Medicaid Efforts to Address Racial Health Disparities
Racial and ethnic disparities in health remain persistent in the United States, driven by inequities in access to and utilization of health care and social and economic factors that drive health, often referred to as social determinants of health (SDOH), that are rooted in historic and ongoing racism and discrimination. As a major source of health coverage for people of color, Medicaid programs are an important potential mechanism to address racial health disparities. Recent coverage gains across racial and ethnic groups between 2019-2022 were largely driven by increases in Medicaid enrollment as disenrollments were paused for three years during the pandemic related continuous enrollment provision. However, unwinding of the continuous enrollment provision could have disproportionate effects on people of color.
The federal government and many states have identified advancing health equity and addressing health disparities as a key priority. This includes President Biden’s Executive Order 13985 that directs federal agencies to take steps to advance racial equity. Other key efforts including improving collection and reporting of race and ethnicity data and focusing on maternal and infant health. While some efforts are broad, a number of efforts are specific to Medicaid. Medicaid coverage and other initiatives can help to address racial health disparities, but broader efforts to address structural racism and inequities within and beyond the health care system will also be key for reducing health disparities.
This issue brief aims to provide greater insight into key ways in which Medicaid can be leveraged to help address racial health disparities, drawing primarily from health coverage data, the 2023 KFF Budget Survey, and analyses from the KFF 1115 waiver tracker. While this brief documents some activities that states are implementing, take up of these initiatives varies across states and additional data are needed to determine if these efforts are effective at reducing disparities. Beyond the topics covered in this brief, states are engaged in other efforts to address racial health disparities in Medicaid and more broadly, including improving the collection and reporting of race and ethnicity data, establishing infrastructure to prioritize health equity, engaging with community to inform policy, and enhancing workforce capacity to provide culturally and linguistically appropriate care. This brief examines three key questions:
- How does Medicaid coverage vary by race and ethnicity?
- How can Medicaid eligibility policies mitigate racial disparities in coverage?
- What other Medicaid initiatives are states pursuing to address racial disparities in health and health care?
How does Medicaid coverage vary by race and ethnicity?
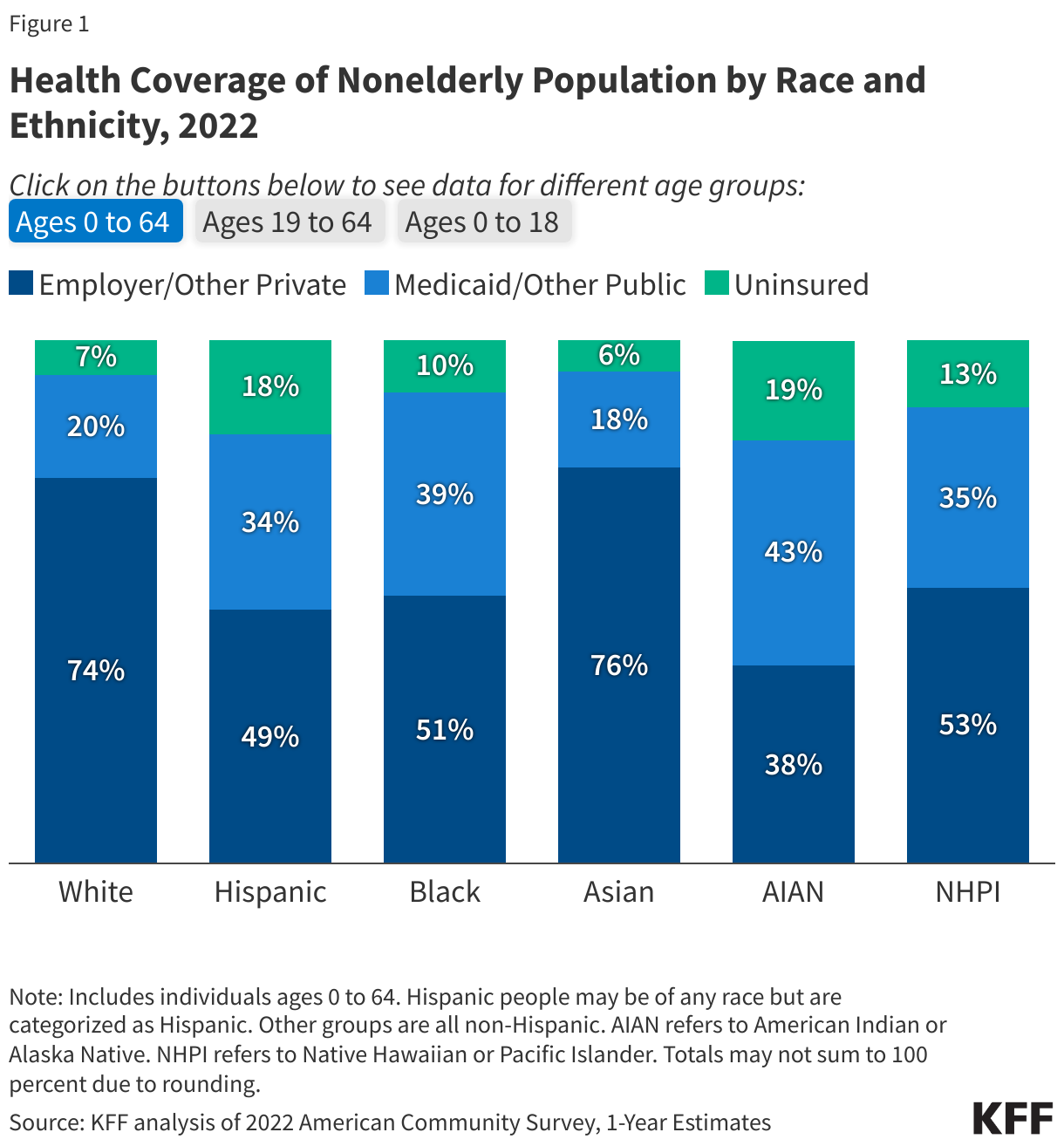
As a major source of coverage for people of color, the Medicaid program helps to ensure access to care and provide financial protection from health care costs. Research shows that uninsured people are far more likely than those with insurance to postpone health care or forgo it altogether. Being uninsured can also have financial consequences, with many unable to pay their medical bills, resulting in medical debt. Although employer-sponsored and other private coverage are primary sources of coverage across racial and ethnic groups, Medicaid helps to fill larger gaps in this coverage for many people of color, particularly children (Figure 1). Moreover, over time, gains in Medicaid coverage have helped to reduce racial disparities in coverage, particularly following the expansion to low-income adults under the Affordable Care Act (ACA). The continuous enrollment provision enacted during the COVID-19 pandemic contributed to additional Medicaid enrollment growth and uninsured rate reductions that further narrowed racial disparities in coverage.
The unwinding of the Medicaid continuous enrollment provision may have disproportionate effects on coverage for people of color. The unwinding of the continuous enrollment provision has resulted in millions of people being disenrolled from Medicaid, most often due to procedural or paperwork reasons, and net declines in Medicaid enrollments, with wide variation across states. While some individuals disenrolled from Medicaid may transition to other forms of health coverage, including Marketplace coverage, others may become uninsured or experience a gap in coverage before reenrolling in Medicaid. As Hispanic, Black, AIAN and NHPI people are more likely than their White counterparts to be covered by Medicaid, they are more likely to be affected by the unwinding. An early analysis of data from nine states reporting racial and ethnic data did not identify racial disparities in disenrollment rates. However, recent analysis of survey data found that Black and Hispanic adults who lost Medicaid coverage were about twice as likely as their White counterparts to report losing Medicaid coverage due to inability to complete the enrollment process. National survey data to assess changes in coverage by race and ethnicity during the unwinding period are lagged and will not be available for several years. The unwinding may also increase “churn,” in which enrollees disenroll and then re-enroll within a short period of time since continuous eligibility has been shown to reduce these coverage disruptions. There may be racial disparities in increases in churn rates. Analysis of earlier data found that churn rates increased among children across racial and ethnic groups following annual renewal, but Hispanic children had the largest increase, likely reflecting greater barriers to maintaining coverage.
How can Medicaid eligibility policies mitigate racial disparities in coverage?
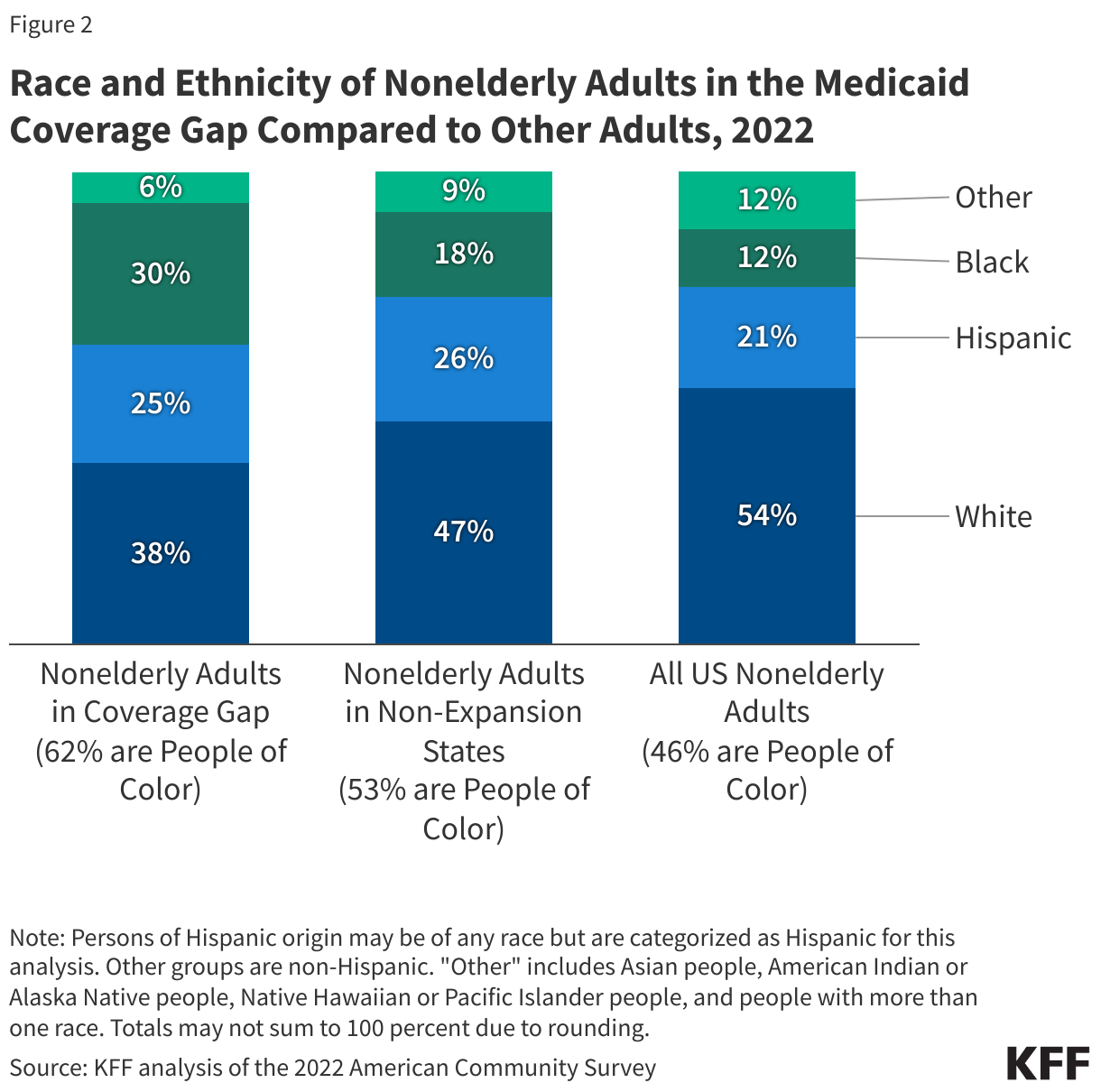
Adoption of the Affordable Care Act (ACA) Medicaid expansion in the 10 non-expansion states could help close coverage disparities for people of color. As of 2014, the ACA expanded Medicaid to adults with incomes through 138% of the federal poverty level ($20,783 annually for an individual in 2024). Research suggests that Medicaid expansion is linked to increased access to care, improvements in some health outcomes, and has contributed to reductions in racial disparities in health coverage compared to non-expansion states. However, as of May 2024, 10 states have not yet adopted the Medicaid expansion. In these non-expansion states, 1.5 million uninsured people fall in a coverage gap, with incomes too high to qualify for Medicaid but too low to qualify for Marketplace subsidies. Nationally, over six in ten people in the coverage gap are people of color, higher than their share of nonelderly adults in non-expansion states (53%) and overall (46%) (Figure 2).
Other expansions of Medicaid eligibility could also reduce racial disparities in coverage and access to care. Medicaid covers almost half of births nationally, including more than two-thirds among Black and American Indian or Alaska Native (AIAN) individuals, who have higher rates of pregnancy-related mortality and morbidity compared to White individuals. Historically, many people who qualify for Medicaid because they are pregnant lost that coverage after 60 days postpartum because Medicaid eligibility levels for parents are lower than for pregnant people, especially in non-expansion states, and postpartum Medicaid coverage was previously limited to 60 days. However, the American Rescue Plan Act (ARPA) included an option, made permanent in the Consolidated Appropriations Act, to allow states to extend postpartum coverage from 60 days to 12 months. As of May 2024, 49 states have implemented the extended the postpartum coverage period or plan to do so. In addition, beginning January 1, 2024, the Consolidated Appropriations Act required all states to implement 12-month continuous eligibility for all children in Medicaid and CHIP, and some states have applied for Section 1115 demonstration waivers that would extend multi-year continuous eligibility for children, which may reduce churn and coverage disparities.
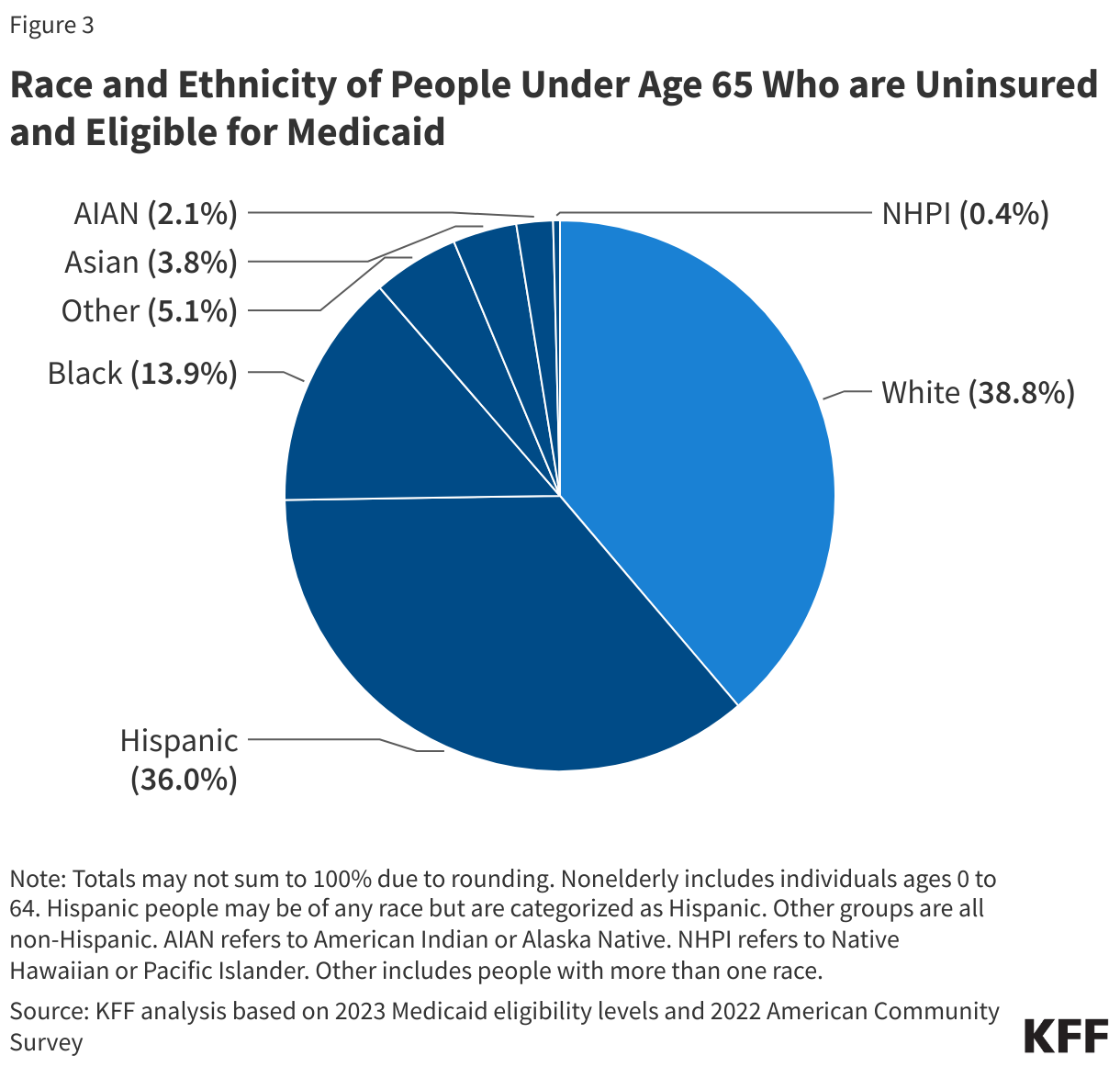
Increased outreach as well as policy changes to make it easier for eligible people to enroll in and maintain Medicaid coverage may also help reduce coverage disparities. In 2022, nearly two-thirds of the 6.4 million uninsured people were eligible for Medicaid but not enrolled were people of color (Figure 3). As noted above, this number may increase with the unwinding of the continuous enrollment provision. During the unwinding, states implemented an array of strategies to expand outreach, increase ex parte renewal rates, and streamline renewal processes, and many strategies will remain in place in the post unwinding period. Sustained outreach and enrollment efforts through trusted members in the community also is key for facilitating enrollment of certain populations, including those with Limited English Proficiency.
What other Medicaid initiatives are states pursuing to address racial disparities in health and health care?
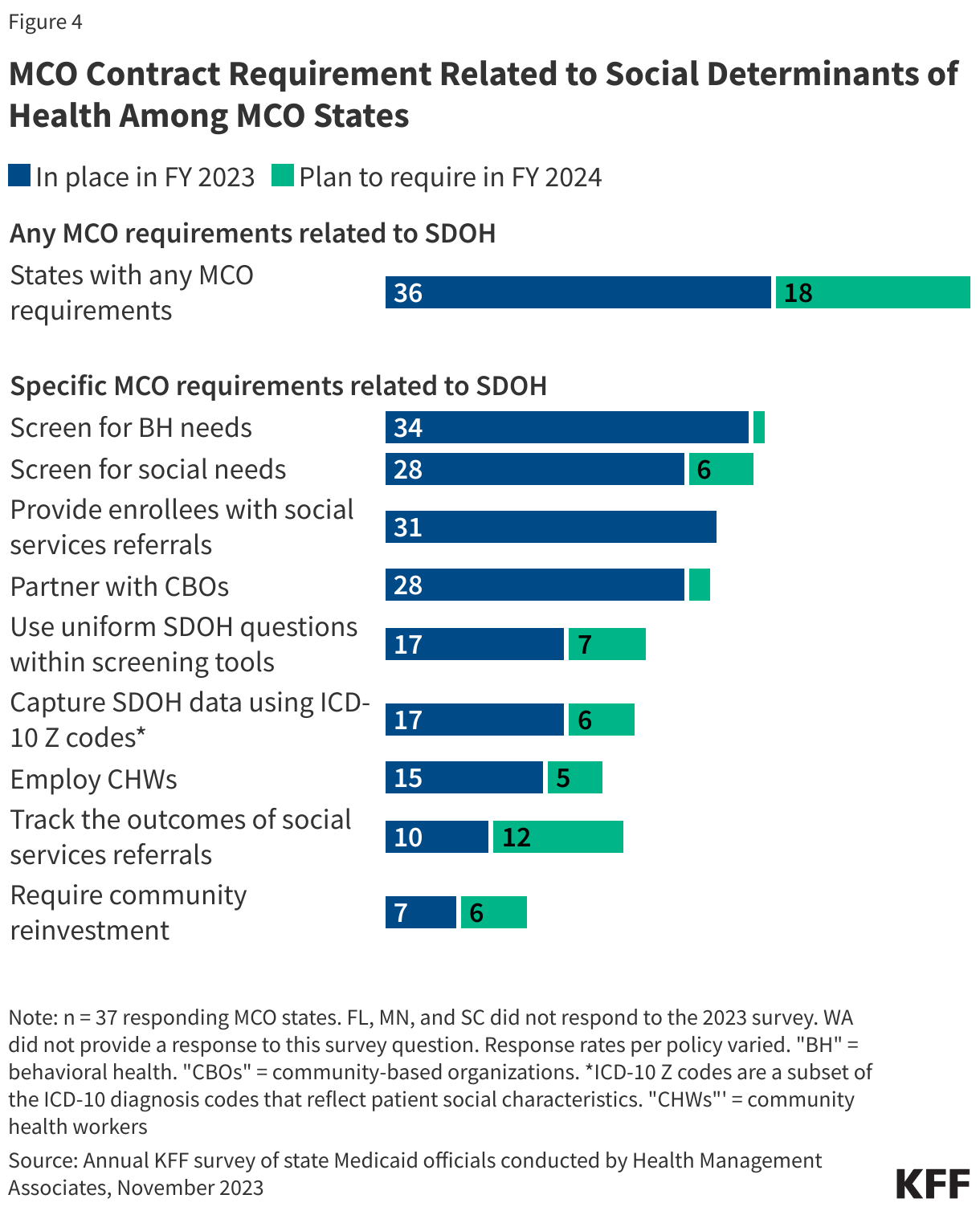
Most states that contract with managed care plans report leveraging MCO contracts to promote at least one strategy to address social determinants of health in FY 2023, which may help mitigate racial health disparities. Managed care is the dominant delivery system for Medicaid enrollees. As of 2021, 74% of Medicaid beneficiaries were enrolled in comprehensive managed care organizations (MCOs). States pay Medicaid managed care organizations a set per member per month payment for the Medicaid services specified in their contracts. According to KFF’s 2023 Medicaid budget survey, more than three-quarters of responding MCO states reported requiring MCOs to screen enrollees for behavioral health needs, provide referrals to social services, screen enrollees for social needs, and partner with community-based organizations (CBOs) (Figure 4). Fewer states reported requiring MCOs to track the outcomes of social service referrals or requiring MCO community reinvestment (i.e., directing plans to reinvest a portion of revenue or profits into the communities they serve) compared to other strategies.
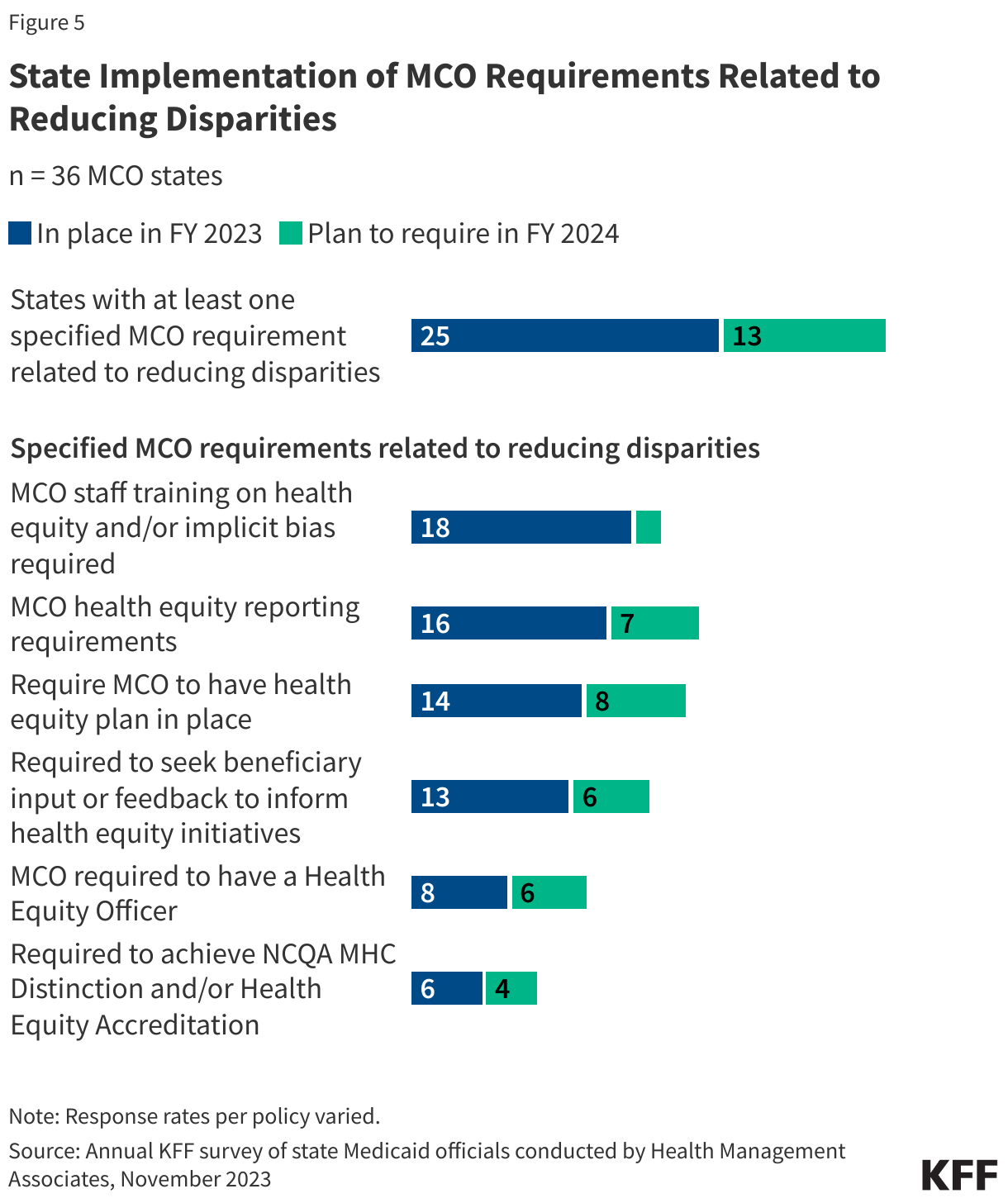
States also leverage managed care contracts in other ways to promote reducing health disparities. Some state MCO contracts incorporate requirements to advance health equity and states may also tie MCO financial quality incentives to reducing health disparities (Figure 5). Examples include:
- MCO financial incentives. States may use financial incentives to improve quality including linking performance bonuses or penalties, capitation withholds, or value-based state-directed payments to quality measures. About one-quarter of responding MCO states reported at least one MCO financial incentive tied to reducing racial and ethnic disparities in place in FY 2023. States most often reported linking capitation withholds, pay for performance incentives, and/or state-directed provider payments to reductions in health disparities.
- MCO contract requirements related to reducing disparities. In addition to financial incentives, states can leverage managed care contracts in other ways to promote reducing health disparities. For example, states can require MCOs to achieve national standards for culturally competent care, conduct staff training on health equity and implicit bias, develop new positions related to health equity, report data on racial and ethnic disparities, and incorporate enrollee feedback, among other requirements. According to KFF’s 2023 Medicaid budget survey, about half of responding states reported requiring MCOs to train staff on health equity and/or implicit bias and meet health disparities reporting requirements (Figure 5). Over one-third of states reported requiring MCOs to have a health equity plan in place and seek enrollee input or feedback to inform health equity initiatives. Fewer states reported requiring MCOs to have a health equity officer or achieve NCQA’s Multicultural Health Care (MHC) Distinction and/or Health Equity Accreditation.
- MCO performance improvement Projects (PIPs). States must require MCOs to implement PIPs to examine access to and quality of care, and these projects often include a focus on reducing health disparities. In FY 2023, states reported a range of state-mandated PIP focus areas with an emphasis on reducing disparities including those related to maternal and child health, chronic diseases, and substance use disorder.
States may pursue CMS approval of equity-related initiatives through Section 1115 waivers, which provide an avenue to test new strategies in Medicaid. The Biden Administration emphasized equity as a key goal of Section 1115 demonstration waivers. States may identify equity as an overarching demonstration goal that underlies all or most waiver provisions or may include specific equity-related provisions. States with an overarching demonstration focus on reducing health disparities or improving equity (e.g., California, New York, North Carolina, Oregon, Washington) often have similar areas of focus including integrating care (physical, behavioral, and social care), connecting enrollees to community-based organizations, managing population health, bolstering data infrastructure and addressing needs of specific populations (e.g., people experiencing homelessness, justice-involved people, people with substance use disorder (SUD), children/youth, and pregnant/postpartum people). States may also use 1115 waivers to expand Medicaid eligibility, add or enhance benefits, or make delivery system changes to address disparities and advance equity. Building on guidance released in 2021, CMS announced new flexibility available through Section 1115 to expand opportunities for states to use Medicaid to address enrollee health-related social needs (HRSNs) in late 2022. In 2023, CMS released guidance encouraging states to apply for 1115 waivers to test transition-related strategies to support community reentry for people who are incarcerated. These new demonstration opportunities are discussed in more detail below along with other 1115 initiatives focused on reducing disparities and advancing equity.
- HRSN waivers. As of June 2024, CMS has approved eight state HRSN waivers under the new HRSN 1115 framework. These waivers authorize evidence-based housing and nutrition services for specific populations with unmet social needs. CMS indicates broadening the availability of HRSN services is “expected to promote coverage and access to care, improve health outcomes, reduce health disparities, and create long-term, more cost-effective alternatives or supplements to traditional medical services.” States will be required to monitor and evaluate the impact of HRSN initiatives on utilization, cost, and health outcomes, including reporting on health equity metrics. A number of other states have approved 1115 waivers with SDOH-related provisions that pre-date the Biden administration HRSN framework. These waivers are generally narrower in scope (services and populations) or pilot programs focused on specific regions.
- Reentry waivers. As of June 2024, four states have approval to provide pre-release services to certain incarcerated, Medicaid eligible individuals. An additional 19 states have reentry waiver requests pending at CMS. Pre-release services include case management, medication-assisted treatment (MAT) for substance use disorders, and prescription medication upon release. People who are incarcerated have higher rates of mental illness, substance use disorder, and chronic and physical health care needs than the general population and are at high risk for unmet health needs and poor health outcomes upon release. Racial disparities in incarceration also exacerbate health disparities. Reentry services aim to improve care transitions and increase continuity of health coverage, reduce disruptions in care, improve health outcomes, and reduce recidivism rates. States will be required to monitor and evaluate the impact of these waivers as well.
- Delivery system reform and other equity investments. States may pursue other equity-related initiatives under 1115 including developing provider payment incentives tied to reducing disparities and/or obtaining “infrastructure” funding to support the implementation of HRSN waivers or build state or regional capacity to manage population health. For example, Arizona’s Targeted Investments 2.0 program provides funding that MCOs are directed to use to make incentive payments to providers with the goal of improving health equity for specified populations. As part of Massachusetts’ Hospital Quality and Equity Initiative, participating hospitals can earn performance-based incentive payments for meeting data collection requirements and improving health care quality and equity. New York’s Health Equity Regional Organization (HERO) is designed to develop regionally focused approaches to reduce health disparities, advance quality and health equity, and make recommendations to incorporate HRSN into value-based payment methodologies.
Expansions of Medicaid benefits may increase access to care for all enrollees, including the disproportionate share of people of color covered by Medicaid. KFF’s 2023 budget survey found many states reporting Medicaid benefit expansions, including benefits that may help reduce disparities. For example, to improve maternal and infant health outcomes and address racial and ethnic health disparities, states continue to expand and enhance pregnancy and postpartum services, including coverage of doula services, lactation services, and home visiting supports. Several states reported benefit changes to support access to culturally competent care, including coverage of community health workers. States also continue to report expansions of mental health and SUD services. Overall, rates of mental illness and SUD are lower for people of color compared to White people but may be underdiagnosed among people of color due to barriers in access to care. Additionally, people of color have experienced worsening mental health as well as increased rates of suicide and overdose deaths during the pandemic.