What Does the Federal Government Spend on Health Care?
Congressional Republicans and President Trump are in search of trillions of dollars in cuts to mandatory federal spending that could help offset the cost of extending expiring tax cuts. With spending on health programs accounting for a substantial share of federal spending, those programs are an obvious target to achieve overall spending goals in current budget reconciliation discussions. Medicaid has been the primary focus for federal spending cuts, but cuts to Medicare and the Affordable Care Act have also been floated. Cuts to discretionary spending, which includes funding for several federal health agencies, veterans health care, and global health, are not part of the reconciliation process, but the Trump Administration has taken unilateral actions to reduce this spending. Proposed cuts to federal spending on health programs and services have trade-offs and could increase the number of people without insurance; reduce access to health care; increase consumer costs for health care; and reduce payments for hospitals, nursing homes, and other providers. The effects would be felt by people of all incomes but would likely be concentrated among people with low incomes.
To provide context for ongoing discussions about federal spending, this brief analyzes current support from the federal government for health programs and services, including both spending and tax subsidies (that is, forgone tax revenues from provisions that reduce tax liability for people and businesses with qualifying health-related spending). The data come from the Office of Management and Budget, U.S. Treasury Department, and the Congressional Budget Office (see Methods).
Key takeaways
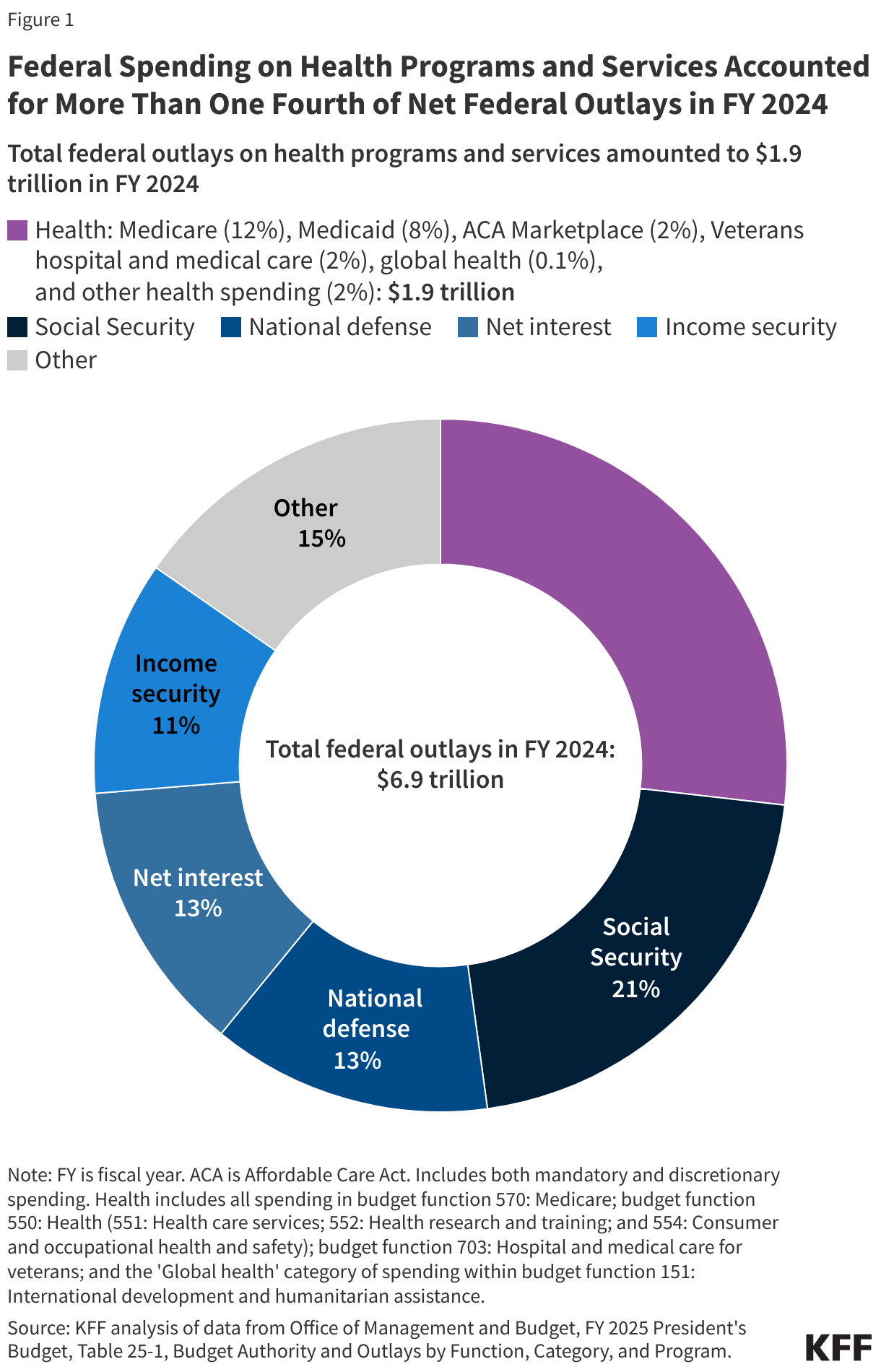
- The federal government spent $1.9 trillion on health care programs and services in fiscal year (FY) 2024, 27% of all federal outlays in that year, and collectively the largest category of federal spending.
- Forgone tax revenues to the federal government resulting from tax subsidies for employer sponsored insurance coverage (ESI) and a portion of the Affordable Care Act (ACA) premium tax credits together totaled $398 billion in FY 2024.
- Over 80% of all federal support for health programs and services, including spending and tax subsidies, goes to programs that provide or subsidize health insurance coverage, with 36% going to Medicare, 25% going to Medicaid and CHIP, 17% going to employment-based health coverage, and 5% going to subsidies for Affordable Care Act (ACA) coverage.
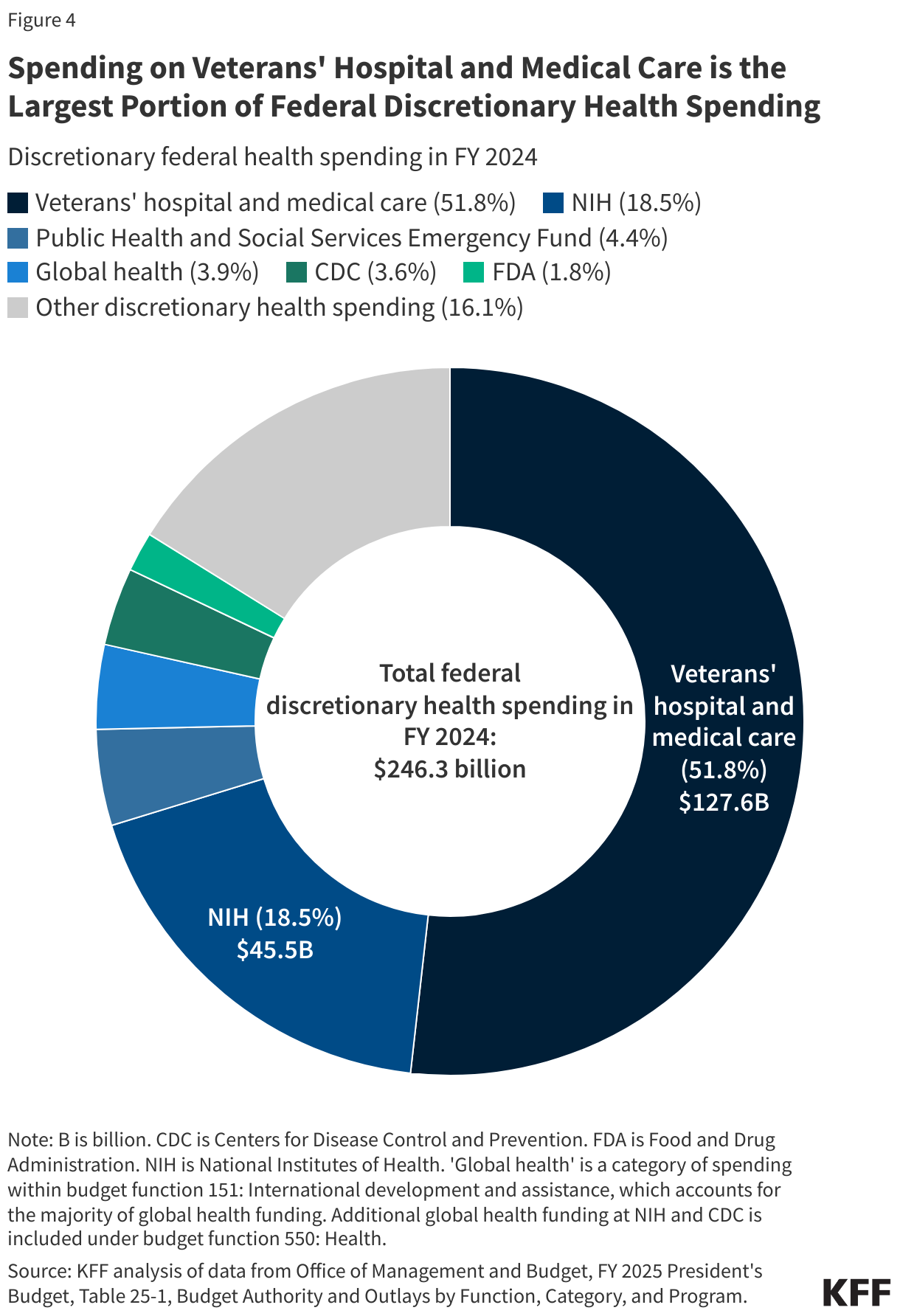
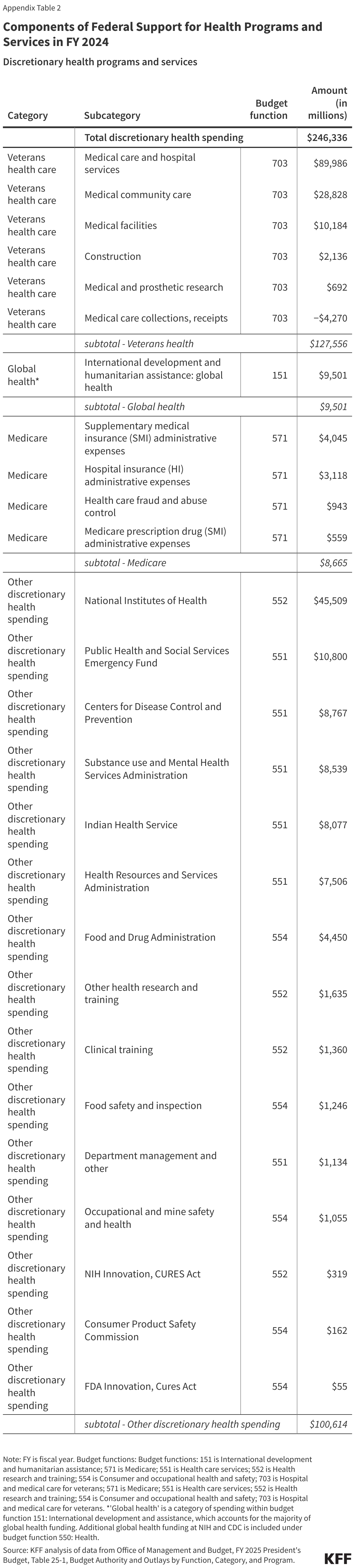
- Discretionary spending is a relatively small component of overall federal support for health programs and services. Over half (52% or $128 billion) of discretionary health spending paid for hospital and medical care for veterans. Discretionary health spending also provides funding for agencies such as the National Institutes of Health (NIH) (19% of discretionary health spending) and the Centers for Disease Control and Prevention (CDC) (4%), as well as global health (4%).
How does the federal budget support health programs and services?
Over one out of every four dollars in federal spending was used to pay for health programs and services in FY 2024 (Figure 1). The next largest categories are Social Security (21%), national defense (13%), and interest payments on the federal debt (13%). Combined, these four categories account for nearly three quarters of all federal spending.
Seventy percent of government support for health programs and services comes from mandatory spending, with tax subsidies accounting for 19% and discretionary spending accounting for 11% (Figure 2). There are three ways that the federal government provides support for health programs and services: mandatory spending (outlays), discretionary spending (outlays), and tax subsidies (forgone tax revenue, also called tax expenditures or tax preferences).
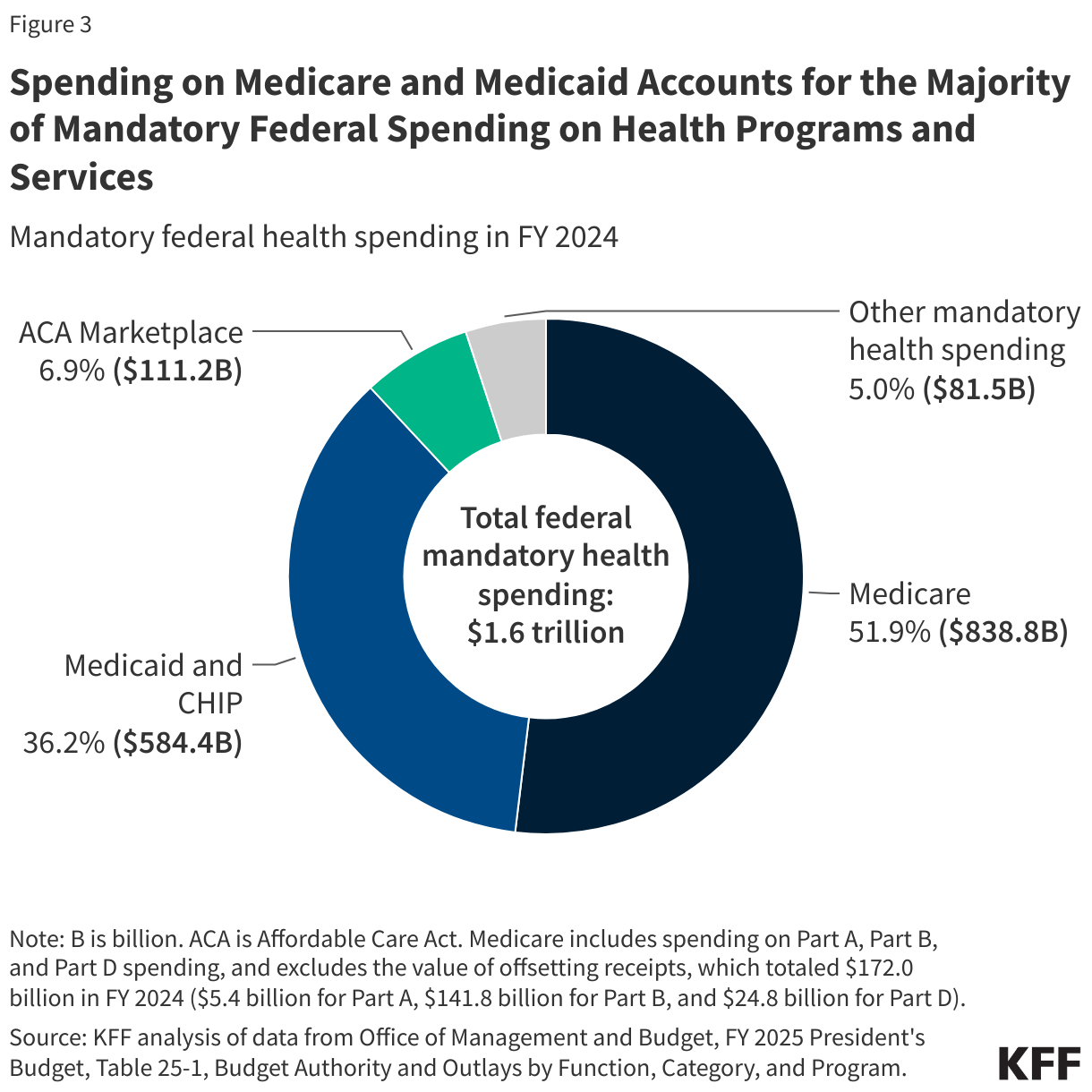
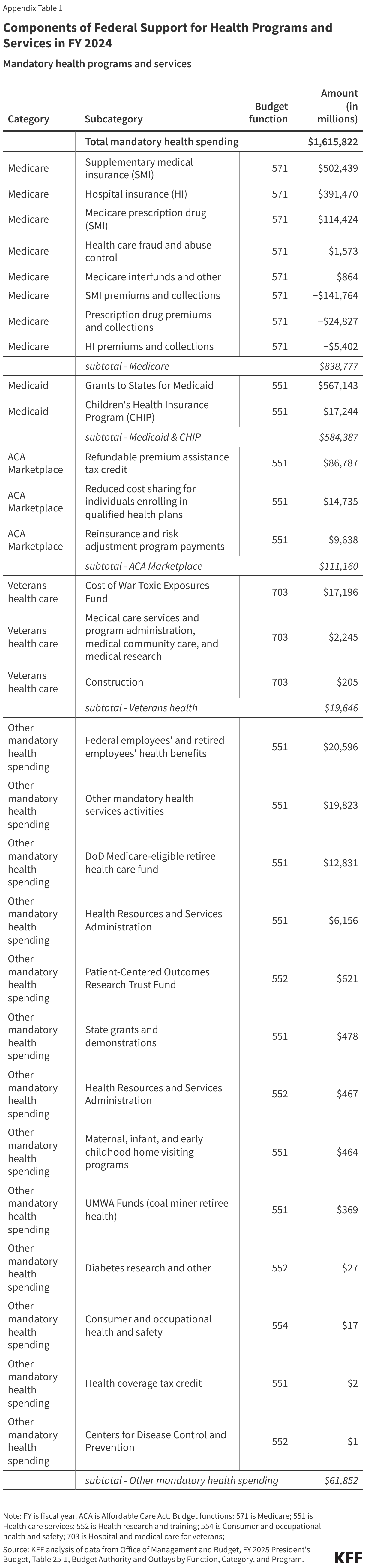
- Mandatory spending, also known as “direct spending,” is governed by regular legislative action in Congress and not determined through the annual appropriations or “spending” bills. Mandatory health spending includes nearly all Medicare spending ($839 billion), federal spending on Medicaid and CHIP ($584 billion in federal funding), and the refundable portion of the health insurance premium tax credit for coverage through the ACA Marketplaces ($111 billion in federal funding) (Appendix Table 1). (This does not include ACA premium tax credits that offset income taxes individuals owe to the federal government.)
- Discretionary spending is funded through annual appropriations bills. The largest component of discretionary health spending ($128 billion) is for veterans’ health care. Discretionary health spending also provides funding for agencies such as the National Institutes of Health (NIH) and the Centers for Disease Control and Prevention (CDC), as well as global health, or international health assistance, much of which is channeled through the Department of State and U.S. Agency for International Development (USAID). (For a more detailed discussion of federal funding for global health, including the potential impact of the Trump administration’s executive order pausing foreign aid, see KFF briefs, 10 Things to Know About U.S. Funding for Global Health, How Much Global Health Funding Goes Through USAID?, and The Status of President Trump’s Pause of Foreign Aid and Implications for PEPFAR and other Global Health Programs) (Appendix Table 2).
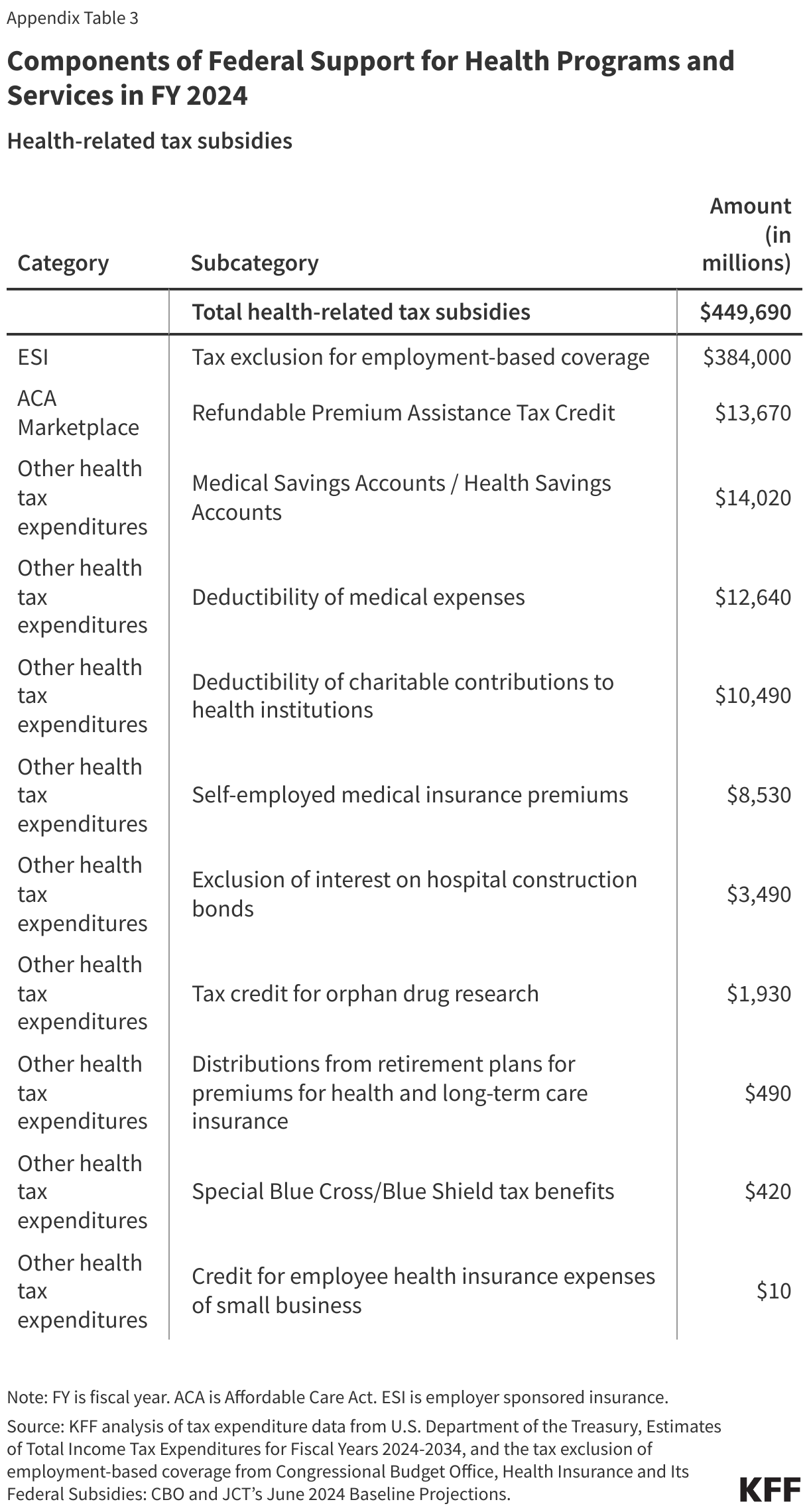
- Tax subsidies allow businesses and individuals to reduce the amount of taxes they must pay based on the amount of money they spend on qualifying health programs and services. Most of the foregone revenue to the federal government from health-related tax subsidies (85%) comes from the exclusion of employer contributions for health insurance, which totaled $384 billion in 2024. Other notable tax subsidies that support health care include the non-refundable portion of the tax credit for coverage through the ACA Marketplaces ($14 billion), contributions to medical and health savings accounts ($14 billion), deductions for medical expenses ($13 billion), and deductions for charitable contributions to health institutions ($10 billion) (Appendix Table 3).
What is the budget reconciliation process?
Congress will likely use reconciliation to make reductions in mandatory spending to help offset some of the cost of extending the expiring tax cuts. Budget reconciliation is a special legislative process used to make changes to taxes and mandatory spending that allows the Senate to pass legislation with only 50 votes rather than the customary 60 votes. There are limits to what kinds of legislation can be passed through budget reconciliation, and it can only be used for policies that make non-incidental changes to mandatory spending or revenues. Congress initially enacted the 2017 Tax Cuts and Jobs Act through reconciliation, and it is expected that the reconciliation process will be used again for an extension. That law made a set of broad but temporary tax cuts, which expire at varying years starting in 2025. The cost of extending these tax cuts has been estimated at $4.0 trillion between FY 2025 and FY 2034.
Reconciliation was originally intended to reduce budget deficits, and there are several unique rules governing the reconciliation process. The budget reconciliation process begins with the adoption of a budget resolution that is passed in both houses of Congress but not signed by the President. The budget resolution provides each Congressional committee with the dollar amount of budgetary changes that must be achieved over a specified budget “window,” which is usually either a five-year or ten-year period. These budget changes can either increase the deficit or decrease it. Budget resolutions often suggest specific policies to achieve budgetary changes, but those suggestions are not binding or enforceable. Committees of jurisdiction must meet the dollar targets in the budget resolution but have discretion as to how to meet the targets. A bill with all the details developed by committees would have to pass both houses of Congress and be signed by the president to become law.
To maintain privileged status in the Senate, a reconciliation bill cannot:
- Increase the deficit in years after the budget period (though it can increase the deficit during the budget period),
- Change Social Security spending or revenues,
- Be “extraneous” to the budget, meaning the reconciliation bill cannot include policies that have “merely incidental” fiscal impacts, or
- Make changes to discretionary spending.
How might a budget reconciliation package affect health insurance coverage?
There are four primary sources of health insurance coverage in the U.S.: Medicare, Medicaid, ACA Marketplaces, and employer sponsored coverage. Each of these sources of coverage could be subject to changes in a reconciliation bill. Of these four programs, Medicare accounts for the largest share (36%) of total federal support for health programs and services (including both spending and tax expenditures), followed by Medicaid and CHIP (25%), employer coverage (17%), and ACA Marketplaces (5%). Reconciliation could be used to reduce federal financial support for each of these programs because they are all funded through mandatory spending and/or financed with tax subsidies.
Existing discussions surrounding a reconciliation package have focused on reductions in mandatory federal health spending, the largest components of which are Medicare (52% of mandatory health spending) and Medicaid (36%) (Figure 3, Appendix Table 1). A 50-page menu of options for policies that could be included in a reconciliation package is largely focused on reducing federal spending to finance an extension of the 2017 tax cuts. Medicaid is the largest source of proposed cuts, but there are also options to reduce spending on Medicare and the ACA subsidies.
Medicaid: Medicaid covers 83 million low-income people, accounts for one fifth of health care spending in the U.S., and covers 61% of long-term care costs. Despite most adults having favorable views of Medicaid and only 13% thinking Medicaid cuts are a top priority, federal Medicaid funding ($584 billion in 2024, see Appendix Table 1) is at significant risk under Republican proposals to reduce federal spending by nearly one third over ten years. Changes to Medicaid under consideration include imposing a per capita cap on federal spending, reducing the federal government’s share of costs for the ACA expansion group, limiting provider taxes states use to help pay for their share of Medicaid costs, and imposing work requirements. Such policy changes would fundamentally alter how Medicaid financing works and large federal spending reductions would force states to make tough choices whether to raise new revenue, restrict the number of people covered, cover fewer benefits, or cut payment rates for physicians, hospitals, nursing homes, and other providers. Millions or even tens of millions of people could lose Medicaid coverage depending on how the policy was structured.
Medicare: Medicare provides health insurance coverage to nearly 68 million older adults and younger people with long-term disabilities and accounted for just over half (52% or $839 billion) of mandatory spending on federal health programs and services in FY 2024. Despite President Trump’s campaign promises not to cut Medicare, Republican lawmakers have put several Medicare savings proposals on the table in recent budget reconciliation talks, including implementing site-neutral payment policies, making changes to Medicare payment of uncompensated care, bad debt, and other hospital payments, and reforming Medicare payment for graduate medical education, among other changes. Altogether, these specific proposals could yield around $500 billion in 10-year savings, and would have the greatest impact on hospitals, with indirect effects on patients, depending on how hospitals responded to payment reductions.
ACA Marketplaces: Healthcare.gov and State-Based Marketplaces cover over 24 million people in 2025 (about 7% of the US population), most of whom are low-income. Federal support totaled $125 billion, including direct spending and tax subsidies in FY 2024, when about 19 million people received a subsidy.
ACA Marketplace subsidies are provided through the tax system, with most subsidized enrollees receiving an advanced payment of the premium tax credit, which they reconcile when they file their taxes the following year. Because incomes can be very volatile for ACA Marketplace enrollees (many of whom work shifts, are self-employed, or gig workers), predicting one’s income a year in advance can be difficult. The ACA currently limits how much an enrollee must pay back in the tax credit if their income is below four times the poverty level. However, a Ways and Means Committee document proposes to remove repayment limits for people who receive excess tax credits.
Since 2021, enhanced premium tax credits have lowered premium payments across all subsidized enrollees and made middle income people (over four times poverty) newly eligible for subsidies. These enhanced tax credits were originally passed as COVID relief and extended by the Inflation Reduction Act of 2022, but they are set to expire at the end of 2025. If the enhanced tax credits are not renewed by Congress, out-of-pocket premium payments for enrollees are expected to increase by over 75%, though this amount will vary by income and location. The cost to renew the subsidies would be $335 billion over ten years, according to CBO projections.
What health programs and services are discretionary, and subject to the annual appropriations process?
Only 11% of federal support for health care programs and services is discretionary spending, and over half of that amount (52%) pays for veterans’ health care (Figure 4, Appendix Table 2). In FY 2024, $128 billion in federal funding supported care for more than 7 million veterans. The next largest source of discretionary spending is the National Institutes of Health, which received $46 billion in 2024 (19% of discretionary spending). Smaller sources of federal discretionary spending include public health and social services emergency funding ($11 billion; 4%), global health ($10 billion; 4%), and the Centers for Disease Control and Prevention ($9 billion; 4%). (Global health totals presented here are outlays, which represent actual cash flows, and therefore do not match those presented in other KFF resources, such as the U.S. Global Health Budget Tracker, which highlight the budget authority totals as provided by Congress in annual appropriations and include some other funding components that are counted elsewhere in this analysis.)
Making changes to discretionary health spending through the appropriations process requires 60 votes in the Senate, meaning changes would require Democratic support, unless President Trump takes unilateral actions to reduce federal spending. Congress is supposed to pass appropriations bills by June 30 each year that provide funding for discretionary programs from October 1 through September 31 of the following year (the federal fiscal year). However, in most years, Congress does not pass the appropriations bills on time, and instead uses continuing resolutions to prevent lapses in federal funding for discretionary programs. The current continuing resolution funds the federal government through March 14, 2025. Extending funding for discretionary programs beyond that date will require a majority vote in the House and 60 votes in the Senate.
In the early weeks of President Trump’s second term in office, the administration has taken unilateral action to reduce federal funding, such as by laying off federal employees and issuing executive orders to freeze federal funding in various programs. Declining to spend appropriated funds is also known as “impoundment.” In 1974, Congress enacted the Impoundment Control Act in response to President Nixon’s attempts to refuse to spend Congressionally-appropriated funds. During the campaign, President Trump promised to “restore Impoundment Power,” and the administration characterizes the Impoundment Control Act as unconstitutional. The Trump administration also indicates that the current funding freezes are “programmatic delays” rather than deferrals. It is currently unclear the extent to which President Trump will be able to significantly reduce federal spending through these and other unilateral actions.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods |
| This analysis is based on data on federal outlays from the Office of Management and Budget (OMB) FY 2025 President’s Budget, tax expenditures from the U.S. Department of the Treasury, and the tax exclusion for employment-based coverage from the Congressional Budget Office (CBO). Specifically, we use FY 2024 data on federal outlays from Table 25-1. Budget Authority and Outlays by Budget Function, Category, and Program, FY 2024 data on tax expenditures from Table 1. Estimates of Total Income Tax Expenditures for Fiscal Years 2024-2034, and FY 2024 data on the tax exclusion for employment-based coverage from CBO, Health Insurance and Its Federal Subsidies: CBO and JCT’s June 2024 Baseline Projections.
The federal budget groups spending into roughly 20 categories called ‘budget functions,’ which are groups of activities or programs that fulfill specific purposes, such as defense, transportation, and health. This analysis focuses on non-defense health spending, which is defined to include spending in the following categories within four budget functions: 150: International Affairs: 151: International development and humanitarian assistance: Global health 550: Health: 551: Health care services 552: Health research and training 554: Consumer and occupational health and safety 570: Medicare 700: Veterans Benefits and Services 703: Hospital and medical care for veterans Each category includes both mandatory and discretionary spending, where applicable. Spending totals in this analysis are outlays, which represent actual cash flows, rather than budget authority, which represents the amounts authorized by Congress for new obligations by federal agencies. Global health outlay totals presented here do not match those presented in other KFF resources, such as the U.S. Global Health Budget Tracker, which highlight the budget authority totals as provided by Congress in annual appropriations and include some other funding components that are counted elsewhere in this analysis. As noted above, in this analysis ‘global health’ is a category of spending within budget function 151: International development and assistance, which accounts for the majority of global health funding. Additional global health funding at NIH and CDC is included under budget function 550: Health. This analysis does not include spending by the Department of Health and Human Services that falls outside of the ‘Health’ or ‘Medicare’ budget functions, which consists mainly of spending on social services and income security for children and families through the Administration for Community Living (ACL) and Administration for Children and Families (ACF), which falls within budget functions 500 (Education, Training, Employment, and Social Services) and 600 (Income Security). A separate KFF brief, How Does the Department of Health and Human Services (HHS) Impact Health and Health Care?, has a more complete description of these operating divisions within HHS. |