Medicare Advantage Enrollees Account for a Rising Share of Inpatient Hospital Days
Enrollment in Medicare Advantage has grown rapidly in recent years, with more than half of all eligible Medicare beneficiaries now receiving their Medicare coverage from a private plan. The rise in Medicare Advantage enrollment has implications for beneficiaries and health care providers, including hospitals, because Medicare Advantage differs from traditional Medicare in many ways.
Unlike traditional Medicare, Medicare Advantage plans often require prior authorization before covering some services. Virtually all Medicare Advantage enrollees are in a plan that requires prior authorization for inpatient hospital stays (98%) and post-acute skilled nursing facility stays (99%). Prior authorization requirements are intended to reduce unnecessary care and lower costs, but also impose administrative burdens on health care providers, and could lead to delays and barriers to care.
Medicare Advantage plans typically establish networks of providers, including (or excluding) hospitals, and impose higher out-of-pocket costs for enrollees who obtain care from out-of-network providers. As enrollment in Medicare Advantage grows, decisions made by insurers about which hospitals to include in the network, and decisions made by hospitals about whether to be in a Medicare Advantage network, can be expected to affect a larger share of the Medicare population.
Recently, some hospitals, health systems, and medical groups have raised concerns about the impact of Medicare Advantage on their finances, with some terminating or threatening to terminate contracts with insurers over delays in payment, more restrictive coverage determinations, and payment rates. One issue that has recently drawn scrutiny from these groups has been Medicare Advantage plans’ practice of shifting hospitalized patients to “observation status,” which often means lower payments to hospitals and higher costs for patients.
This data note examines the growth of Medicare Advantage as a share of hospital inpatient days between 2015 and 2022 using data from hospital cost reports submitted to the Centers for Medicare and Medicaid Services (CMS). This analysis documents the share of hospital inpatient days attributable to Medicare Advantage across general short-term hospitals with full-year cost reports in a given year, excluding those that were missing data or in the U.S. territories.
Key Takeaways
- Medicare Advantage represents a growing share of total hospital inpatient days. Medicare Advantage grew from 13% to 23% of inpatient hospital days, and as of 2022, nearly half (48%) of all Medicare inpatient hospital days were attributable to Medicare Advantage enrollees.
- Three in ten hospitals had more inpatient days from Medicare Advantage enrollees than traditional Medicare enrollees in 2022. The share of hospitals with more Medicare Advantage than traditional Medicare inpatient days grew from 5% in 2015 to 30% in 2022.
- Medicare Advantage inpatient day shares have grown fastest at non-metropolitan hospitals. The share of inpatient hospital days attributable to Medicare Advantage enrollees more than doubled in non-metropolitan counties between 2015 and 2022.
- The share of inpatient hospital days for Medicare Advantage enrollees varied widely across counties in 2022. Medicare Advantage inpatient day shares were highest in counties with higher Medicare Advantage penetration, and lowest in those with lower Medicare Advantage penetration.
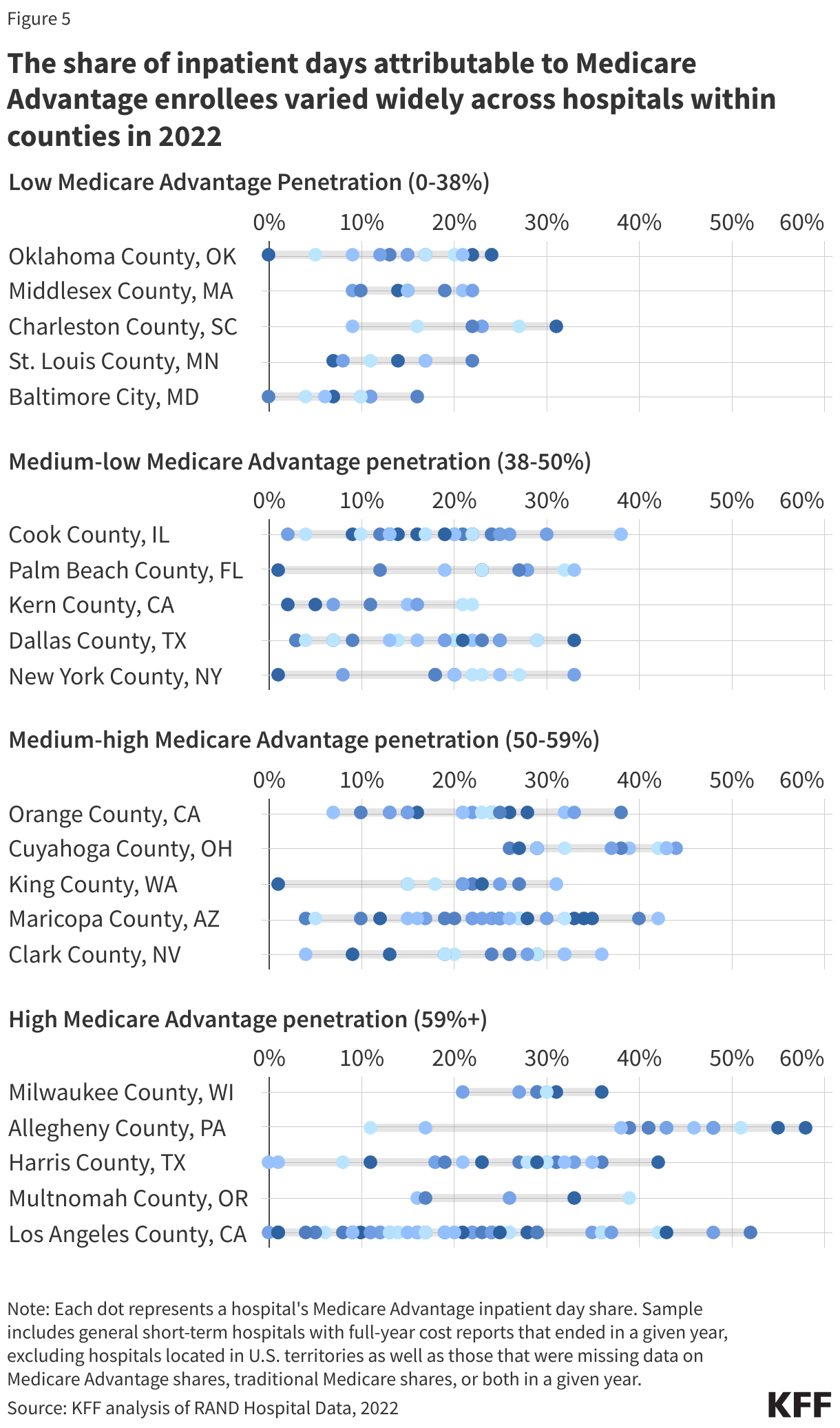
- Within counties, the share of inpatient days attributable to Medicare Advantage enrollees also varied widely across hospitals in 2022. For example, in Allegheny County, PA (a county with relatively high Medicare Advantage penetration), inpatient days attributable to Medicare Advantage enrollees ranged from 11% to 58% across hospitals. Similarly, there was large variation in counties with lower-than-average penetration, such as in Oklahoma County, Oklahoma, where the Medicare Advantage inpatient day share ranged from close to 0% to 24% across hospitals.
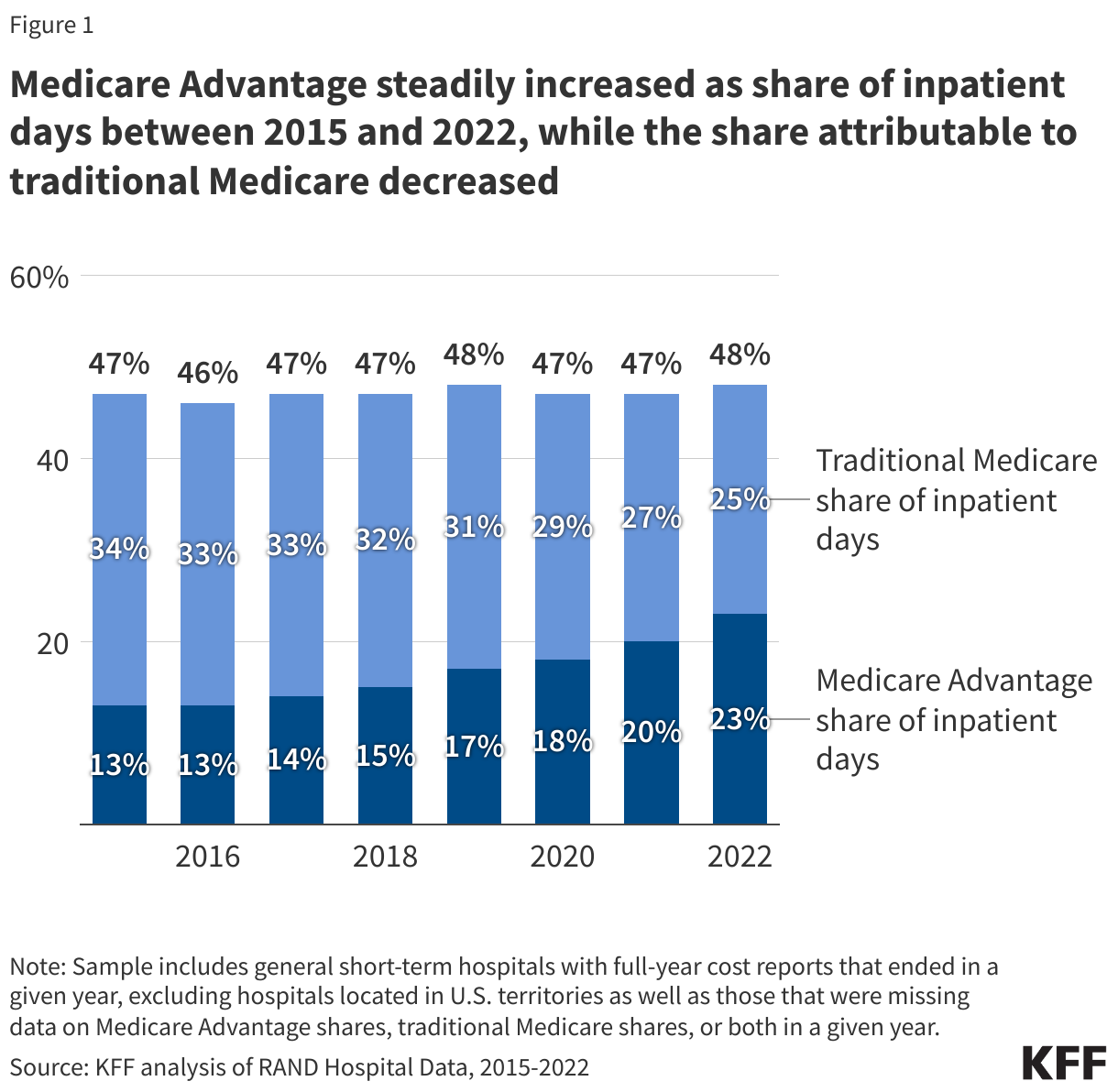
Medicare Advantage steadily increased as share of inpatient days between 2015 and 2022, while the share attributable to traditional Medicare decreased.
The share of total inpatient days attributed to Medicare Advantage enrollees grew from 13% in 2015 to 23% in 2022 among general short-term hospitals in the U.S (see Figure 1). During this same period, the share of inpatient days attributed to traditional Medicare declined from 34% to 25%. As of 2022, nearly half (48%) of all Medicare inpatient days were attributable to Medicare Advantage patients. The rise in the share of inpatient days attributable to Medicare Advantage enrollees coincided with an increase in Medicare Advantage enrollment as a share of all eligible Medicare beneficiaries from 32% in 2015 to 48% in 2022.
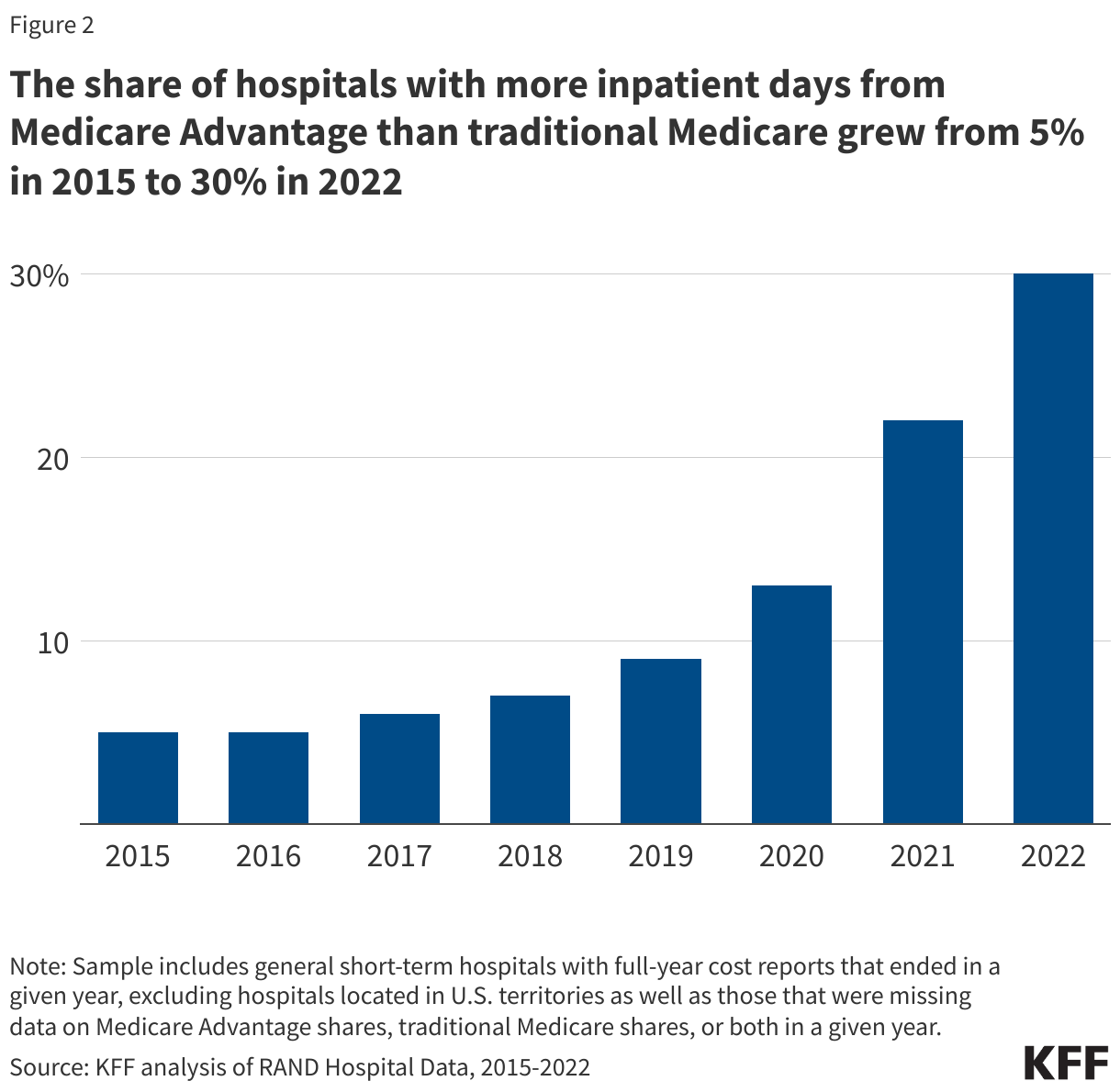
The share of hospitals with more inpatient days from Medicare Advantage than traditional Medicare increased from 5% in 2015 to 30% in 2022.
The increase in Medicare Advantage enrollment has contributed to a shift in patient mix across hospitals, affecting some more than others. The share of hospitals with more Medicare Advantage than traditional Medicare inpatient days increased from just 5% in 2015 to 30% in 2022 (Figure 2). Hospitals with a greater share of patients from Medicare Advantage than traditional Medicare may be more reliant on revenue from these plans, and more affected by various plan rules and decisions, such as prior authorization requirements, denials of claims, observation stay designations, and network restrictions.
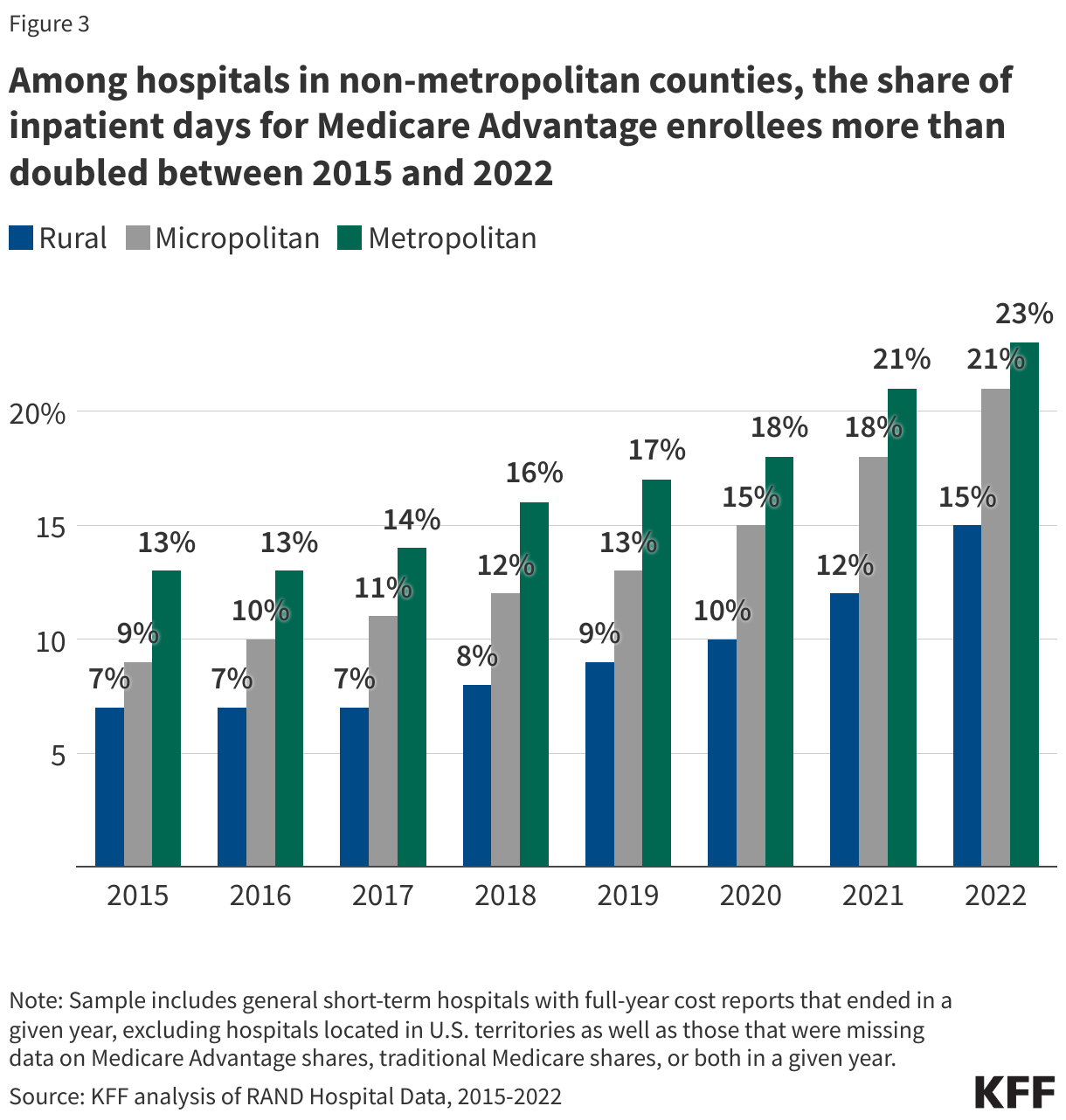
Among hospitals in non-metropolitan counties, the share of inpatient days for Medicare Advantage enrollees more than doubled between 2015 and 2022.
Across all rural hospitals, the share of inpatient days attributed to Medicare Advantage has been consistently lower than in metropolitan areas, but more than doubled over the study period, rising from 7% in 2015 to 15% in 2022 (Figure 3). The Medicare Advantage share of inpatient days also more than doubled in micropolitan areas, where it grew from 9% in 2015 to 21% in 2022. Enrollment in Medicare Advantage is lower in rural areas than in metropolitan or micropolitan areas, though it grew swiftly during this period, rising from 18% to 40% of eligible beneficiaries between 2015 and 2022. Some rural hospitals have raised concerns that negotiated rates paid by Medicare Advantage insurers are often lower than rates paid by traditional Medicare. As Medicare Advantage enrollment continues to climb, and as Medicare Advantage enrollees comprise a larger share of patients, rural hospitals may face new challenges.
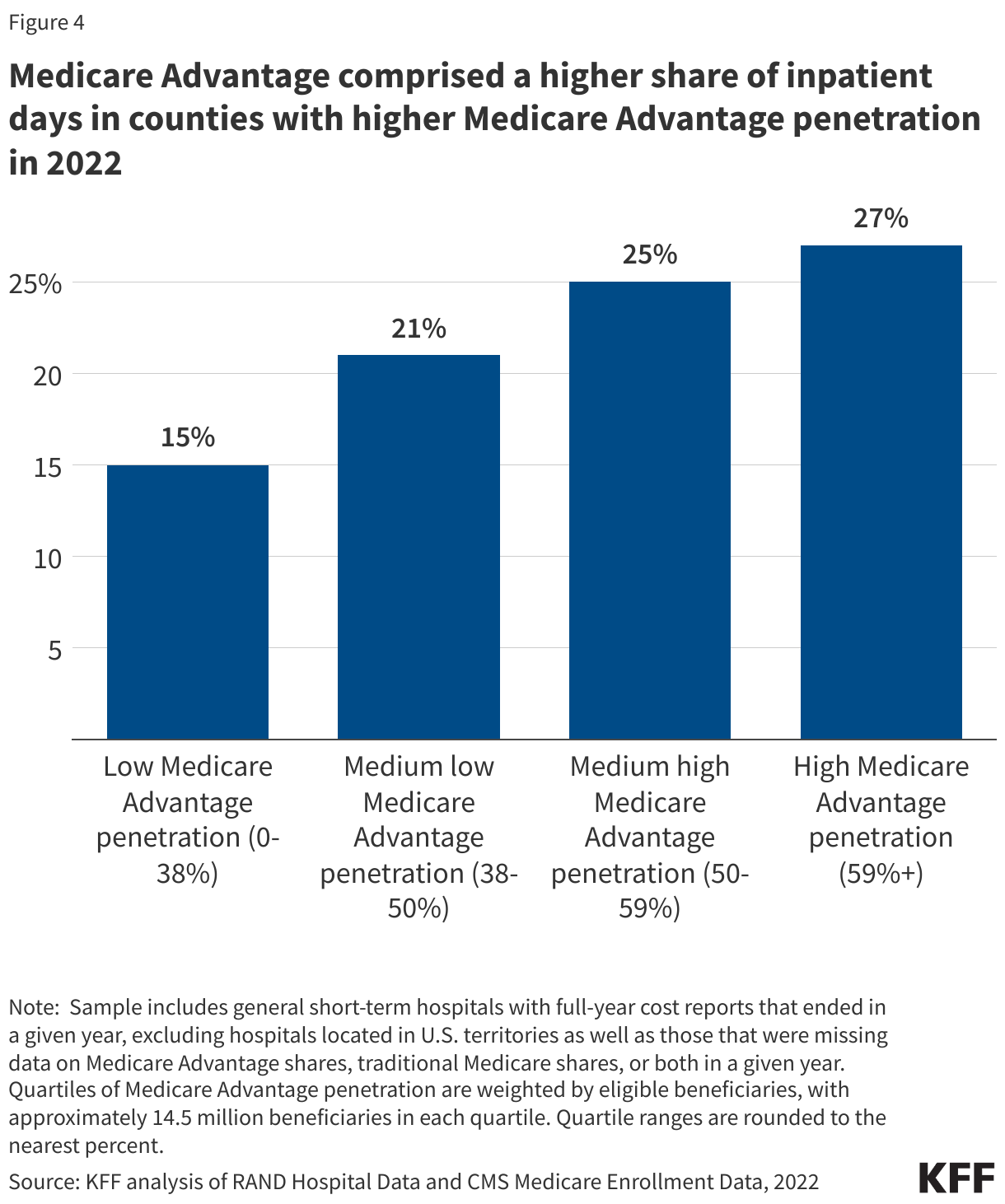
Medicare Advantage comprised a higher share of inpatient days in counties with higher Medicare Advantage penetration.
Across the country, the share of Medicare beneficiaries enrolled in Medicare Advantage varies widely. As might be expected, counties with higher Medicare Advantage penetration had larger Medicare Advantage shares of inpatient days than counties with lower Medicare Advantage penetration. Among counties in the top quartile of Medicare Advantage penetration, Medicare Advantage comprised 27% of inpatient days in 2022 (Figure 4), substantially greater than the 15% share among the bottom quartile of counties.
The share of inpatient days attributable to Medicare Advantage enrollees varied widely across hospitals within counties in 2022.
Although the share of inpatient days attributed to Medicare Advantage tracked county-level Medicare Advantage penetration, there was large variation within counties. The figure below illustrates the range in Medicare Advantage inpatient days as a share of total inpatient days for a set of counties that have several hospitals and are geographically dispersed in each quartile of Medicare Advantage penetration. For example, in Allegheny County, PA, a high penetration county, where 73% of eligible Medicare beneficiaries were enrolled in a Medicare Advantage plan in 2022, Medicare Advantage enrollees accounted for just 11% of all inpatient days in one hospital but more than half in others.
Even in relatively low penetration counties, there was substantial variation in the share of inpatient days attributed to Medicare Advantage. For instance, in Oklahoma County, Oklahoma, where 38% of beneficiaries were enrolled in a Medicare Advantage plan, the Medicare Advantage inpatient day share ranged from close to 0 to 24%.
Differences in Medicare Advantage inpatient day shares across hospitals within the same county may be due to a number of factors including whether a given hospital is included in Medicare Advantage networks, the extent to which a given hospital tends to serve people with Medicare based on the types of services and procedures it provides, and beneficiary preferences that might be based on convenience or perceived quality. As noted above, hospitals with a relatively large number of patients from Medicare Advantage may be more affected by prior authorization requirements, denials of claims, observation stay designations, and network restrictions of these plans. As Medicare Advantage enrollment continues to rise, the decisions made by Medicare Advantage plans related to reimbursement, coverage, and networks could have revenue implications for hospitals and other health care providers that can be expected to vary across counties and within local markets.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
This analysis draws on a number of data sources. Data on inpatient days and hospital characteristics came from RAND Hospital Data, which is a cleaned and processed version of annual cost report data that Medicare-certified hospitals are required to submit to the Healthcare Cost Report Information System (HCRIS). To our knowledge, the accuracy of reported traditional Medicare and Medicare Advantage days in hospital cost report data has not been evaluated. Hospitals report combined days for Medicare Advantage and cost plan enrollees. Cost plans account for a negligible share of Medicare enrollment, so we refer to the combination as “Medicare Advantage days” throughout. County-level Medicare Advantage penetration was calculated from Medicare enrollment data. Enrollment data is only provided for plan-county combinations that have at least 11 beneficiaries, and some counties do not have plans that meet this threshold. We assumed these counties had 0% Medicare Advantage penetration. Core Based Statistical Area (CBSA) classifications were used to designate hospitals as being in metropolitan or micropolitan counties. Metropolitan CBSAs contain at least one urban area with 50,000 or more inhabitants, and micropolitan CBSAs contain at least one urban area with at least 10,000 but fewer than 50,000 inhabitants. We classified counties not located in CBSAs as rural.
We restricted this analysis to general short-term hospitals and excluded hospitals in U.S territories. Cost reports reflect varying reporting periods that often do not align with a calendar year. We assigned cost reports to calendar years based on the year that the cost report ended in. We only examined cost reports that covered 365 or 366 days (referred to as “full-year cost reports”). These restrictions left 4,389 cost reports in 2022. Of these 4,389 cost reports, we analyzed 3,772 that were not excluded from the analysis due to missing Medicare Advantage or traditional Medicare inpatient days, or due to rare circumstances (2 cost reports in 2022) where combined Medicare Advantage and traditional Medicare inpatient days exceeded the total inpatient days reported by the hospital, suggesting inaccurate data.
Fourteen percent of the 4,389 cost reports described above were missing data for Medicare Advantage inpatient days in 2022 (compared to less than 1% for inpatient days overall and 1.3% for traditional Medicare days). The 14 percent of hospitals that were missing Medicare Advantage data were more likely to be small or rural and accounted for less than 2 percent of all inpatient days. None of the reports in our sample reported zero Medicare Advantage inpatient days. It is unclear whether and when missing values represent zero days. We suspect that Medicare Advantage may represent a relatively small share of inpatient days on average among hospitals with missing data, in part because hospitals with relatively few Medicare Advantage days have a smaller incentive to track and report these days when required for additional reimbursement under traditional Medicare (e.g., for medical education adjustments).
We conducted sensitivity analyses to explore the implications of missing Medicare Advantage data. First, we ran analyses excluding groups of hospitals that were most likely to be missing data, such as Critical Access Hospitals and hospitals with fewer than 25 beds. Second, we ran analyses that assumed that hospitals with missing data had zero Medicare Advantage inpatient days, which would be the lower bound of the possible Medicare Advantage shares at these hospitals. Third, we ran our analysis of overall and rural hospital Medicare Advantage share trends using hospitals that had Medicare Advantage data for all years (2015 through 2022). Different approaches increased or decreased average Medicare Advantage shares—e.g., with lower shares when replacing missing values with zeroes and higher shares when excluding small hospitals and Critical Access Hospitals—and especially so among rural hospitals. However, our main findings that there were large increases in Medicare Advantage as a share of inpatient days across hospitals in rural, micropolitan and metropolitan areas alike and that shares were higher in counties with greater Medicare Advantage penetration was true across all of our sensitivity analyses.