big changes as part of tax and spending debates and the Trump administration may make changes to Medicaid through executive actions. Amid the potential changes, this brief highlights ten key things to know about Medicaid.
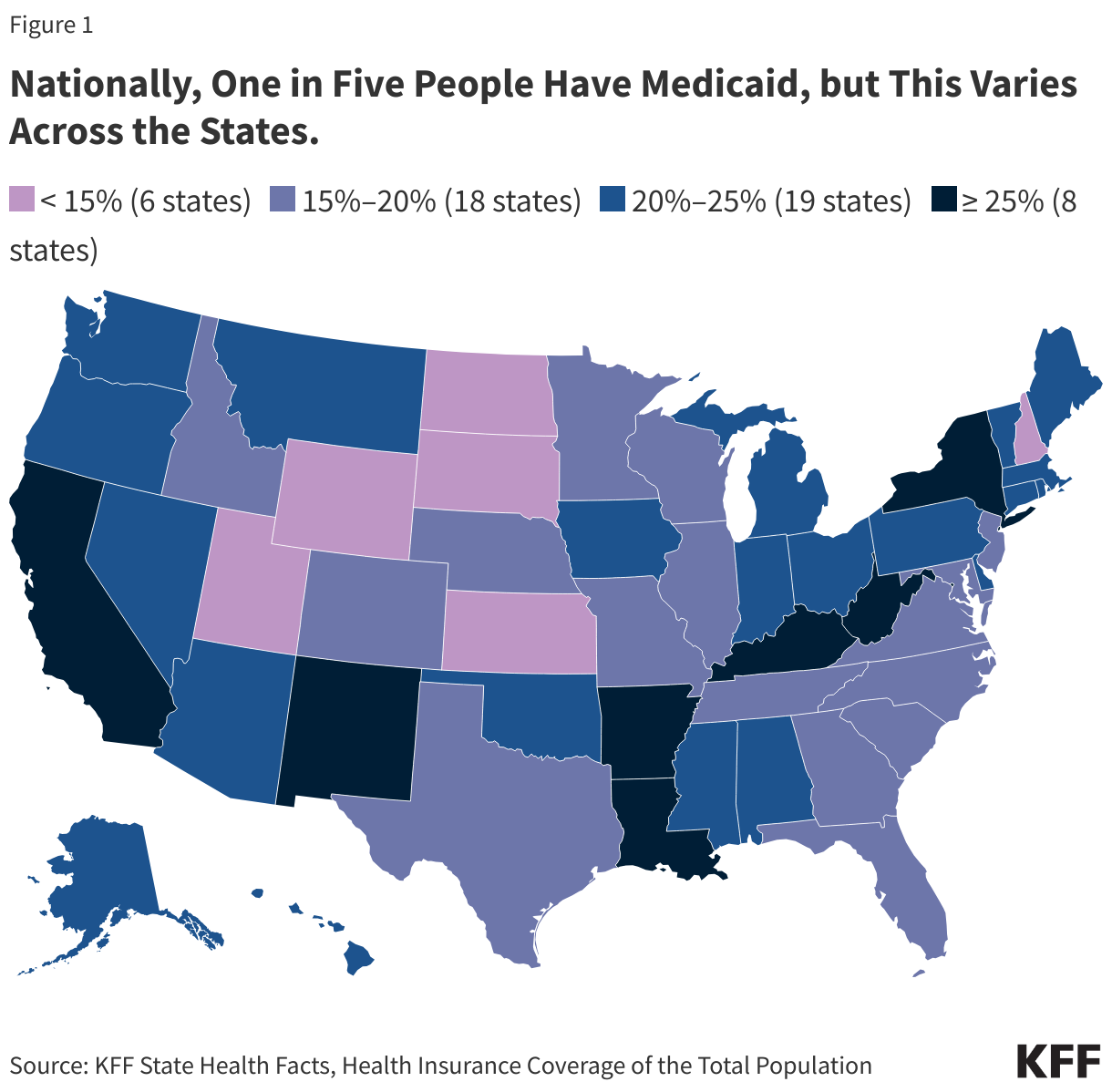
1. Nationally, one in five people have Medicaid, but this varies across the states.
The percentage of people who report having Medicaid is 21% nationally, but ranges from 11% in Utah to 34% in New Mexico (Figure 1). The percentage tends to be higher in the 41 states that expanded Medicaid under the Affordable Care Act (ACA), which includes 21 states that voted for Trump and 20 that voted for Harris. Rates of Medicaid coverage are also higher in states with lower average incomes and lower rates of health insurance offered through employers.
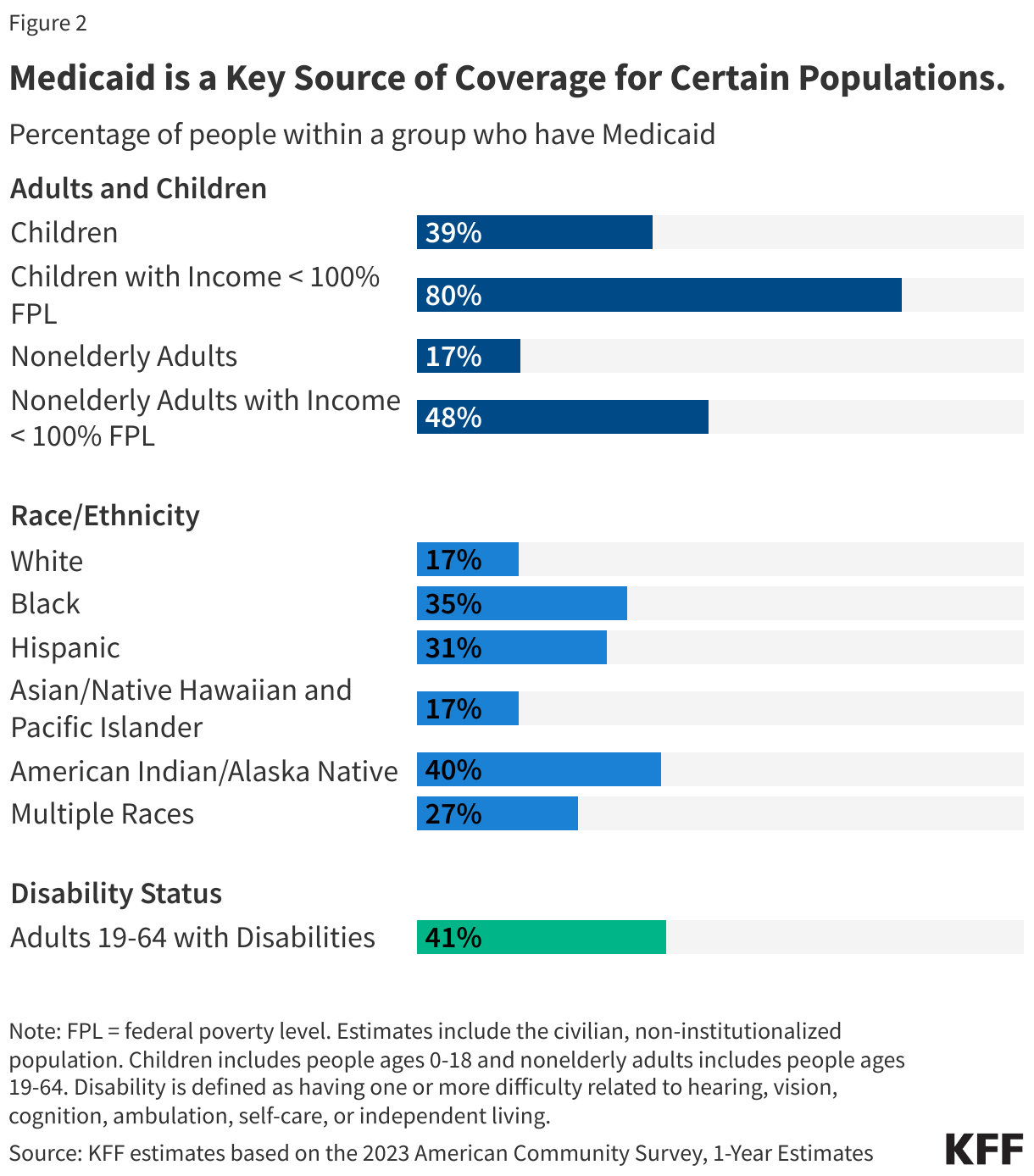
2. Medicaid is a key source of coverage for certain populations.
While Medicaid covers 1 in 5 people living in the United States, Medicaid is a key source of coverage for certain populations. In 2023, Medicaid covered nearly 4 in 10 children, over 8 in 10 children in poverty, 1 in 6 adults, and almost half of adults in poverty. Relative to White children and adults, Medicaid covers a higher share of Black, Hispanic, and American Indian or Alaska Native (AIAN) children and adults. Medicaid covers more than 1 in 4 adults ages 19-64 with disabilities, who are defined as having one or more difficulty related to hearing, vision, cognition, ambulation, self-care, or independent living (Figure 2).
Medicaid provides coverage for several special populations. For example, Medicaid covers 41% of all births in the United States, nearly half of children with special health care needs, 5 in 8 nursing home residents, 29% of non-elderly adults with any mental illness, and 40% of non-elderly adults with HIV. Medicaid pays Medicare premiums and often provides wraparound coverage for services not covered by Medicare (like most long-term care) for nearly 1 in 5 Medicare beneficiaries (13 million). Medicaid is a key source of coverage for individuals experiencing homelessness and those transitioning out of carceral settings, particularly in states that have adopted the Medicaid expansion.
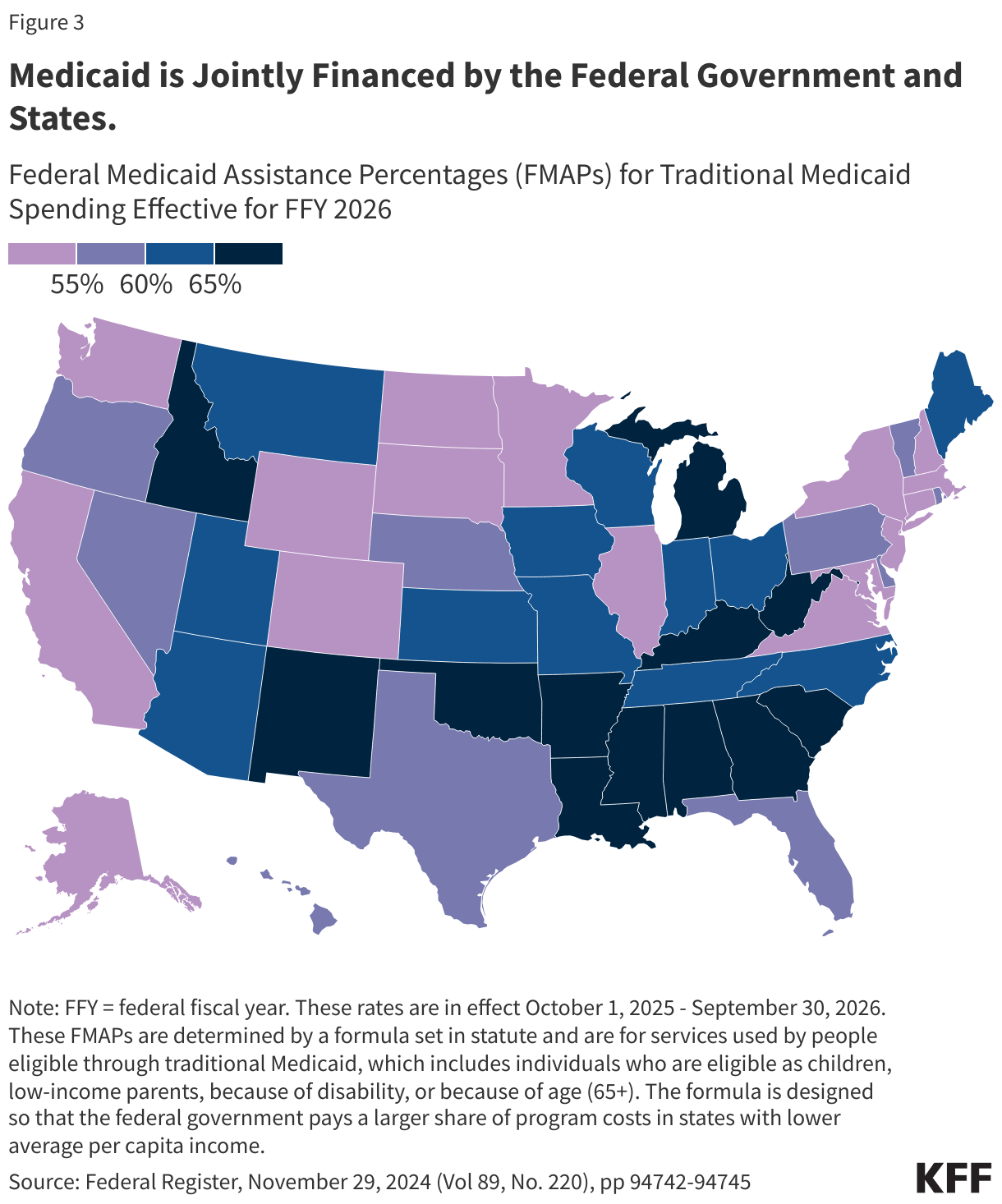
3. Medicaid is jointly financed by the federal government and states.
States are guaranteed federal matching dollars without a cap for qualified services provided to eligible enrollees. The match rate for most Medicaid enrollees is determined by a formula in the law that provides a match of at least 50% and provides a higher federal match rate for states with lower per capita income (Figure 2). States may receive a higher match rate for certain services and populations. The ACA expansion group is financed with a 90% federal match rate, so states pay 10%; however, the American Rescue Plan Act included an additional temporary fiscal incentive to states that newly adopt the Medicaid expansion. In FY 2023, Medicaid spending totaled $880 billion of which 69% was federal spending. Total Medicaid spending typically accelerates during economic downturns because people may lose income and enroll in the program. To help states manage increased costs, the federal government has temporarily increased the federal share of Medicaid. Most recently, states received an increase in the match rate between 2020 and 2024 to help manage increased enrollment and costs due to the pandemic related continuous enrollment provision.
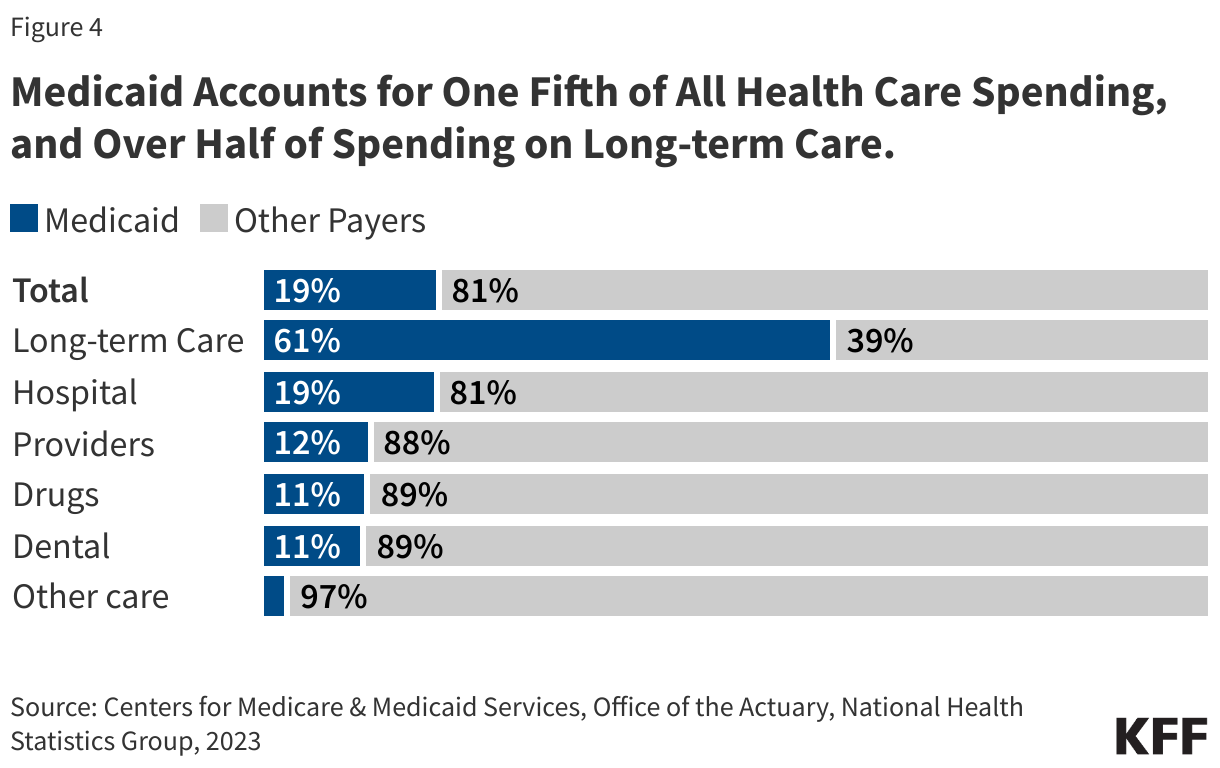
4. Medicaid accounts for one fifth of all health care spending, and over half of spending on long-term care.
Medicaid provides a major source of funding for the U.S. health care system, covering 19% of all health care spending and 19% of hospital spending (Figure 4). In addition to covering the services required by federal Medicaid law, all states elect to cover optional benefits including prescription drugs and home care. Home care, also known as home- and community-based services or HCBS, is long-term care provided in non-institutional settings including homes, day care centers, and assisted living facilities. Other long-term care is provided in institutions such as nursing facilities. Medicaid is the primary payer for long-term care in the United States, covering 61% of total spending. Beyond long-term care, Medicaid provides other benefits not usually covered by health insurance including non-emergency medical transportation, which helps enrollees get to appointments, and comprehensive benefits for children, known as Early Periodic Screening Diagnosis and Treatment (EPSDT) services.
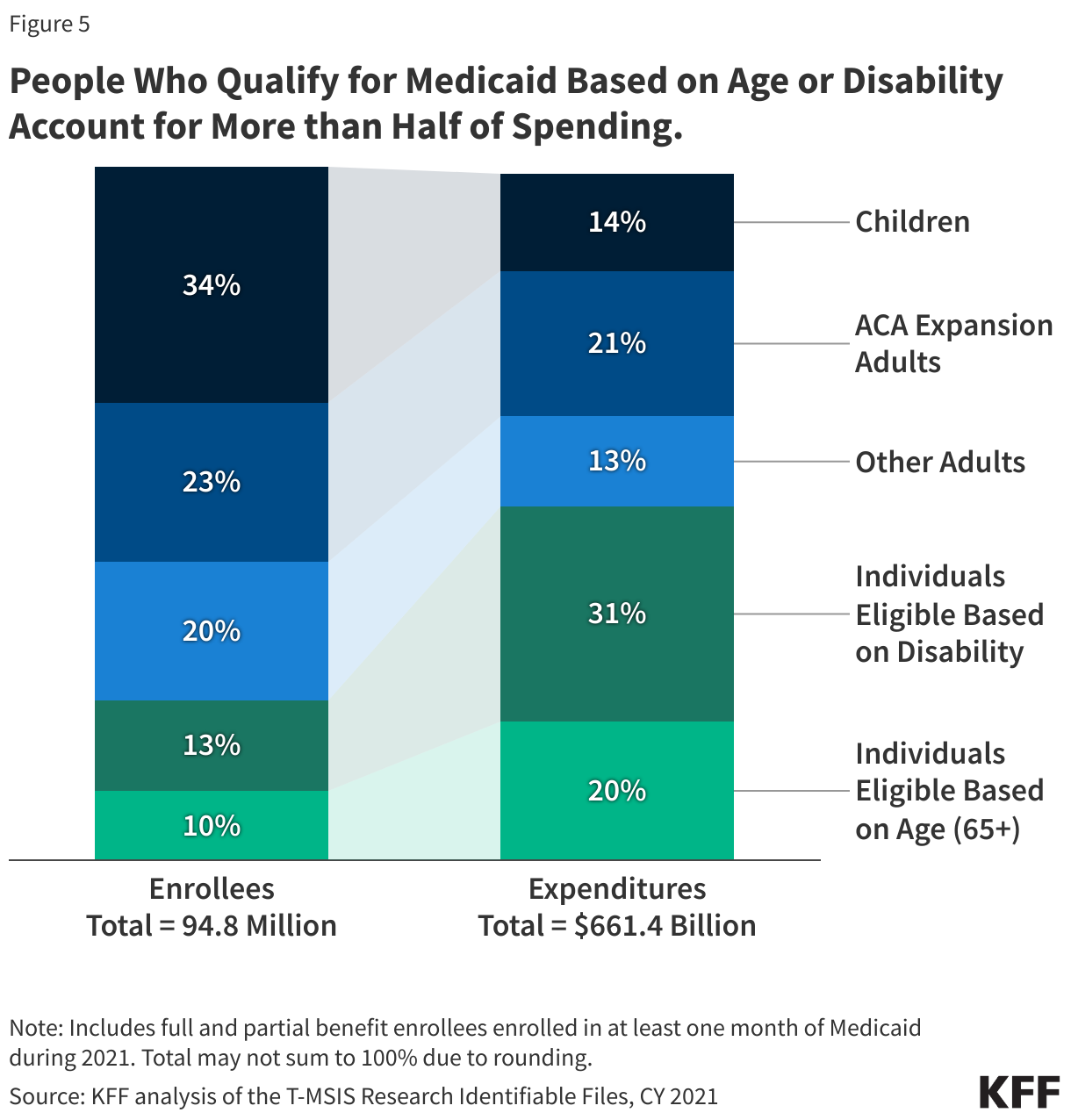
5. People who qualify for Medicaid based on age or disability account for more than half of spending.
Overall, seniors and individuals with disabilities account for 23% of enrollment but 51% of spending whereas children account for 34% of enrollment, but 14% of spending (Figure 5). The disproportionate spending on certain eligibility groups stems from variation in spending per enrollee across the eligibility groups. Spending per enrollee was highest for enrollees ages 65 and older ($18,923) and eligible because of disability ($18,437). Seniors and people with disabilities often have higher health care costs than other enrollees due to more complex health care needs, higher rates of chronic conditions and being more likely to utilize long-term care. There is significant state variation in the percentage of Medicaid spending that pays for enrollees eligible because of a disability or being age 65 and older: In some states (Alaska, Nevada, Montana, Illinois, and Indiana), only a third of spending went to those populations, and in five states (Alabama, Florida, Kansas, Mississippi, and North Dakota), care for people eligible because of disabilities or being over age 64 accounted for at least two-thirds of spending.
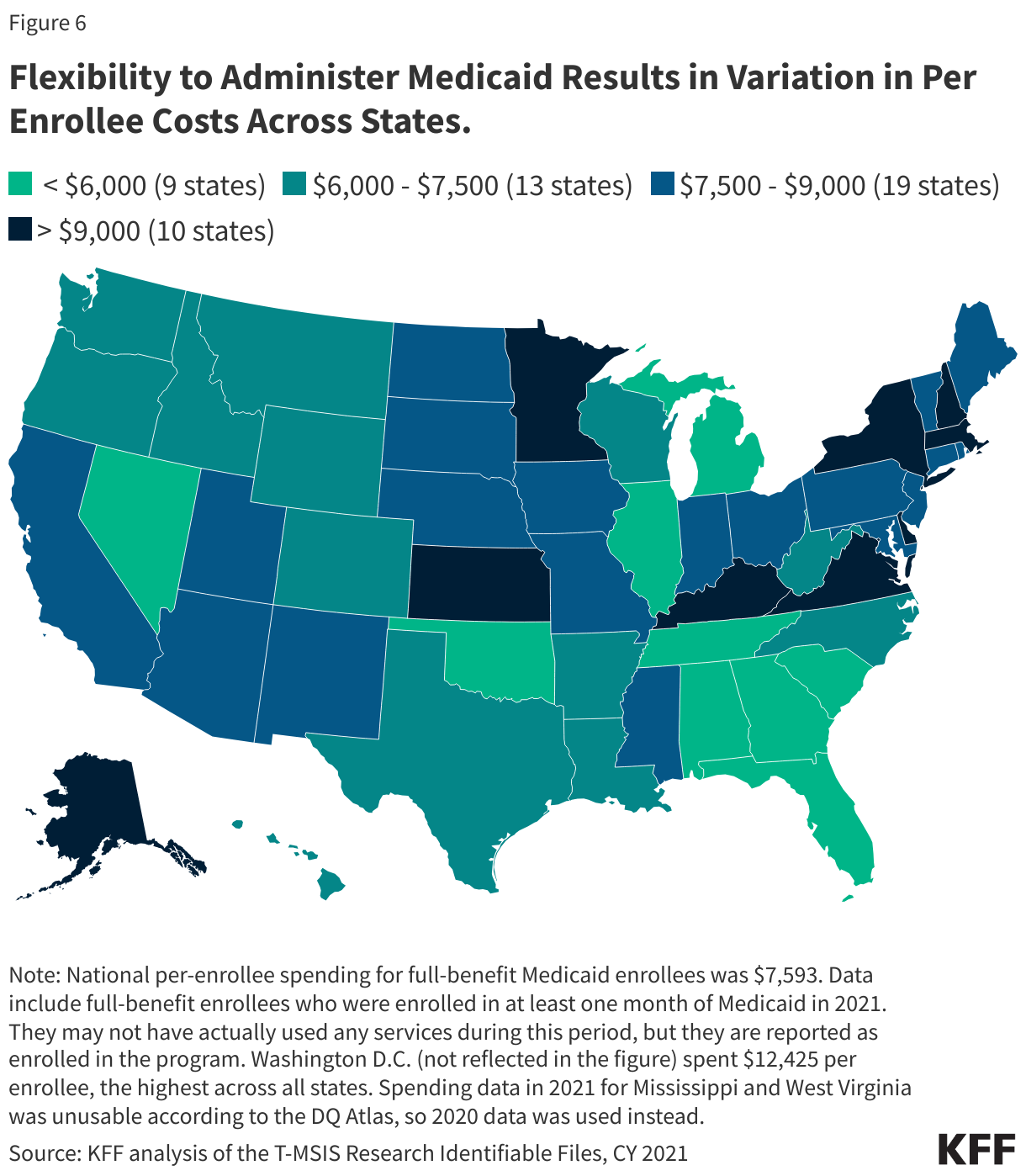
6. Flexibility to administer Medicaid results in variation in per enrollee costs across states.
Across the states, spending per full-benefit enrollee ranged from a low of $3,713 in Alabama to $10,229 in the District of Columbia in 2020 (Figure 6). Variation in spending across the states reflects considerable flexibility for states to design and administer their own programs – including what benefits are covered and how much providers are paid — and variation in the health and population characteristics of state residents as well as overall health care costs. Although all states are required to provide some Medicaid benefits, many others are optional, including prescription drugs (covered by all states), vision services, dental care and most home care. In recent years, states have expanded coverage of behavioral health services and benefits to help enrollees address social determinants of health (SDOH) like nutrition or housing.
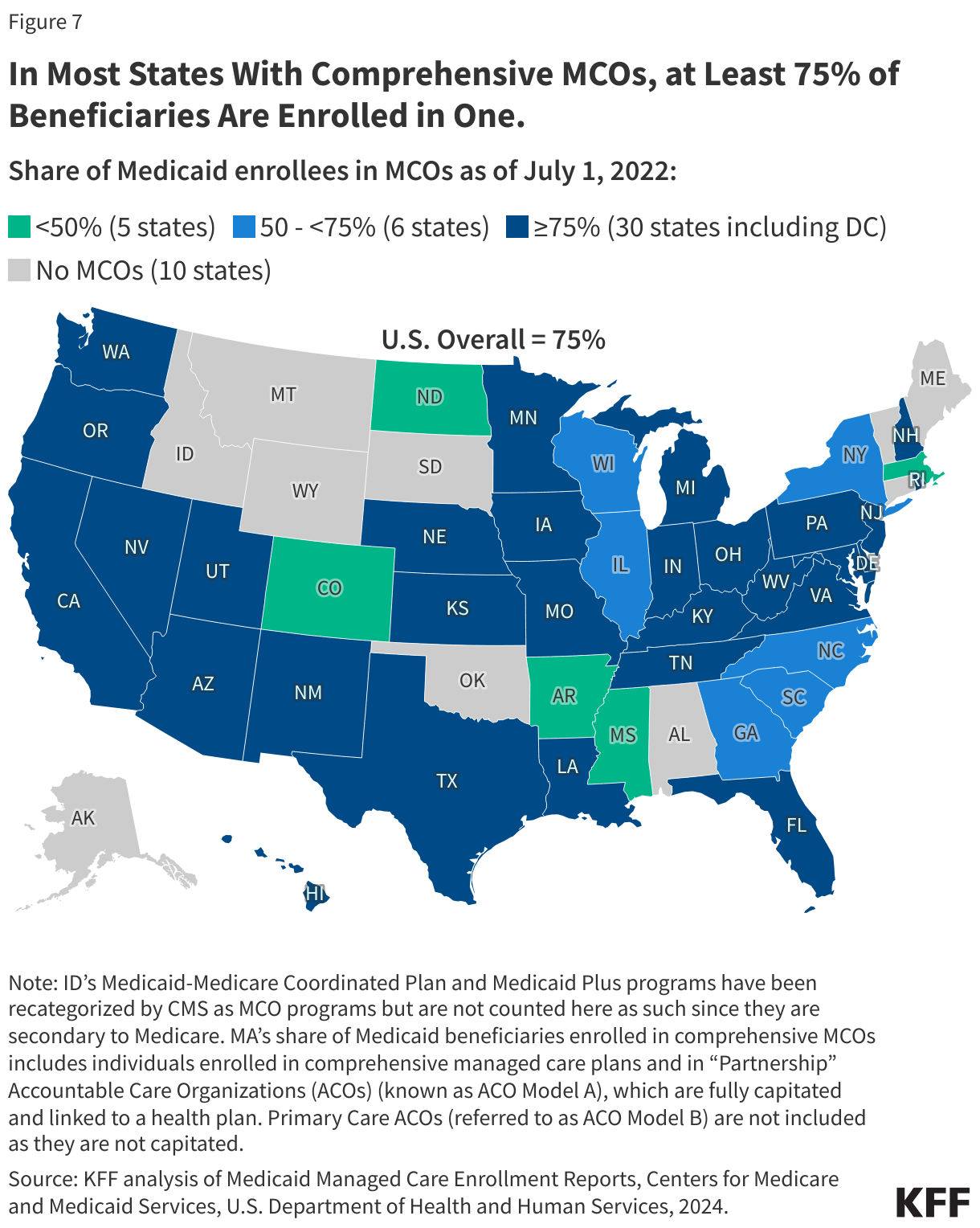
7. Three-quarters of all Medicaid enrollees receive care through comprehensive, risk-based MCOs.
Overall, 75% of all Medicaid enrollees receive care through comprehensive, risk-based managed care organizations (MCOs) (Figure 7). Payments to MCOs accounted for more than half (52%) of Medicaid spending in FY 2023. As of July 2024, 42 states (including DC) contract with comprehensive MCOs. Medicaid MCOs provide comprehensive acute care (i.e., most physician and hospital services) and in some cases long-term care to Medicaid enrollees and are paid a set per member per month payment for these services. Medicaid MCOs represent a mix of private for-profit, private non-profit, and government plans. Five for-profit parent firms (Centene, Elevance (formerly Anthem), UnitedHealth Group, Molina, and CVS) account for 50% of all Medicaid MCO enrollment. States have increased their reliance on MCOs with the aim of improving access to certain services, enhancing care coordination and management, and making future costs more predictable. While the shift to MCOs has increased budget predictability for states, the evidence about the impact of managed care on access to care, costs, and outcomes is both limited and mixed.
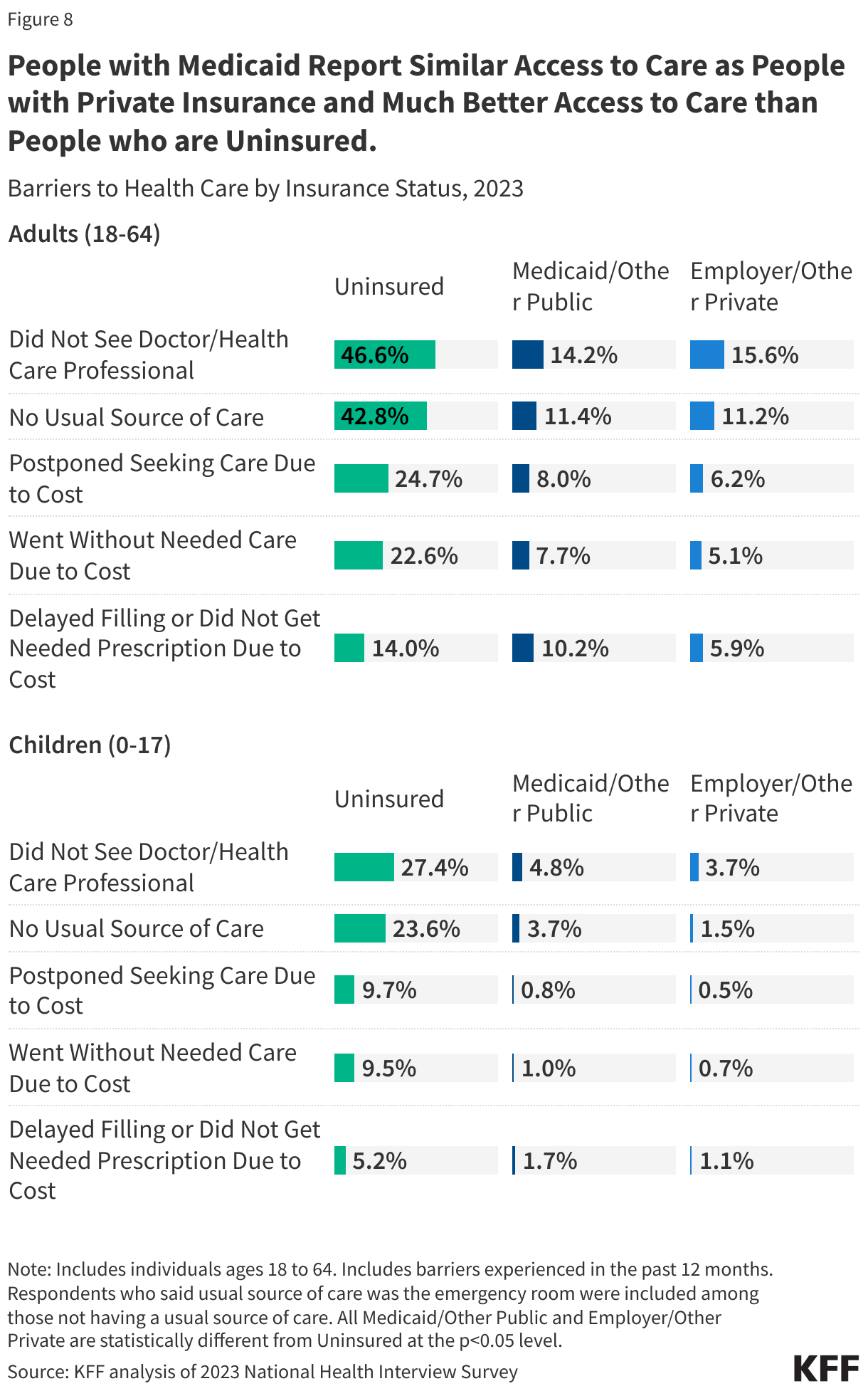
8. Medicaid coverage facilitates access to care, improves health outcomes, and provides financial protection from medical debt.
A large body of research shows that Medicaid beneficiaries have substantially better access to care than people who are uninsured (who are also primarily low-income) and are less likely to postpone or go without needed care due to cost, as federal rules generally limit out of pocket Medicaid costs. Key measures of access to care among Medicaid enrollees are generally comparable to rates for people with private insurance (Figure 8). Gaps in access to certain providers (e.g., psychiatrists and dentists) is an ongoing challenge in Medicaid that may reflect system-wide problems, but may be exacerbated by provider shortages in low-income communities, Medicaid’s lower physician payment rates, and lower Medicaid physician participation compared with private insurance.
Longstanding research shows that Medicaid eligibility during childhood is associated with positive effects on health (including reduced avoidable hospitalizations and mortality) and impacts beyond health, such as improved long-run educational attainment. Early and updated research findings show that state Medicaid expansions to low-income adults are associated with increased access to care, increased economic security, improved self-reported health status, and other outcomes including increased early-stage cancer diagnosis rates, lower mortality rates for certain conditions (e.g., cancer, cardiovascular disease, liver disease), decreased maternal mortality, improved treatment management for conditions (e.g., diabetes, HIV), and improved outcomes related to substance use disorders. Research conducted by NBER (National Bureau of Economic Research) suggests that the ACA Medicaid expansion had impacts beyond health care use, including on consumer financial outcomes – reducing unpaid bills and medical debt sent to collections.
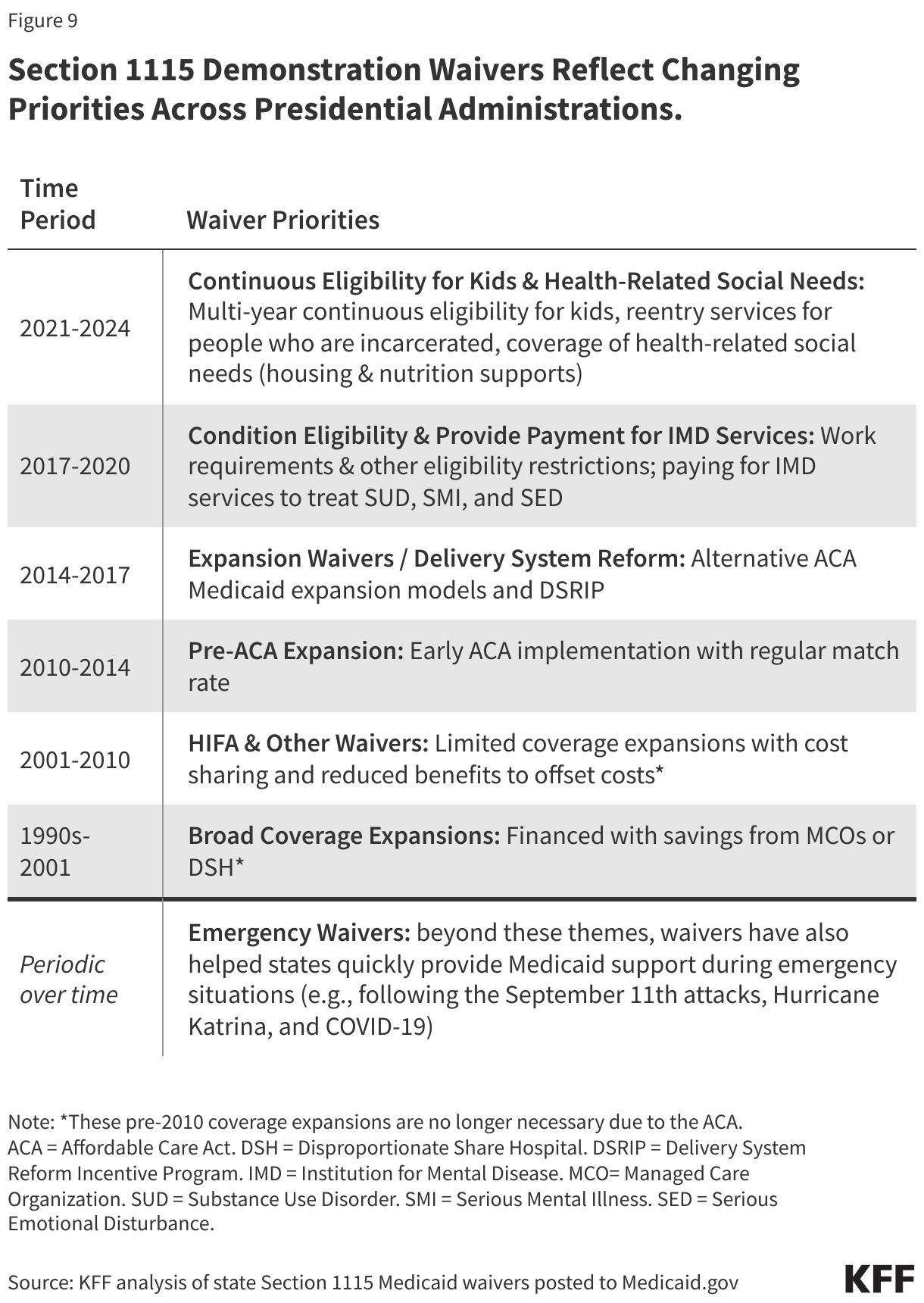
9. Section 1115 demonstration waivers reflect changing priorities across presidential administrations.
Section 1115 demonstration waivers offer states an avenue to test new approaches in Medicaid that differ from what is required by federal statute, if [in the HHS Secretary’s view] the approach is likely to “promote the objectives of the Medicaid program.” Waivers generally reflect priorities identified by states as well as changing priorities from one presidential administration to another (Figure 9). Waivers have been used to expand coverage or benefits, change policies for existing Medicaid populations (e.g., testing premiums or other eligibility requirements), modify delivery systems, restructure financing or authorize new payments (e.g., supplemental payments or incentive-based payments), as well as make other program changes. Waivers vary in size and scope. States can obtain “comprehensive” Section 1115 waivers that make broad program changes or narrow waivers focused on a specific population. Nearly all states have at least one active Section 1115 waiver and some states have multiple 1115 waivers.
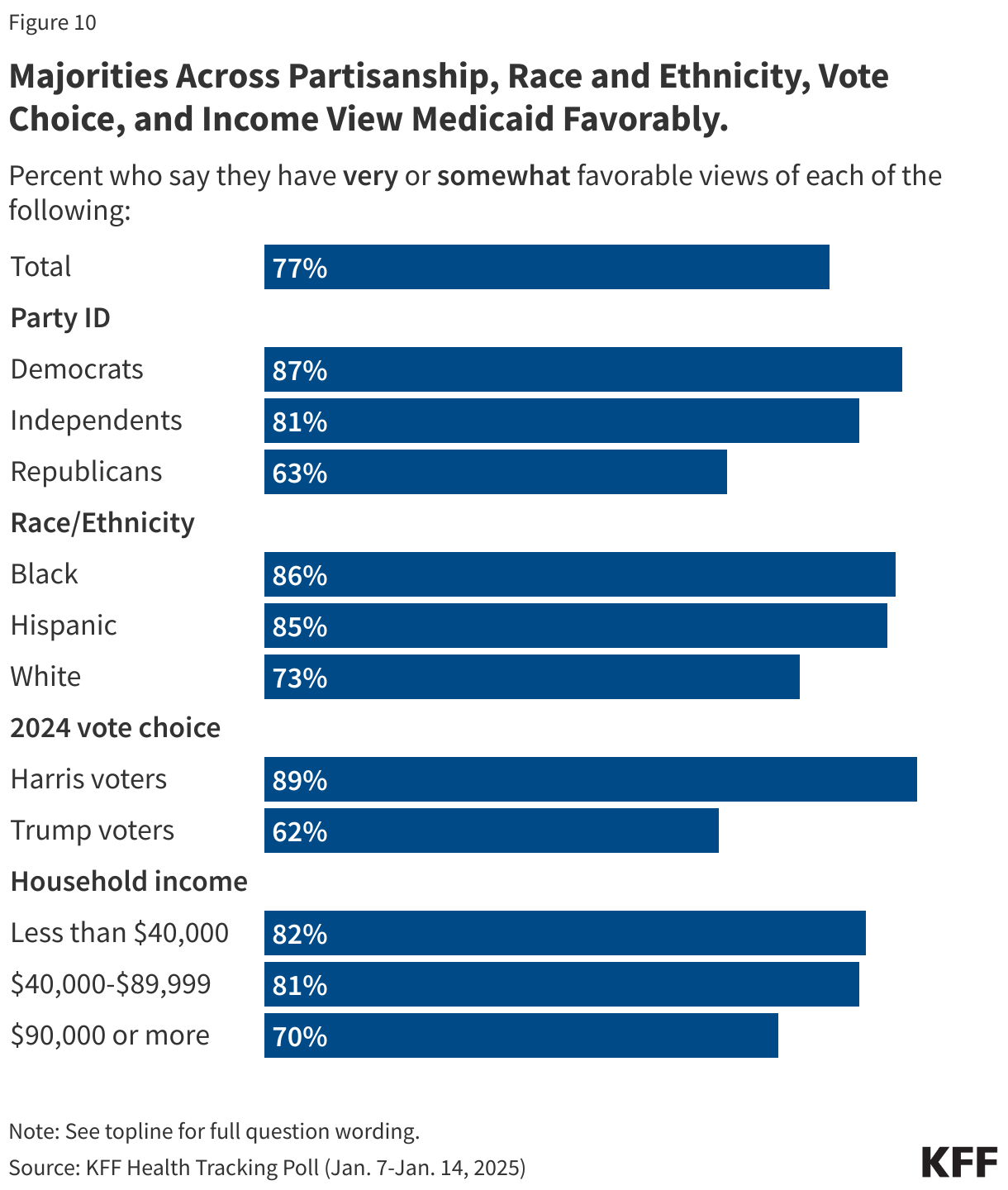
10. The majority of the public holds favorable views of Medicaid.
In the most recent KFF tracking poll, more than three-fourths (77%) of Americans held favorable views of Medicaid, including six in ten Republicans (63%), and at least eight in ten independents (81%) and Democrats (87%) (Figure 10). Medicaid is also viewed favorably by a majority of voters who say they voted for President Trump in the 2024 election (62%). Nearly half of the public (46%) say the federal government doesn’t spend enough on the Medicaid program, with another third (33%) saying it spends “about the right amount,” and around one in five (19%) saying it spends “too much.” With possible changes to government health programs, seven in ten (72%) say they are worried about the level of benefits that will be available to people covered by Medicaid in the future