FAQs about the Inflation Reduction Act’s Medicare Drug Price Negotiation Program
This brief was updated in January 2025 to reflect details about the 15 drugs selected for the second year of the Medicare drug price negotiation program.
The Inflation Reduction Act of 2022 (the Act), signed into law by President Biden in August 2022, includes several provisions to lower prescription drug costs for people with Medicare and reduce drug spending by the federal government. One of the Act’s key drug-related provisions is a requirement for the Secretary of Health and Human Services (HHS) to negotiate prices with drug companies for certain drugs covered under Medicare Part D (starting in 2026) and Part B (starting in 2028). This requirement is the culmination of years of debate among lawmakers over whether to grant the federal government the authority to negotiate drug prices in Medicare, and is being implemented at the same time that several lawsuits have been filed seeking to thwart this effort.
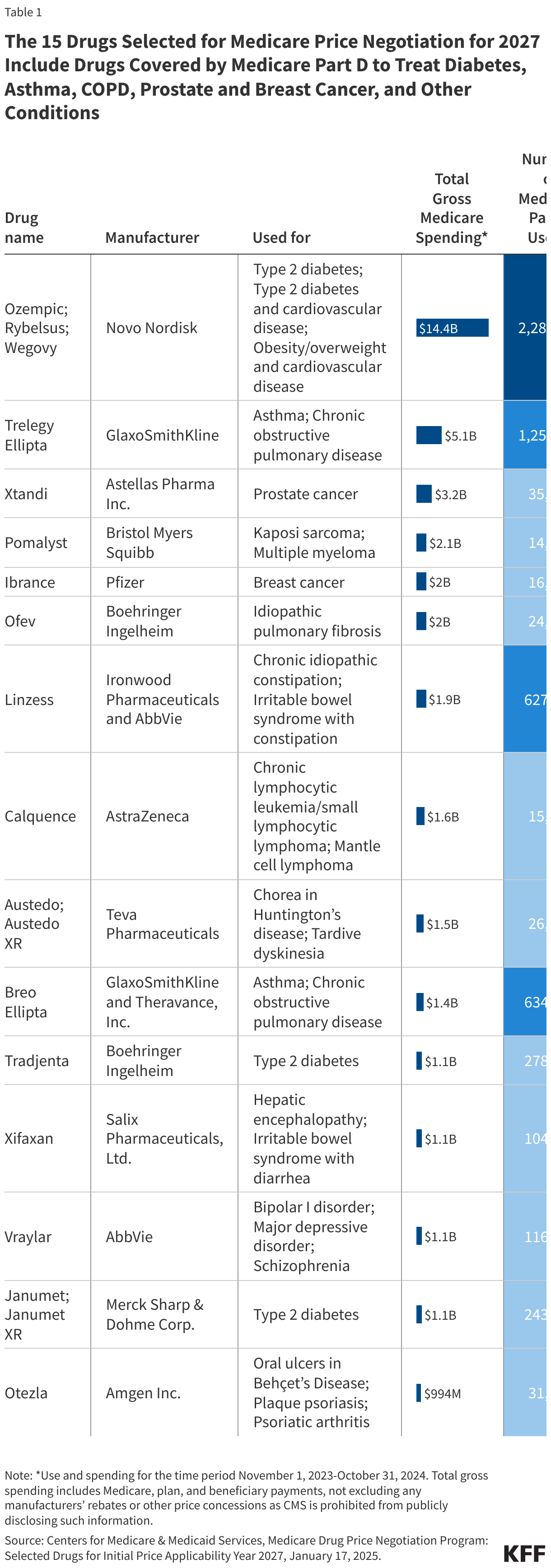
On January 17, 2025, the Centers for Medicare & Medicaid Services (CMS) announced the list of 15 Part D drugs selected for the second round of price negotiation, after concluding the first round of negotiation for 10 Part D drugs in August 2024. These 15 drugs include the popular diabetes and obesity drugs Ozempic and Wegovy, along with other drugs used to treat asthma and chronic obstructive pulmonary disease, type 2 diabetes, different types of cancer, and other medical conditions (see Table 1 below). Negotiated prices for these drugs will take effect on January 1, 2027.
Drawing on CMS’s guidance for the second year of the Medicare drug price negotiation program, issued by the Biden Administration in October 2024, and the Act’s statutory language, these FAQs address several questions related to the negotiation program and CMS’s plans for implementation, with a focus on the details that apply for 2027. (For the next cycle of negotiation that will include both Part D and Part B drugs selected for 2028, CMS under the Trump administration would need to issue updated guidance.)
- How many and which types of drugs qualified for price negotiation for 2027?
- How did CMS identify the drugs selected for price negotiation for 2027?
- What is the timeline for key activities under the Medicare drug price negotiation program for 2027?
- How will CMS determine if a generic or biosimilar is available and being marketed?
- What is the Small Biotech Exception?
- What is the Biosimilar Delay?
- What factors does CMS use in negotiating the maximum fair price for a given selected drug?
- Who is eligible to receive the maximum fair price?
- Is there a ceiling on the maximum fair price? Does it vary depending on the type of drug?
- How will CMS determine its initial offer for the maximum fair price for a selected drug?
- What are the steps in the negotiation process between CMS and manufacturers of selected drugs?
- What happens if a generic or biosimilar drug becomes available after a drug has been selected for negotiation?
- Are there limitations on administrative or judicial review of various features of the drug price negotiation program?
- How will people with Medicare benefit from the drug price negotiation program?
- What was the outcome of the first round of negotiation for 2026?
- What is public opinion related to the drug price negotiation program?
- What is the status of lawsuits challenging the drug price negotiation program?
In general, implementation of the program for the second round of negotiation will be largely similar to the first round, but with additional opportunities for public input through more patient-focused roundtable discussions and more opportunities for the exchange of offer prices between CMS and manufacturers during the negotiation process. In its updated guidance, CMS also provided substantially more details about the “Medicare Transaction Facilitator” that will enable manufacturers to pass through the maximum fair price to dispensers of selected drugs for eligible individuals. While it is unclear what direction the Trump administration might take with respect to the negotiation program, it is possible that the approach to implementation in 2025 and beyond may differ from that which was laid out in CMS’s most recent guidance.
How many and which types of drugs qualified for price negotiation for 2027?
For 2027, 15 Medicare Part D drugs have been selected for price negotiation (Table 1). These 15 drugs include the popular diabetes and obesity drugs Ozempic and Wegovy, along with other drugs used to treat asthma and chronic obstructive pulmonary disease, type 2 diabetes, prostate and breast cancer, and other conditions. Total spending on these 15 drugs between November 2023 and October 2024 was $40.7 billion, with 5.3 million Medicare beneficiaries using these medications during that time.
Drugs qualified for price negotiation for 2027 if they are covered under Medicare Part D, Medicare’s outpatient prescription drug benefit program, and are single source brand-name drugs or biological products without therapeutically-equivalent generic or biosimilar alternatives that are approved or licensed and marketed on a “bona fide” basis (see below). In addition, a drug product must be at least 7 years (for small-molecule drugs) or 11 years (for biologics) past its FDA approval or licensure date, as of the date that the list of drugs selected for negotiation is published. This means that for a single source drug to be eligible for negotiation for 2027, a drug product must have been approved on or before February 1, 2018, and a biological product must have been licensed on or before February 1, 2014. For drugs with multiple FDA approvals, CMS uses the earliest approval date to determine the number of years that have elapsed.
The definition of ‘qualifying single source drug’ excludes certain types of drugs: (1) drugs that are designated for only one rare disease or condition and approved for an indication (or indications) only for that disease or condition (known as the orphan drug exclusion); (2) drugs with total spending under Part D and Part B combined of less than $200 million, increased by the percentage increase in the consumer price index for all urban consumers (CPI-U) between June 1, 2023 to September 30, 2024 (based on drug spending data from November 1, 2023 to October 31, 2024 for the 2027 determination); and (3) plasma-derived products. For 2026 to 2028, the Act also makes an exception for so-called “small biotech” drugs (explained in more detail below).
According to CMS, a drug that is designated for more than one rare disease or condition will not qualify for the orphan drug exclusion, even if it is not approved for any indications for those additional diseases or conditions. CMS will only consider active designations and approvals when making determinations about whether a drug qualifies for the orphan drug exclusion.
For 2028, up to 15 drugs covered under Medicare Part D or Part B will be selected for price negotiation, followed by up to 20 additional drugs covered under Part D or Part B drugs for 2029 and later years. The number of drugs with negotiated prices available will accumulate over time.
How did CMS identify the drugs selected for price negotiation for 2027?
The 15 Part D drugs that were selected for price negotiation for 2027 were chosen from the top 50 negotiation-eligible Part D drugs with the highest total Medicare Part D expenditures. For this purpose, total expenditures are defined as total gross covered prescription drug costs. To determine this ranking, CMS first identified the qualifying single source drugs among all covered Part D drugs, applying the relevant statutory exclusions (as described above). CMS then calculated total expenditures for each qualifying drug, based on spending data for the 12-month period from November 1, 2023 to October 31, 2024. The top 50 drugs with the highest total expenditures for this 12-month period were the negotiation-eligible drugs for 2027.
The Inflation Reduction Act provides for a delay in selecting drugs for negotiation if they are biological products where there is a “high likelihood” of biosimilar market entry within two years of the publication date of the selected drug list (see details below). CMS announced that for 2027, when selecting the 15 highest-ranked Part D drugs from this top 50 list, no products qualified for delayed selection based on a high likelihood of biosimilar market entry before February 1, 2027.
What is the timeline for key activities under the Medicare drug price negotiation program for 2027?
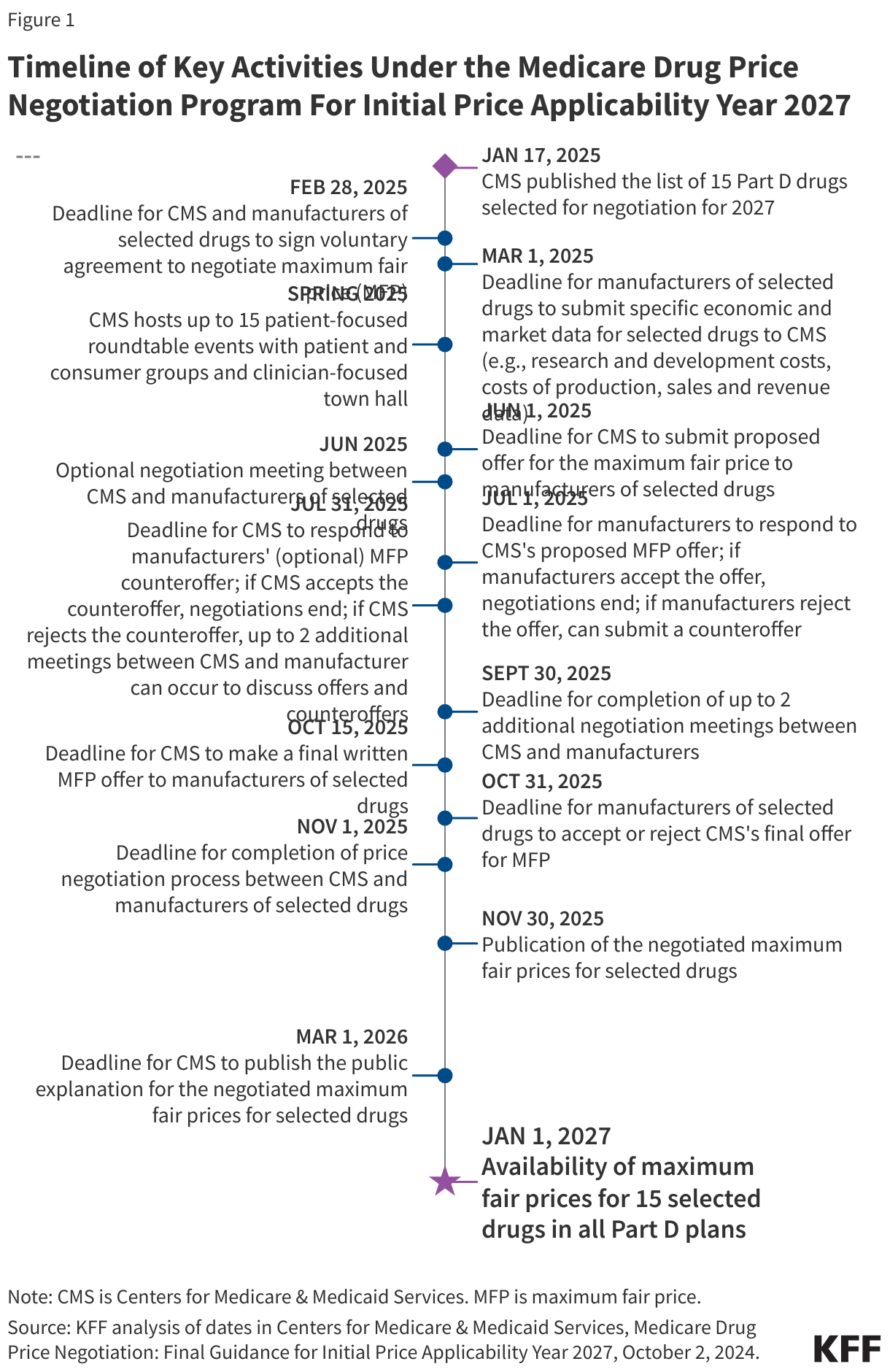
For the 15 Part D selected drugs with negotiated prices taking effect in 2027, Figure 1 provides a timeline of key dates and activities in the negotiation timeline.
How will CMS determine if a generic or biosimilar is available and being marketed?
The availability and “bona fide” marketing of a generic or biosimilar for any strength or dosage form of a drug product will eliminate that drug from consideration as a qualifying single source drug. In determining whether a potential qualifying single source drug may be disqualified based on the availability and bona fide marketing of a generic or biosimilar, CMS intends to draw on information from multiple sources.
CMS will use FDA reference sources to determine whether a generic or biosimilar has been approved. In determining whether generic or biosimilar equivalents were available and marketed on a bona fide basis for the potential qualifying single source drugs for 2027, CMS reviewed Part D claims data from the period of January 16, 2024 to January 15, 2025, and Average Manufacturer Price (AMP) data for December 1, 2023 to November 30, 2024 to assess utilization and sales of generics or biosimilars.
According to CMS guidance, the determination of marketing on a bona fide basis will not be based on a strict quantitative definition but on the “totality of circumstances,” which, in addition to utilization and sales data, could also include factors such as whether the generic or biosimilar is readily available for purchase and whether any agreements exist between manufacturers of the brand and generic drug that might limit availability of the drug. CMS will conduct ongoing assessments to determine whether “meaningful” competition exists and ensure marketing on a bona fide basis.
What is the Small Biotech Exception?
For 2026 through 2028, the Inflation Reduction Act specifies that “small biotech” drugs will not be eligible for negotiation. To qualify under this “Small Biotech Exception” for 2027, total expenditures under Part D on the drug in 2021 must be both 1% or less of total Part D expenditures for all covered Part D drugs, and 80% or more of total expenditures under Part D for all of the manufacturer’s drugs where a Coverage Gap Discount Program agreement was in effect in 2021. These calculations are made by CMS.
A manufacturer that seeks to have a drug considered for the Small Biotech Exception is required to submit information about the company and its products to CMS. For 2027, exception requests were due by December 10, 2024, and CMS determined that four drugs qualified for the Small Biotech Exception for the second round of negotiation.
Manufacturers who want to have a drug considered for this exception for 2028 will have to resubmit their request in the future, since CMS’s determinations about the Small Biotech Exception for 2026 and 2027 will not carry over to future years.
What is the Biosimilar Delay?
The Inflation Reduction Act provides for a delay in selecting drugs for negotiation if they are biological products where there is a “high likelihood” of biosimilar market entry within two years of the publication date of the selected drug list. For 2027, this means that licensure and marketing of a biosimilar must be highly likely to occur before February 1, 2027. The rationale for this delay is to not create financial incentives that could deter biosimilars from entering the market if, for example, a reference product (the original biological product approved by FDA against which a proposed biosimilar product is compared) is selected for negotiation and ultimately priced lower than potential competitor biosimilar products.
For CMS to consider whether to grant such a delay, the manufacturer of the biosimilar biological product for a given negotiation-eligible reference product will need to submit a delay request to CMS prior to the selected drug publication date. The biosimilar manufacturer must not be the same as the manufacturer of the reference product, and there must be no agreements between the two manufacturers that restrict the availability of the biosimilar in the U.S. A biosimilar manufacturer will not know if the reference product will be selected for negotiation when they submit this request, but CMS will disregard the request if the reference product does not end up being selected for negotiation. For 2027, the deadline for submissions from biosimilar manufacturers for delay requests, including the documentation required to support CMS’s consideration of the request, was December 10, 2024.
CMS will make a determination of whether there is a high likelihood of biosimilar market entry based on two factors: (1) whether an application for licensure of the biosimilar product has been accepted for review or already approved by the FDA (no later than January 15, 2025 for the 2027 negotiation year), and (2) “clear and convincing” evidence that the manufacturer will engage in bona fide marketing of the biosimilar product within two years of the selected drug publication date (by February 1, 2027 for the 2027 negotiation year), including demonstrating that there are no patent barriers to entry and operational readiness to bring the biosimilar product to market. CMS will not grant a request to delay selection of a reference product for negotiation if more than one year has passed between licensure of the biosimilar and its marketing. CMS announced that for 2027, none of the 15 selected drugs qualified for delayed selection based on a high likelihood of biosimilar market entry.
What factors does CMS use in negotiating the maximum fair price for a given selected drug?
The Inflation Reduction Act requires CMS to consider certain manufacturer-specific factors and information about therapeutic alternatives to selected drugs in negotiating the “maximum fair price” for selected drugs, although the Act does not specify how CMS should weigh these different elements in the process of developing its offer for the maximum fair price.
The manufacturer-specific factors related to selected drugs include:
- The manufacturer’s research and development costs and the extent to which the manufacturer has recouped these costs.
- The current unit costs of production and distribution.
- Federal financial support for novel therapeutic discovery and development related to the drug.
- Data on pending and approved patent applications, exclusivities, and certain other applications and approvals.
- Market data and revenue and sales volume data in the U.S.
For the manufacturers of the 15 Part D selected drugs for 2027, these data elements are required to be reported to CMS by March 1, 2025.
Information about therapeutic alternatives includes:
- The extent to which the selected drug represents a therapeutic advance compared to existing therapeutic alternatives and the costs of these alternatives.
- Prescribing information for the selected drug and its therapeutic alternatives, which may include generics or biosimilars.
- Comparative effectiveness of the selected drug and its therapeutic alternatives, taking into account their effects on specific populations, such as individuals with disabilities, the elderly, the terminally ill, children, and other patient populations.
- The extent to which the selected drug and its therapeutic alternatives address unmet needs for a condition that is not adequately addressed by available therapy.
According to CMS guidance, information on these factors may be submitted by several entities, including the manufacturer of the selected drug, other drug manufacturers, people with Medicare, academic experts, clinicians, and others. Submissions are due by March 1, 2025 for the selected drugs for 2027. In addition to evaluating the information in these submissions, CMS will review the literature and real-world evidence, conduct internal analysis, and consult with experts regarding evidence of the clinical benefits of the selected drugs and their therapeutic alternatives.
The Act explicitly directs that the HHS Secretary “shall not use evidence from comparative clinical effectiveness research in a manner that treats extending the life of an elderly, disabled, or terminally ill individual as of lower value than extending the life of an individual who is younger, non-disabled, or not terminally ill.” In other words, the use of health outcomes evidence based on quality-adjusted life years (QALYs) in the process of negotiating a maximum fair price is not permitted.
Who is eligible to receive the maximum fair price?
For selected drugs covered under Part D that are dispensed directly to individuals by a retail or mail order pharmacy, Medicare beneficiaries who are enrolled in Part D stand-alone drug prescription plans or Medicare Advantage plans offering drug coverage are eligible to receive the maximum fair price. For selected drugs covered under Part B that are administered to individuals in provider settings, Medicare beneficiaries enrolled in Part B, including those in both traditional Medicare and Medicare Advantage plans, are eligible to receive the maximum fair price. (Part B drugs will not be selected for negotiation until 2028.)
According to CMS guidance, the maximum fair price for a Part D selected drug must be provided to an enrollee when they use their Part D coverage to obtain that drug, but not when other coverage or payment arrangements are used, including plans that receive the Retiree Drug Subsidy, discount cards, or cash purchases.
CMS will require manufacturers to either ensure in advance that dispensing entities pay no more than the maximum fair price when they obtain the selected drug or reimburse dispensing entities for the difference between the acquisition price and the lower maximum fair price. A key requirement is that manufacturers adhere to a 14-day prompt payment window to facilitate timely payment of refunds to dispensing entities. CMS will engage a “Medicare Transaction Facilitator” (MTF) to help with the exchange of claims data and other information between different entities in the prescription drug supply chain to enable manufacturers to pass through the maximum fair price to dispensers of selected drugs for eligible individuals. CMS has established detailed guidelines for manufacturers of selected drugs and dispensing entities to participate in the MTF data exchange process, as well as guidelines for manufacturers who choose to use the MTF to pass through payments to dispensing entities.
CMS will require manufacturers of selected drugs to submit a plan for making the maximum fair price available in writing at least four months before the prices take effect (e.g., for the 2027 negotiation year, written plans are due no later than September 1, 2026). The plan shall include a description of how manufacturers will communicate with dispensing entities and, if the manufacturer chooses not to use the MTF for payment and reimbursement of dispensing entities, a description of the proposed alternative reimbursement mechanism. The Act establishes that manufacturers that do not ensure access to the maximum fair price for selected drugs to eligible individuals and dispensers may be subject to civil monetary penalties.
Is there a ceiling on the maximum fair price? Does it vary depending on the type of drug?
The Inflation Reduction Act establishes an upper limit for the maximum fair price for a given drug. The upper limit is the lower of the drug’s enrollment-weighted negotiated price (net of all price concessions, including rebates) for a Part D drug, the average sales price for a Part B drug (which is the average price to all non-federal purchasers in the U.S., inclusive of rebates, other than rebates paid under the Medicaid program), or a percentage of a drug’s average non-federal average manufacturer price (non-FAMP) (which is the average price wholesalers pay manufacturers for drugs distributed to non-federal purchasers). This percentage of non-FAMP varies depending on the number of years that have elapsed since FDA approval or licensure: 75% for small-molecule drugs and vaccines more than 9 years but less than 12 years beyond approval; 65% for drugs between 12 and 16 years beyond approval or licensure; and 40% for drugs more than 16 years beyond approval or licensure. This approach means that the longer a drug has been on the market, the lower the ceiling on the maximum fair price.
How will CMS determine its initial offer for the maximum fair price for a selected drug?
To determine its initial offer for a maximum fair price for a selected drug, CMS will: (1) identify therapeutic alternative(s) for the selected drug; (2) determine pricing information about the therapeutic alternatives to determine the starting point for the initial offer; (3) adjust the initial offer based on information about the clinical benefit of the selected drug compared to its therapeutic alternatives; and (4) make further adjustments to the offer price as needed based on manufacturer-specific data to determine the initial offer price.
According to the guidance, CMS will use the price of therapeutic alternative(s) as the starting point for determining the initial offer for the maximum fair price for a given selected drug. Specifically, for the 2027 negotiation year, CMS will use the lower of: the net Part D plan payment and beneficiary liability, which excludes both rebates as well as payments made by manufacturers in the coverage gap discount program, or the maximum fair price negotiated for 2026 selected drugs if any are therapeutic alternatives for 2027 selected drugs. If there is more than one therapeutic alternative for a selected drug, CMS will determine the starting point within the range of prices (whether net plan payment and beneficiary liability or maximum fair prices for those products).
For selected drugs with no therapeutic alternative or where the price of the alternative(s) is above the ceiling price, CMS will use the Federal Supply Schedule (FSS) or “Big Four Agency” price as the starting point, whichever is lower. (Drug prices listed on the FSS, which establishes prices available to all direct federal purchasers, are determined through both statutory rules and negotiation. A statutory cap on drug prices for the Big Four agencies—the Department of Veterans Affairs, the Department of Defense, the Public Health Service, and the Coast Guard—means the prices they pay are generally lower than prices paid by other direct federal purchasers.) If the FSS or Big Four prices are above the statutory ceiling, CMS will use the statutory ceiling as the starting point for its initial offer.
CMS will adjust the starting point for the initial offer based on a broad evaluation of evidence, including that which is submitted by manufacturers and the public, about the clinical benefit the selected drug provides relative to its therapeutic alternatives, including information about potential safety concerns and side effects, whether the selected drug represents a therapeutic advance as measured by improvements in clinical outcomes, and information about the effects of the selected drug and its therapeutic alternatives on specific populations, including people with disabilities and older adults. CMS will also consider comparative effectiveness data on patient-centered outcomes and patient experiences.
If a selected drug has no therapeutic alternatives, CMS will evaluate evidence about the drug’s clinical benefit, including outcomes and effect on specific populations, and also will consider the extent to which the selected drug fills an unmet medical need, meaning the drug treats a disease or condition where there are very limited or no other treatment options, or the existing treatments do not adequately address the disease or condition. This consideration will be made separately for each indication of a selected drug, where applicable.
After considering information about clinical benefit, CMS will adjust its starting point for the initial offer price to arrive at a “preliminary price.” After determining the preliminary price, CMS will take into account manufacturer-specific data elements. These data, and their illustrative effect on the preliminary price as described in the revised guidance, are:
- Research and development (R&D) costs: if a manufacturer has recouped its R&D costs, CMS could adjust the preliminary price downward, or upward if such costs have not been recouped.
- Current unit costs of production and distribution: if lower than the preliminary price, CMS could adjust the price downward, or upward if such costs are higher than the preliminary price.
- Prior federal financial support: if discovery and development of the selected drug was supported by federal funding, CMS could adjust the preliminary price downward.
- Patent information: this data will support CMS’s evaluation of whether a selected drug represents a therapeutic advance or meets an unmet medical need, particularly in light of any exclusivities which mean that a selected drug is the only available therapy.
- Market data and revenue and sales volume data for the drug in the U.S.: depending on how CMS’s preliminary price compares to other market pricing data for the selected drug, CMS could, for example, revise downward the preliminary price if the average commercial net price is lower, or upward if the average commercial net price is higher.
After making any necessary adjustments to the preliminary price based on a review of manufacturer-specific data, CMS will arrive at its initial offer for the maximum fair price.
What are the steps in the negotiation process between CMS and manufacturers of selected drugs?
CMS’s guidance outlines several steps in the negotiation process (Figure 1). These steps, and the relevant dates for selected drugs for 2027, are:
- CMS and manufacturers of selected drugs enter into a written agreement to negotiate to determine the maximum fair price for selected drugs by February 28, 2025.
- Submission of economic and market data from manufacturers of selected drugs to CMS and information about therapeutic alternatives is due on March 1, 2025.
- CMS will host one meeting with manufacturers of selected drugs in Spring 2025 after the submission of manufacturer-specific data elements so that manufacturers can provide additional context for their data submission and share new information, if applicable.
- CMS will host up to 15 patient-focused roundtable events with consumer and patient organizations (with selected drugs aggregated by condition, as appropriate) and one clinician-focused town hall event in Spring 2025 to solicit patient-focused and clinical information on therapeutic alternatives and other information for CMS to consider in developing its initial offer for selected drugs.
- CMS will make a written offer to the manufacturer of a selected drug with its initial offer of the maximum fair price by June 1, 2025. This written offer will include a justification for CMS’s initial offer based on the methodology used, including how CMS evaluated various data submitted by manufacturers and evidence about alternative therapies.
- An optional negotiation meeting between CMS and manufacturers of selected drugs could take place between the date of CMS’s initial offer and the deadline for manufacturers to respond.
- Manufacturers respond to CMS’s initial offer in writing either accepting the offer or making a counteroffer within 30 days of receiving the initial offer (e.g., July 1, 2025, for initial offers made by CMS on June 1, 2025). The written counteroffer should include the manufacturer’s proposed maximum fair price, along with a justification for that amount and a response to CMS’s justification for its initial offer. If the manufacturer does not accept CMS’s initial offer, a written counteroffer must be submitted, If the manufacturer accepts CMS’s initial offer, the negotiation process ends.
- CMS will provide a written response to the manufacturer in response to an optional written counteroffer, either accepting or rejecting the counteroffer, within 30 days (e.g., July 31, 2025, if the manufacturer’s counteroffer is made on July 1, 2025). If CMS accepts the manufacturer’s counteroffer, the negotiation process ends.
- If CMS rejects the manufacturer’s counteroffer, up to 2 additional in-person or virtual meetings could occur between CMS and the manufacturer to discuss offers and counteroffers. The meetings would focus on manufacturer-submitted data and information about therapeutic alternatives, and how that information should factor into the maximum fair price. The timeframe for negotiation meetings would end no later than September 30, 2025. Additional written offers and counteroffers could be exchanged after CMS’s rejection of the manufacturer’s counteroffer and final agreement on the maximum fair price (up to one week prior to CMS submitting a final written offer).
- After any negotiation meetings between CMS and the manufacturer, CMS makes a final written offer for the maximum fair price (no later than October 15, 2025 for the 2027 negotiation cycle).
- Manufacturers consider CMS’s final offer and either accept or reject the offer in writing (by October 31, 2025 for the 2027 negotiation cycle).
- The negotiation process ends when CMS and manufacturers of selected drugs reach agreement on the maximum fair price, but no later than the statutorily defined deadline for the negotiation process (November 1, 2025 for the 2027 negotiation cycle).
If an agreement on the maximum fair price is not reached by the deadline for the negotiation process, manufacturers may be subject to an excise tax, which is being administered by the IRS, as specified in the Inflation Reduction Act. CMS has outlined an expedited process manufacturers can follow if they choose to not participate in the negotiation program, which would enable them to withdraw their drugs from coverage under Medicare and Medicaid to avoid paying the excise tax.
According to CMS, manufacturers may disclose information related to the negotiation process with CMS if they choose to do so. CMS will not publicly discuss the specifics of the negotiation process related to any manufacturer but reserves the right to do so if manufacturers themselves choose to disclose this information.
What happens if a generic or biosimilar drug becomes available after a drug has been selected for negotiation?
Drugs are not eligible to be selected for negotiation if there is a generic or biosimilar using that drug as the reference product approved or licensed by the FDA and being marketed. (Authorized generics do not count for this purpose, since they are not technically generic drugs as that term is commonly used, but rather the same drug product as the brand-name drug with a different label.) If a drug has already been selected for negotiation and CMS determines that a generic or biosimilar drug has been approved or licensed and is being “bona fide” marketed (as described above) – either before or during the negotiation process – the negotiation process will not start or will be suspended. The drug will continue to be a selected drug (not replaced by another drug), but no maximum fair price will be negotiated. To be removed from the list of selected drugs for 2027, CMS will need to make this determination between February 1, 2025 and November 1, 2025 (between the selected drug publication date and the end of the negotiation process.)
If CMS determines that a generic or biosimilar drug has been approved and marketed after a drug has been selected for negotiation and after a maximum fair price has been established, the maximum fair price will take effect, but depending on when the determination is made, that drug will no longer be a selected drug and the maximum fair price will not apply in subsequent years. For selected drugs for 2027, if the determination of generic drug availability is made between November 2, 2025 and March 31, 2027, the maximum fair price will only apply in 2027 and the drug will no longer be a selected drug for 2028; if the determination is made between April 1, 2027 and March 31, 2028, the maximum fair price will apply in 2027 and 2028 and the drug will no longer be a selected drug for 2029.
Are there limitations on administrative or judicial review of various features of the drug price negotiation program?
The Act specifies several features of the drug price negotiation program that are not subject to administrative and judicial review, including:
- The determination of whether a drug is a qualifying single source drug
- The determination of whether a drug is a negotiation-eligible drug
- The selection of drugs for negotiation
- The determination of the maximum fair price for a selected drug
- The determination of whether a drug is subject to renegotiation
- The determination of units of a drug or biological product for the purposes (where unit is defined as the lowest amount of the product that is dispensed)
- The determination of whether a drug qualifies for the biosimilar delay
How will people with Medicare benefit from the drug price negotiation program?
There is uncertainty about how many Medicare beneficiaries will see lower out-of-pocket drug costs in any given year under the drug price negotiation program and the magnitude of potential savings, since both will depend on which drugs are subject to the negotiation process and the price reductions achieved through the negotiation process relative to what prices would otherwise be. For the 15 drugs selected for the second round of price negotiation, a total of 5.3 million Medicare beneficiaries used these medications between November 2023 and October 2024, ranging from a high of 2.2 million who used Ozempic, Wegovy, and Rybelsus down to 14,000 for the anti-cancer drug Pomalyst.
In addition, whether Part D enrollees pay lower out-of-pocket costs for a given Part D selected drug will depend in part on whether they pay flat copayment amounts or a coinsurance rate for the drug in their chosen Part D plan. If they pay coinsurance, they could see savings, assuming the negotiated maximum fair price is lower than their plan’s negotiated price.
Aside from the potential for out-of-pocket cost savings, the drug price negotiation program could improve Medicare Part D enrollees’ access to Part D drugs that are selected for negotiation, since Part D plans are required to cover all selected drugs with negotiated maximum fair prices, including all dosage forms and strengths. In the absence of this coverage requirement, it is possible that not all selected drugs, or all forms of the drugs, would be covered on all Part D plan formularies. Under current law, Part D plans generally can choose which drugs to cover and not cover on their formularies, subject to CMS’s formulary guidelines and requirements, except for drugs in six called “protected classes,” where all or substantially all drugs must be covered. CMS will use the annual formulary review process to ensure that all Part D plans cover all dosages and formulations of selected drugs. CMS will also review whether Part D plan sponsors place selected drugs on non-preferred tiers; place selected drugs on a higher tier than non-selected drugs in the same class; require utilization of an alternative brand prior to a selected drug; or impose more restrictive utilization management tools on a selected drug relative to a non-selected drug in the same class. In any such instances, CMS expects Part D plan sponsors to provide a clinical justification for these practices and will only approve those formularies that adhere to all statutory and regulatory guidelines and requirements.
What was the outcome of the first round of price negotiation for 2026?
On August 15, 2024, CMS announced negotiated prices for the first 10 drugs that were selected for negotiation. The 10 drugs selected for the first round of negotiations include treatments for several medical conditions, including diabetes (Farxiga, Fiasp/NovoLog, Januvia, Jardiance), blood clots (Eliquis, Xarelto), heart failure (Entresto, Farxiga), psoriasis (Stelara, Enbrel), rheumatoid arthritis (Enbrel), Crohn’s disease (Stelara), and blood cancers (Imbruvica) (Table 2). These prices will take effect for Medicare beneficiaries on January 1, 2026.

According to CMS, Medicare would have saved $6 billion if the prices that CMS negotiated for these 10 drugs had been in effect in 2023, amounting to net savings of 22% on these medications. CMS has also estimated that Medicare beneficiaries will save $1.5 billion when these negotiated prices take effect in 2026.
CMS published written explanations of the negotiated prices for the first 10 selected Part D drugs in December 2024, explaining the factors that were considered in the negotiation process, including manufacturer-specific financial data about the selected drugs and evidence about the clinical benefits of selected drugs compared to alternative treatments.
What is public opinion related to the drug price negotiation program?
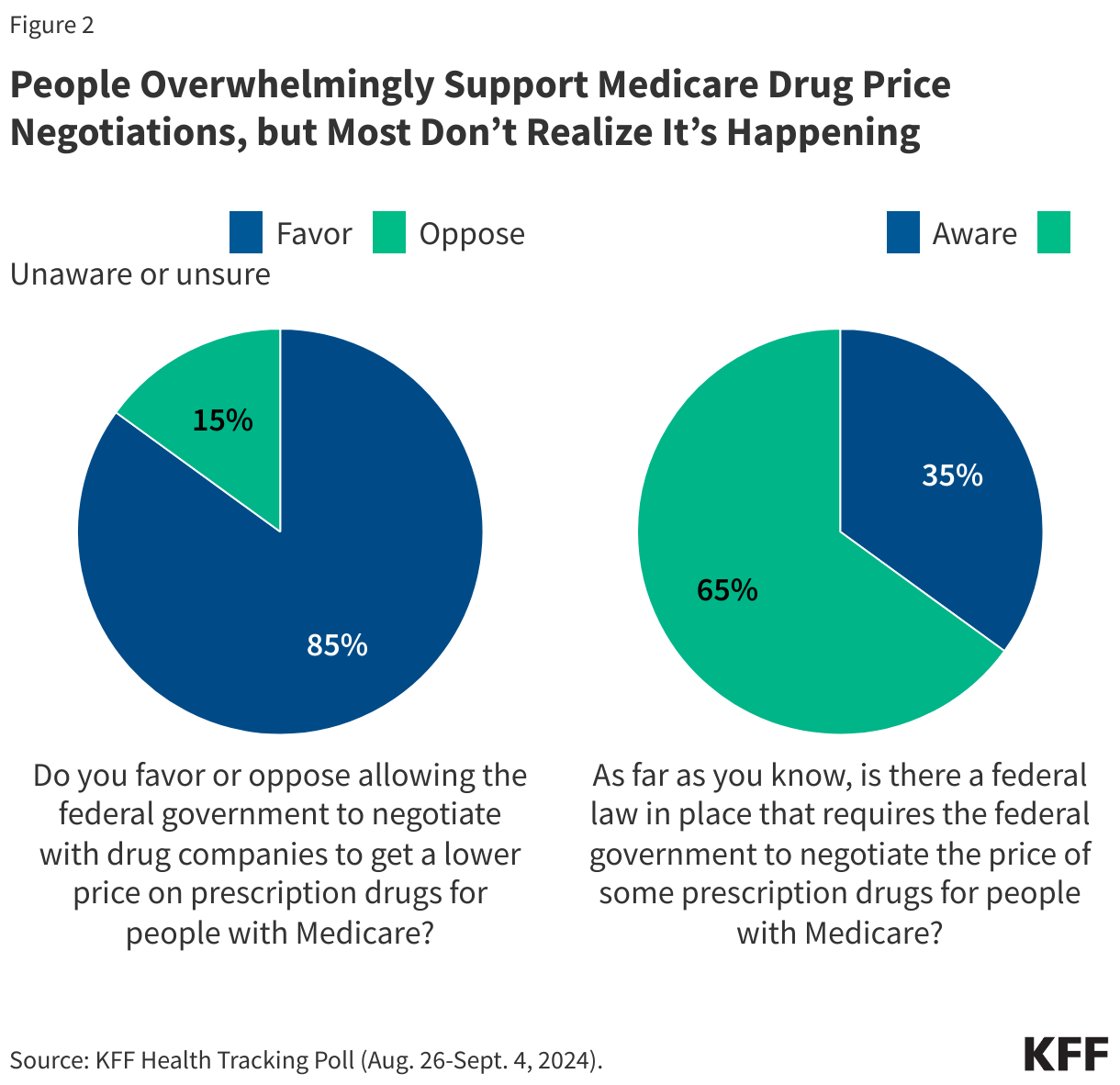
According to KFF Health Tracking polls, most adults favor allowing the federal government to negotiate drug prices with manufacturers to get a lower price on prescription drugs, and more than half of the public (55% overall, including 65% of Democrats, 54% of Independents, and 48% of Republicans) thinks that expanding the number of drugs subject to negotiation should be a top priority for Congress and the Trump administration.
More than 8 in 10 adults (85%) also favor allowing the government to negotiate lower prices with drug companies that would apply to both Medicare and private insurance (Figure 2). Even after hearing arguments for and against drug price negotiation by the federal government, a majority of adults continue to favor this approach. At the same time, KFF polling also shows that most adults are unaware that the law now requires the federal government to negotiate the price of some prescription drugs for people with Medicare. Just over one-third of voters overall (35%), and close to 4 in 10 (38%) voters ages 65 and older, say they are aware of this provision of the Inflation Reduction Act.
What is the status of lawsuits challenging the drug price negotiation program?
Since June 2023, several lawsuits have been filed challenging the drug price negotiation program by manufacturers of selected drugs and entities representing the pharmaceutical industry. These lawsuits – nine of which are ongoing, as of January 2025 – have raised similar constitutional and statutory challenges against the program. Among the constitutional challenges raised are the following:
- Drug manufacturers will be forced to give selected drugs to the government without fair compensation, in violation of the Fifth Amendment.
- Drug manufacturers are compelled to call this program a “negotiation” and say that final prices are “fair,” in violation of the corporations’ freedom of speech.
- The penalties levied on drug manufactures for not complying with the program and negotiation terms are so high they constitute “excessive fines,” which are banned by the Eight Amendment.
Other constitutional challenges include that the program violates the separation of powers doctrine and the Due Process Clause. In addition, plaintiffs are challenging the program on statutory grounds, such as the Administrative Procedures Act.
To date, none of these lawsuits have been decided in favor of industry plaintiffs. Most cases are either in the briefing stage or awaiting decisions before various U.S. appellate courts. In the event of conflicting rulings, an eventual hearing of one or more of these cases by the Supreme Court would be the likely outcome, but the timeframe for that is uncertain. It is not clear to what extent the federal government under the Trump administration will continue to defend the Medicare drug price negotiation program in court as these lawsuits move through the judicial system.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.