Medicaid Eligibility Levels for Older Adults and People with Disabilities (Non-MAGI) in 2025
To achieve the federal savings required by the House budget resolution, Congress would need to cut federal Medicaid spending by hundreds of billions of dollars, leaving states with significant budget shortfalls. Such policies could have major implications for older adults and people with disabilities who comprise 1 in 4 Medicaid enrollees but over half of Medicaid spending on account of higher per-person costs. Within this group, there are multiple eligibility pathways, most of which are optional for states to cover, and all of which have more complex eligibility requirements than coverage for other enrollees. Proposals to limit federal spending on Medicaid may pressure states to restrict Medicaid eligibility pathways, cover fewer optional benefits, and reduce provider payment rates. Coverage for people eligible through optional pathways, which are offered by all states, may be particularly at risk because of the high per-person costs of people enrolled through those pathways.
KFF’s Survey of Medicaid Financial Eligibility for Older Adults & People with Disabilities conducted in March 2025 by KFF and Watts Health Policy Consulting, provides a baseline of Medicaid eligibility as states return to normal operations after the end of the COVID-19 pandemic and ahead of potential changes to the Medicaid program. (These eligibility pathways are known as “non-MAGI” pathways because they do not determine eligibility based on Modified Adjusted Gross Income, as is the case for people covered under the Affordable Care Act Medicaid expansion and other groups.) Overall, 50 states including the District of Columbia (hereafter referred to as a state) responded to the survey, though response rates to specific questions varied. Florida was the only state that did not respond. Responses were supplemented with publicly available data and information from KFF’s past surveys when available, and state-level data are included in the Appendix Tables. Key takeaways include:
- States are generally required to provide Medicaid to people who receive Supplemental Security Income (SSI) and Medicare beneficiaries with limited income and savings. Eighteen states have increased the income or savings limits for Medicare beneficiaries beyond the federal minimums.
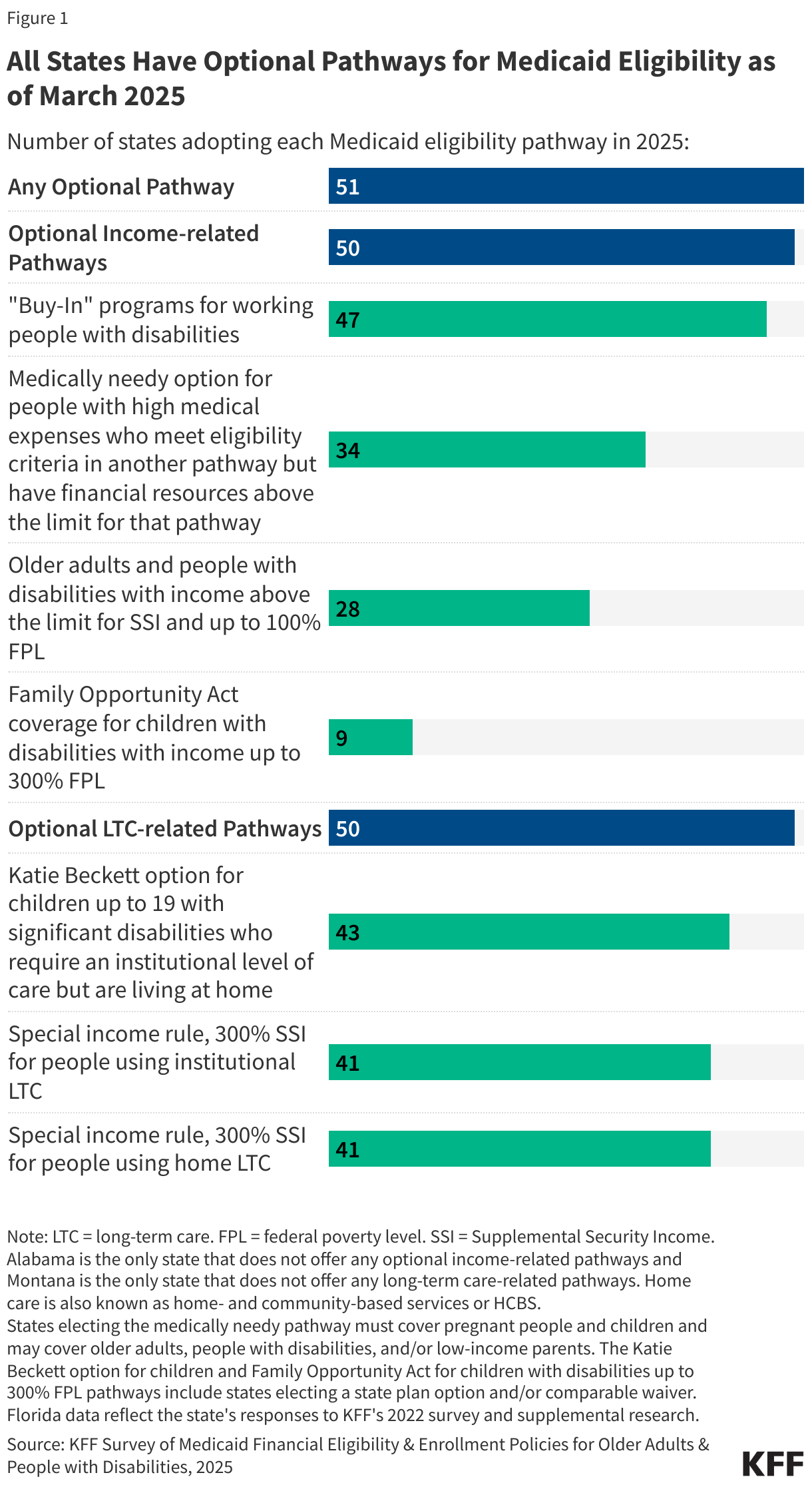
- Any optional pathway: All states also offer coverage through one or more optional eligibility pathways to people who have disabilities or are ages 65 and older who have limited financial resources.
- Optional income-related pathway: All states except Alabama extend eligibility to low-income adults with disabilities or people ages 65 and older who have income above the SSI limits (Figure 1).
- The most common income-based optional eligibility group is the Medicaid Buy-In for adults with disabilities who want to work, which is offered by 47 states.
- Optional LTC-related pathway: All states except for Montana offer optional coverage to people who use long-term care, people who tend to have much higher average spending than other Medicaid enrollees.
- Between 2024 and 2025, there were few changes in states’ eligibility requirements for older adults and people with disabilities, although 12 states increased the personal needs allowance for people using institutional care in 2025, with South Dakota reporting the largest increase (from $60 to $100).
What are the two required eligibility pathways for older adults and people with disabilities?
States are only required to cover two eligibility groups for older adults and people with disabilities in Medicaid, both of which require people to demonstrate having limited income and savings. Federal statutes generally require states to enroll people who receive Supplemental Security Income (SSI) in Medicaid and to enroll eligible Medicare beneficiaries in the Medicare Savings Programs:
- SSI is a disability program that provides monthly income to people who are unable to work on account of a disability and who have limited income ($967 per month in 2025 for an individual) and financial resources below federal limits ($2,000 for an individual).
- The Medicare Savings Programs provide Medicaid coverage of Medicare premiums and in most cases, cost sharing to Medicare beneficiaries who have limited income ($1,781 per month in 2025 for an individual) and financial resources below federal limits ($9,660 for an individual in 2025). People who are eligible for the Medicare Savings Programs, but not full Medicaid, receive help only with Medicare costs, and not full Medicaid benefits.
States may choose to expand eligibility for the Medicare Savings Programs beyond federally-required minimum levels. As was the case in 2024, 33 states use federal eligibility criteria for the Medicare Savings Programs, and the remaining 18 states expanded eligibility beyond those limits (Appendix Table 2).
Which states offer optional Medicaid eligibility for low-income older adults and people with disabilities?
All states except for Montana offer optional Medicaid eligibility for low-income older adults and people with disabilities. There are four types of optional Medicaid eligibility pathways based on income for people with disabilities which include:
- Medicaid buy-in programs for working adults are available in 47 states in 2025, allowing working people with disabilities to “buy into” Medicaid by paying a premium when their earned income exceeds eligibility limits but falls below a percentage of the federal poverty level (FPL).
- In 2025, the median income limit was 250% of FPL ($3,261 per month in 2025) and median asset limit was $10,000 for an individual and $14,470 for a couple (Appendix Table 3).
- Over half of states (27 of 45 responding) have an age limit for these buy-in programs, typically ages 16-64.
- Most states (33 of 47 responding) reported premiums for buy-in enrollees, with the median premium being $25 in 2025.
- Medically needy coverage is available in 34 states in 2025, allowing people to qualify for Medicaid if their income or assets are higher than permitted under another pathway but below the medically needy limit after accounting for their health care expenses.
- Most income limits are low—usually below 50% of FPL and many states limit enrollees’ assets to $2,000 (Appendix Table 4).
- Unlike income limits for other eligibility pathways, medically needy limits are generally established as a dollar amount. The median income limit increased from $504 in 2024 to $511 in 2025.
- Poverty level coverage is available in 28 states, allowing low-income older adults and people with disabilities to qualify for Medicaid when their income exceeds the SSI limits. States with this type of coverage generally establish income eligibility as a percentage of the SSI benefit rate or federal poverty level ($1,305 per month for an individual in 2025). Among the states that have expanded eligibility above SSI levels:
- 11 states have eligibility above SSI but below FPL,
- 15 states have eligibility at FPL, and
- 2 states have eligibility above FPL (Appendix Table 5).
- Coverage through the Family Opportunity Act, available in 9 states, allows families with incomes up to 300% of FPL to purchase Medicaid for their children under age 19 (Appendix Table 3). Parents who are eligible for coverage through an employer are required to pay premiums for private coverage too as a condition of Medicaid eligibility. In such cases, Medicaid covers the services children with disabilities need which are often not covered by private coverage.
- In 2025, the median income limit was about 265% of FPL ($3,452 per month) and 7 states had no limit on assets.
- Family Opportunity Act coverage is another type of “buy in,” with 5 states charging premiums in 2025. Premiums vary with family income and the median premium started at $12 per month for families with an income of 150% FPL.
What states offer optional Medicaid eligibility for people who use long-term care?
All states except for Montana offer optional Medicaid eligibility for people who use long-term care. Recognizing the high costs of long-term care, eligibility for people who use long-term care is almost always 300% of the SSI limit ($2,901 per month per individual in 2025), and most states limit enrollees’ assets to $2,000 per person (Appendix Table 6). The pathways include:
- Katie Beckett coverage is available in 43 states, allowing children under 20 with significant disabilities who require an institutional level of care to receive Medicaid while living at home. Only the child’s income and assets are considered for eligibility purposes, which allows some children of higher-income families to qualify. Like Family Opportunity Act coverage, children with Katie Beckett coverage may also have private health insurance, and 7 states charge families premiums for Medicaid.
- The special income rule allows states to extend Medicaid eligibility to people who require an institutional level of care and live in institutions or in home and community settings. Each pathway is available in 41 states, although Massachusetts offers coverage only for people using home care and New Hampshire offers coverage only for people using institutional care.
Most Medicaid enrollees who qualify because of long-term care are subject to limits on their home equity and must contribute to the cost of their care each month. In 2025, federal rules specified that limits on home equity must be between $730,00 and $1,097,000; and most states set the 2025 limit at $730,000 (Appendix Table 7). In all states, there are circumstances in which the home is exempt from limits, and other circumstances in which the home is counted as an asset when determining eligibility. California is the only state that does not have a home equity limit. Once eligible for Medicaid, enrollees who use long-term care must generally contribute nearly all monthly income to the cost of their care except for a small “personal needs allowance.” In 2025, the median personal needs allowance is $62 for institutional care and $2,901 for home care. Those limits were similar to the limits in 2024, although 12 states increased the personal needs allowance for institutional care in 2025, with South Dakota reporting the largest increase (from $60 to $100).
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.