5 Key Facts About Medicaid Coverage for People with Medicare
The recently passed House budget resolution targets cuts to Medicaid of up to $880 billion or more over a decade to help pay for tax cuts. Major cuts to Medicaid may impact coverage for the almost 1 in 5 Medicare beneficiaries (12.2 million) who are also enrolled in Medicaid. For people covered under both programs (“dual-eligible individuals”), Medicare is the primary payer and covers medical acute and post-acute care, including skilled nursing facility services and home health care. Medicaid wraps around Medicare coverage by paying Medicare premiums and in most cases, cost sharing. Most dual-eligible individuals (8.9 million people in 2024) are “full-benefit” enrollees, which means they are eligible for Medicaid benefits that are not otherwise covered by Medicare, including long-term care, vision, and dental. The remaining 3.3 million dual-eligible individuals, “partial-benefit” enrollees, are eligible for Medicare premiums and often, cost sharing assistance, but not for full Medicaid benefits.
It is unclear what policies might be designed to achieve $880 billion in savings, but there are possible implications for Medicare beneficiaries, who account for nearly 30% of Medicaid spending. Effects would vary across states as coverage and benefits do.
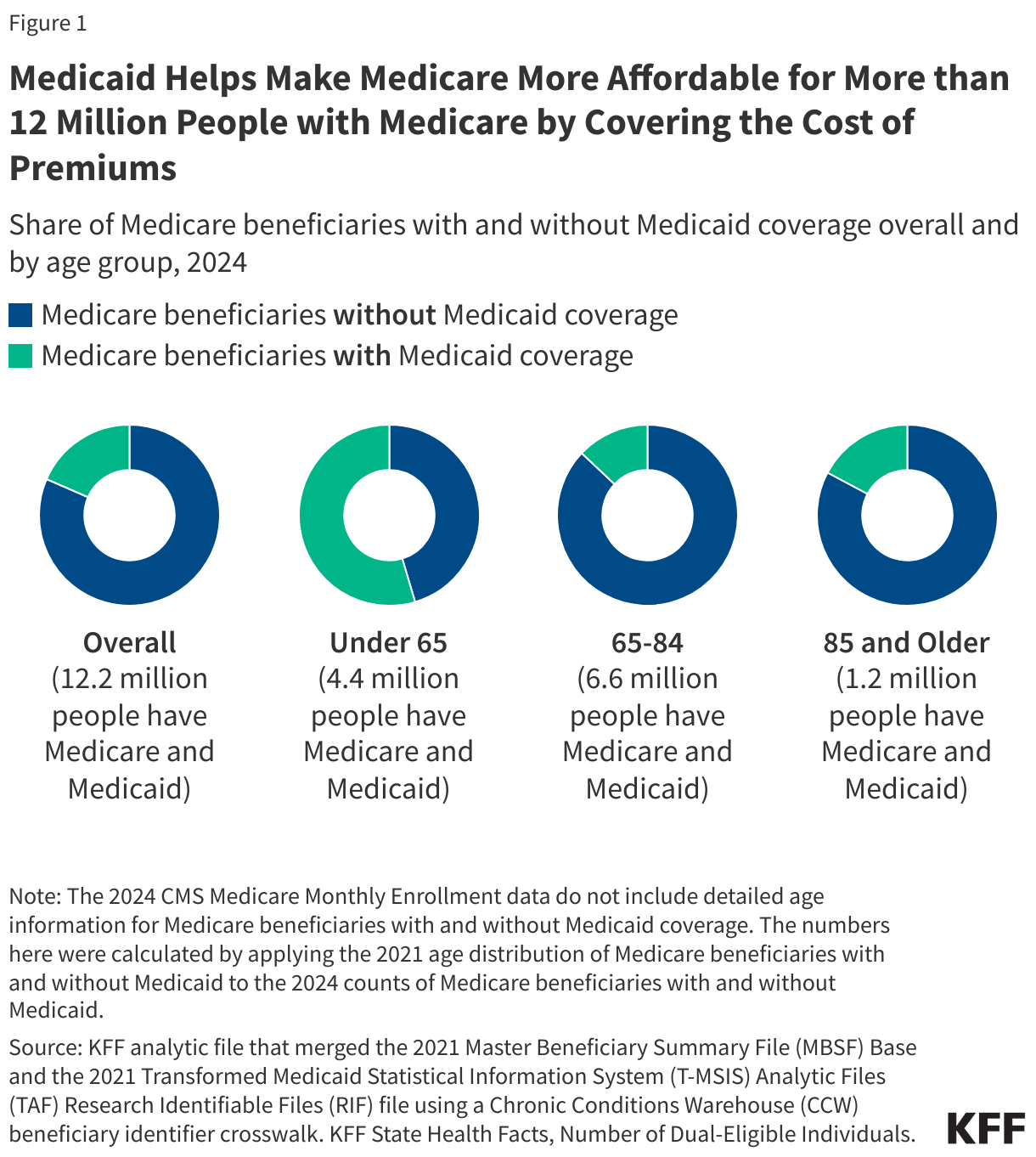
1. Medicaid helps make Medicare more affordable for more than 12 million people with Medicare by covering the cost of premiums.
Nearly 1 in 5 (18%), or 12.2 million Medicare beneficiaries also have Medicaid coverage (Figure 1). Most Medicare beneficiaries with Medicaid have low incomes and modest savings, and Medicaid coverage makes the Medicare program more affordable by paying premiums, and in most cases, cost sharing. Medicare Part B premiums are $185 per month in 2025 and without Medicaid, these premiums alone would consume close to 15% of income for people in poverty. Most Medicare beneficiaries with Medicaid also get help from Medicaid to pay their Part A and B deductibles, coinsurance, and copayments through the Medicare Savings Programs, which provide coverage of Medicare premiums and often, cost sharing, to Medicare beneficiaries with limited financial resources. Many dual-eligible individuals receive additional Medicaid-covered wraparound services, such as long-term care, vision, and dental services. Just over half (55%) of Medicare beneficiaries who are under age 65 (who are eligible for Medicare on the basis of a permanent disability) are also covered by Medicaid. Most people with both Medicare and Medicaid receive benefits from separate Medicare and Medicaid coverage arrangements. In 2021, just 5% of people with Medicare and Medicaid were in a program that covered Medicare and Medicaid benefits under a single plan or program with integrated financing.
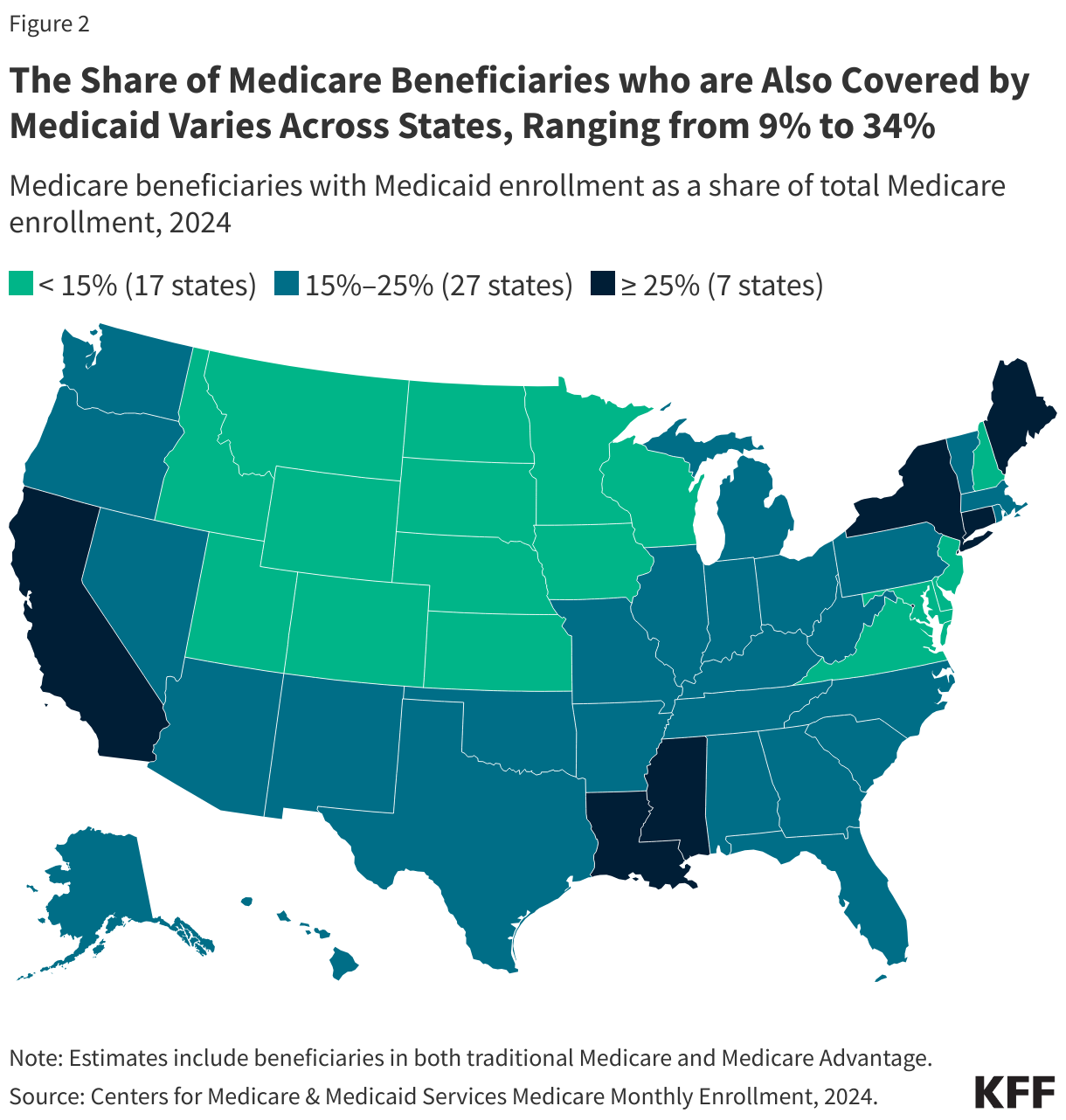
2. The share of Medicare beneficiaries who are also covered by Medicaid varies across states, ranging from 9% to 34%.
Across the 50 states and the District of Columbia, the share of Medicare beneficiaries who are also covered by Medicaid ranges from 9% in New Hampshire to 34% in D.C (Figure 2). The variation stems from differences in eligibility criteria for Medicaid, as well as the income and asset levels of Medicare beneficiaries living in different states. The primary Medicaid eligibility pathways for people with Medicare are through Supplemental Security Income and Medicare Savings Programs, both of which are mandatory. In addition, there are several optional pathways that states can choose to use to expand coverage, making eligibility complex and different across states. In general, in states where more people meet Medicaid eligibility criteria—which may reflect either lower incomes among Medicare beneficiaries or higher income eligibility criteria, a higher share of Medicare beneficiaries are also covered by Medicaid.
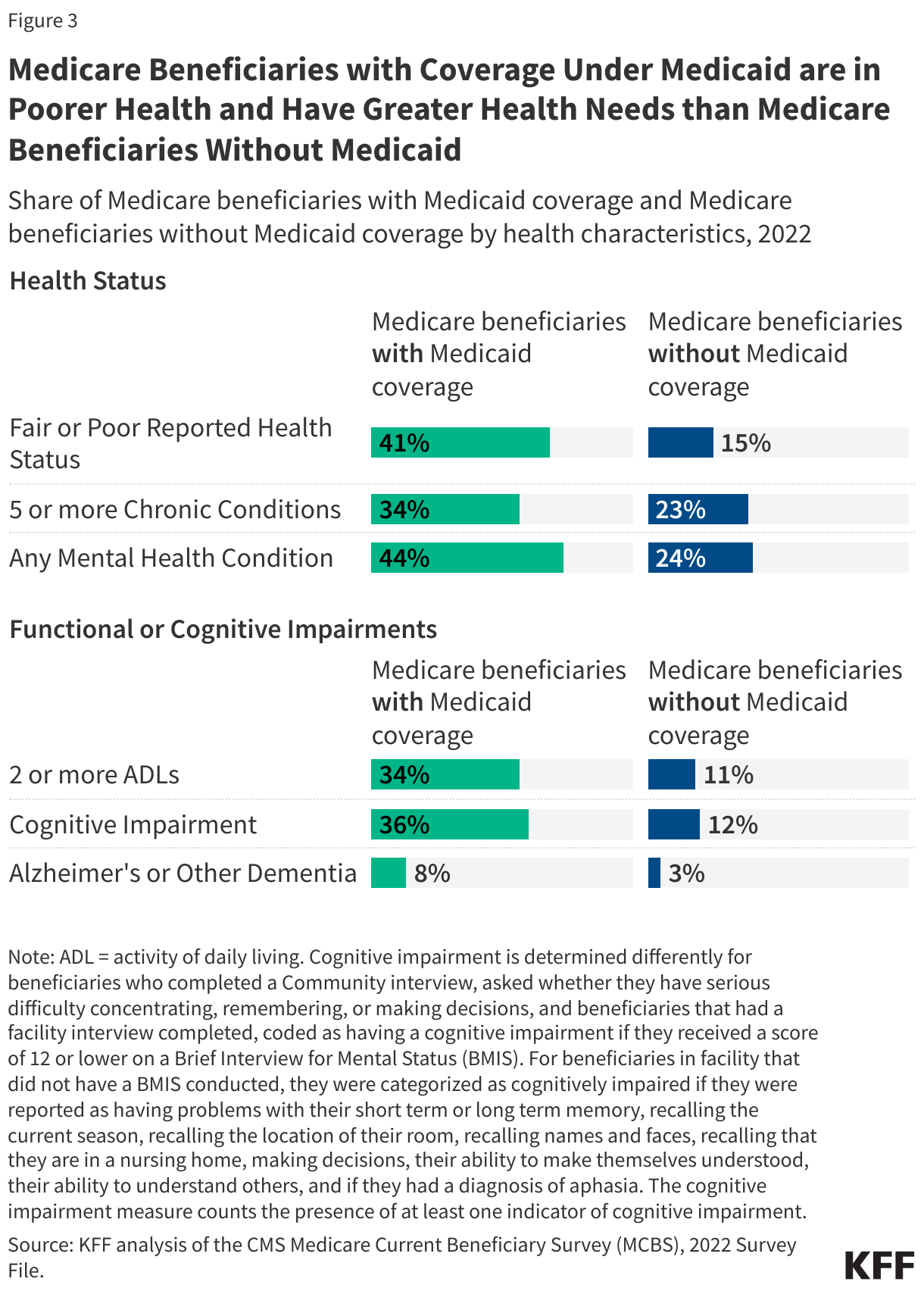
3. Medicare beneficiaries with coverage under Medicaid are in poorer health and have greater health needs than Medicare beneficiaries without Medicaid.
Four in ten (41%) people with both Medicare and Medicaid report their health as fair or poor, compared with 15% of Medicare beneficiaries without Medicaid coverage (Figure 3). More than a third (34%) of those with both Medicare and Medicaid have five or more chronic conditions, such as diabetes, hypertension, and heart disease, compared with 23% of Medicare beneficiaries without Medicaid coverage. Additionally, more than four in 10 (44%) have at least one mental health condition, such as depression and schizophrenia, compared with 24% of Medicare beneficiaries without Medicaid coverage.
A larger share of people with both Medicare and Medicaid experience functional or cognitive impairments than Medicare beneficiaries without Medicaid coverage. More than a third (34%) report difficulties performing two or more activities of daily living—such as eating, bathing, and toileting—compared to 11% of Medicare beneficiaries without Medicaid coverage. Additionally, a higher share of people with both Medicare and Medicaid coverage have cognitive impairments (36% versus 12%) and Alzheimer’s or other dementia (8% versus 3%) than beneficiaries without Medicaid coverage.
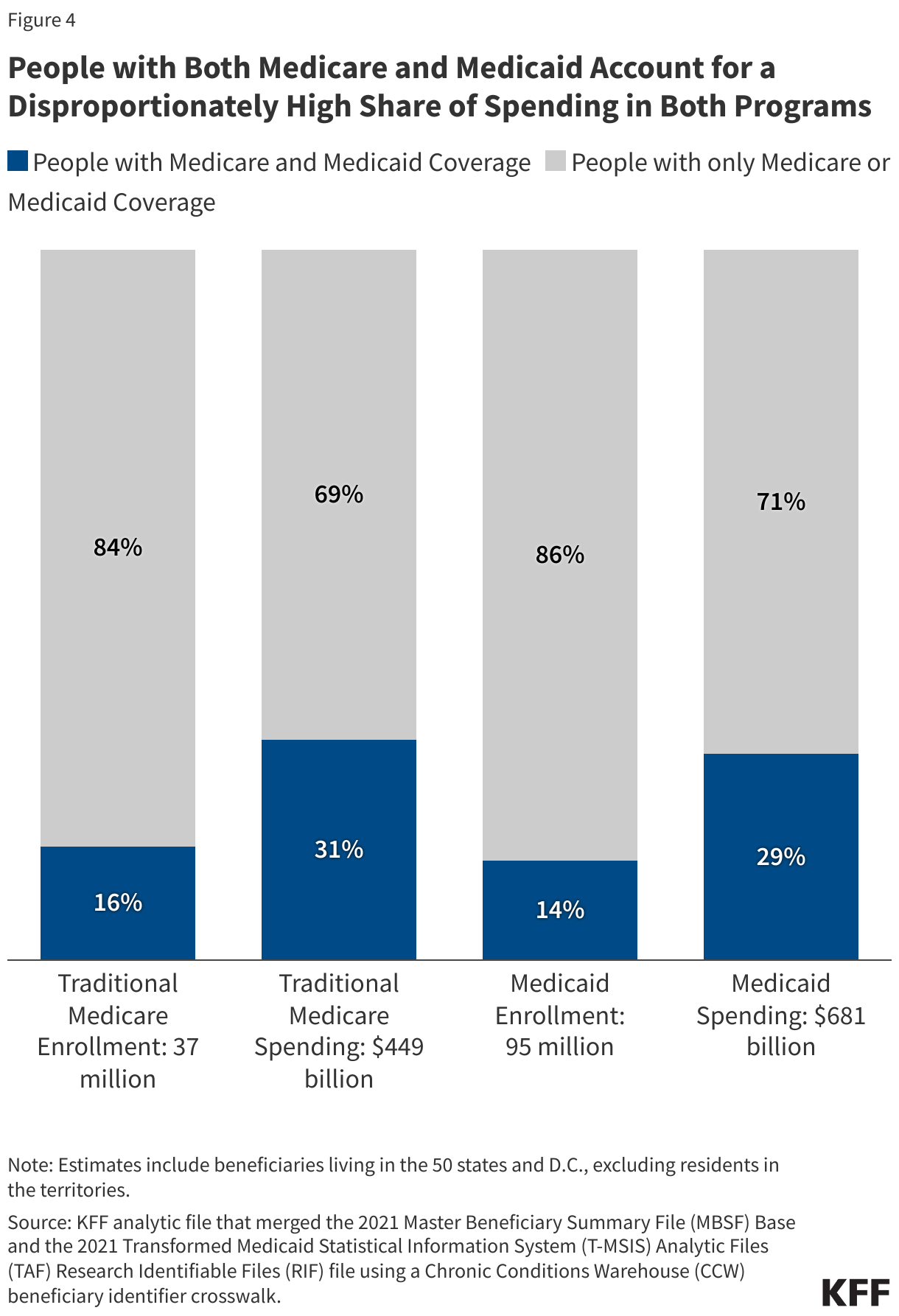
4. People with both Medicare and Medicaid account for a disproportionately high share of spending in both programs.
People with both Medicare and Medicaid comprise 16% of the traditional Medicare population and 31% of traditional Medicare spending in 2021 (Figure 4). Similarly, people with both Medicare and Medicaid comprise 14% of all Medicaid enrollment and 29% of federal and state Medicaid spending. The higher spending relative to enrollment is consistent with the greater health and functional needs of people with both Medicare and Medicaid. (People enrolled in private Medicare Advantage plans are not included in this analysis because Medicare comparable spending data are not available.)
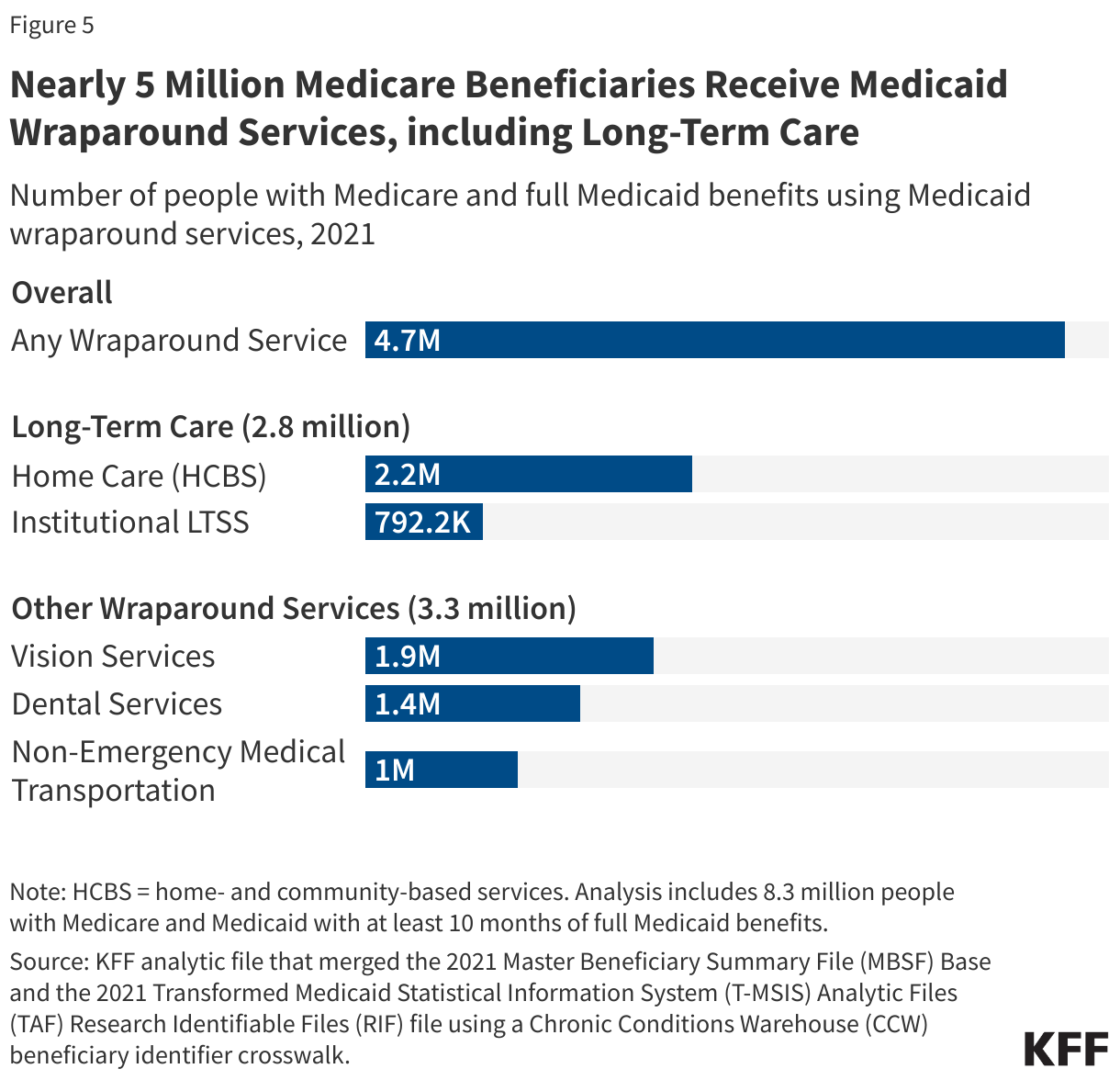
5. Nearly 5 million Medicare beneficiaries receive Medicaid wraparound services, including long-term care.
Almost 5 million Medicare beneficiaries with Medicaid used at least one of four Medicaid wraparound services in 2021, including long-term care, vision services, dental services, and non-emergency medical transportation (Figure 5). Medicaid wraparound services are Medicaid benefits available to most Medicare beneficiaries with Medicaid that are not covered under Medicare Part A or Part B. (The services may be covered as a supplemental benefit for people enrolled in a Medicare Advantage plan.) All states are required to provide some wraparound benefits including nursing facility care (part of institutional long-term care), home health (part of home care), and non-emergency medical transportation. Other services are optional for states to provide including dental services, vision services, and all other home care, which includes personal care, support for family caregivers, and services for people in assisted living facilities.
Medicaid covered vision services for 1.9 million Medicare beneficiaries, dental services for 1.4 million beneficiaries, and non-emergency medical transportation for 1.0 million Medicare beneficiaries. In addition, Medicaid covered long-term care services for 2.8 million Medicare beneficiaries (some of whom used both home care and institutional long-term care). Most of the people using long term-care (2.2 million) receive services in home and community settings. The costs of long-term care often exceed the median income and would quickly exhaust the median savings of Medicare beneficiaries, making Medicaid the primary payer of long-term care in the U.S., covering 61% of total spending.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.