Fiscal Implications for Medicaid of Enhanced Federal Funding and Continuous Enrollment
For a three-year period, states provided continuous enrollment in Medicaid in exchange for an increase in the percentage of Medicaid spending that is paid for by the federal government (the Federal Medical Assistance Percentage or “FMAP”). A recent KFF analysis estimated that over 23 million people gained Medicaid coverage during the continuous enrollment period. Beginning April 1, 2023, states could begin disenrolling individuals from Medicaid, but phased-down federal matching funds will be available through the end of the year if states comply with certain rules. While there remains a great deal of uncertainty as to how Medicaid enrollment will change during the unwinding, the end of the Medicaid continuous enrollment provision and enhanced FMAP are expected to have a significant impact on Medicaid enrollment and spending. This brief examines how Medicaid spending changed during the continuous enrollment period and estimates the amount of enhanced federal funding states received during the continuous enrollment period. Key findings include:
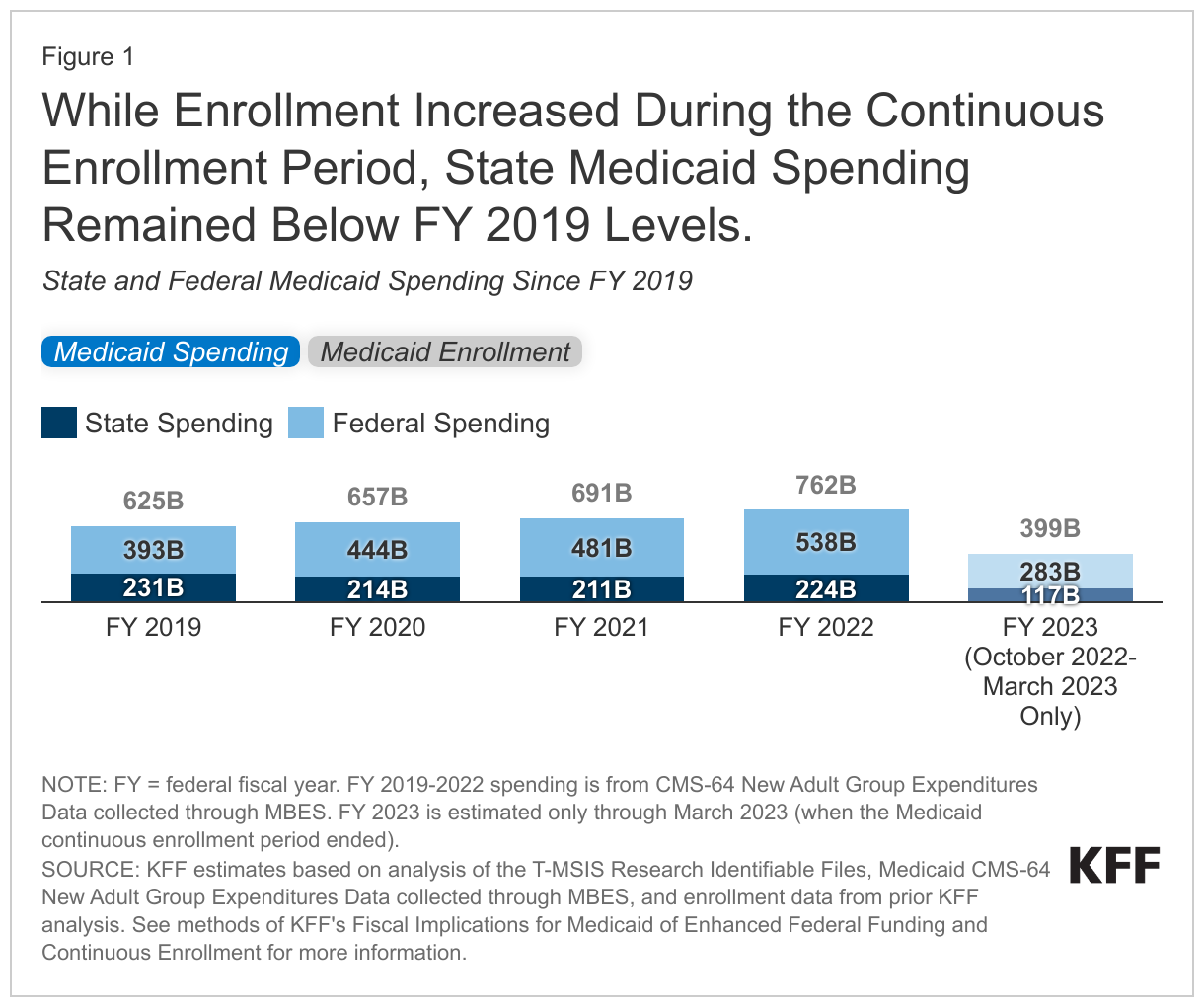
- State spending dipped below pre-pandemic levels even as Medicaid enrollment increased by 23 million during the continuous enrollment period. With the substantial enrollment growth, total spending increased, including significant increases in federal Medicaid spending due to the enhanced FMAP.
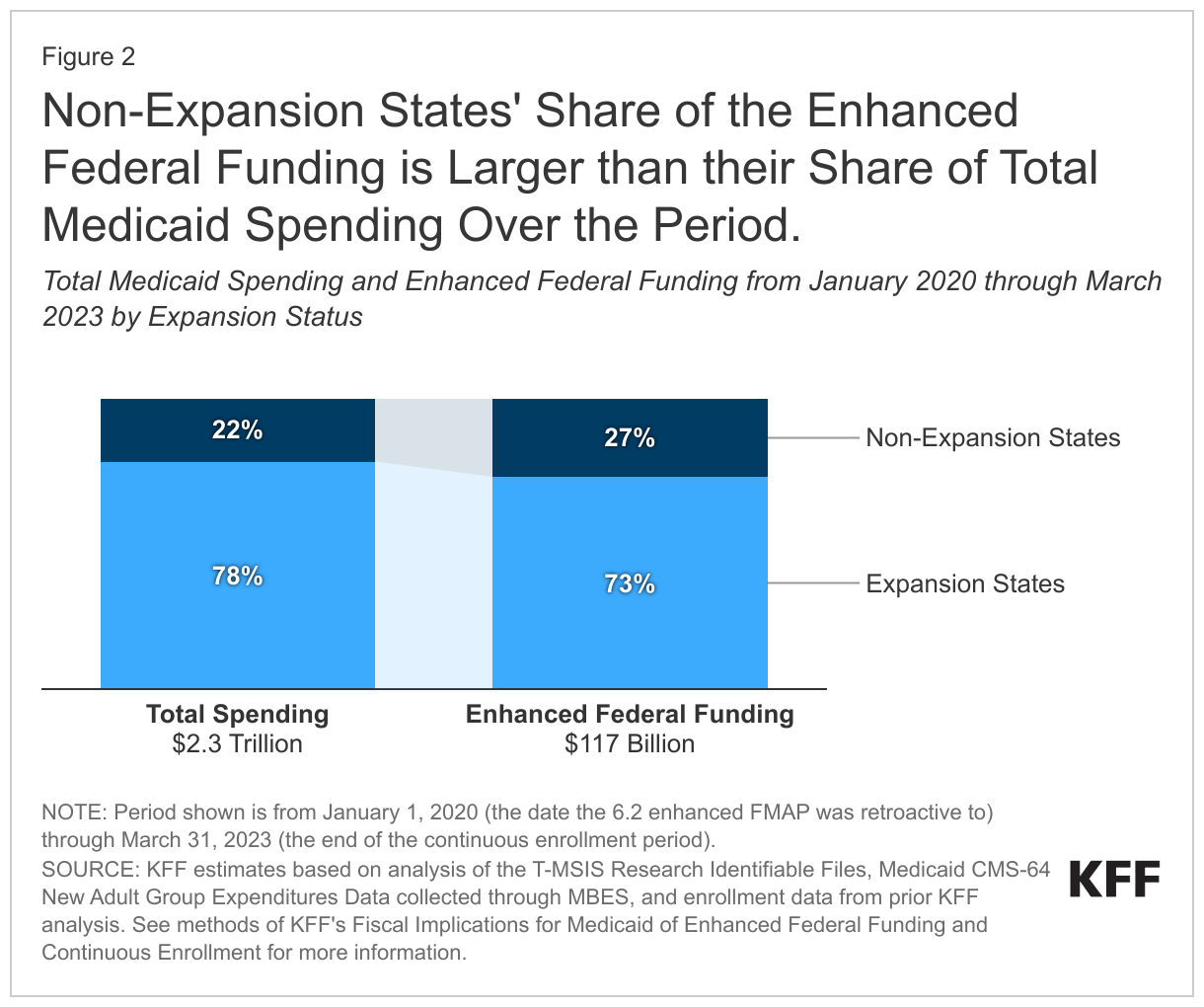
- We estimate states received over $117 billion from the increased FMAP during the continuous enrollment period, with enhanced federal funds comprising a larger share of total Medicaid spending in states that had not adopted Medicaid expansion through the Affordable Care Act (ACA).
- Although the magnitude is uncertain, significant decreases in Medicaid enrollment are expected during the unwinding of the continuous enrollment provision, which will result in lower Medicaid spending. Even with lower enrollment, state spending will likely increase as the enhanced FMAP expires.
- The phase down of the enhanced FMAP was designed to provide continued financial support to states during the unwinding process and to mitigate sharp increases in state Medicaid spending. How much state Medicaid spending increases as the enhanced FMAP phases down and is ultimately eliminated next year will depend on how many and how quickly people are disenrolled, how many new people come on to Medicaid, and how spending per person in the Medicaid program will change.
What was the purpose of the enhanced federal Medicaid match rate?
States received a 6.2 percentage point FMAP increase in exchange for keeping individuals continuously enrolled during the pandemic as authorized by the Families First Coronavirus Response Act (FFCRA). The increased FMAP was retroactive to January 1, 2020 and generally applied to Medicaid spending that would otherwise reimbursed at the state’s regular FMAP. The enhanced federal matching funds do not apply to administrative expenses or to Medicaid spending that is already subject to an increased match, including spending for ACA expansion adults (the FMAP is 90% for adults eligible through expansion). The Consolidated Appropriations Act, 2023 (CAA) delinked the continuous enrollment provision from the public health emergency (PHE), ending continuous enrollment on March 31, 2023. The CAA also phases down the enhanced federal Medicaid matching funds through December 2023, with the increased FMAP decreasing to 5 percentage points from April to June 2023, 2.5 percentage points from June to September 2023, and 1.5 percentage points from October to December 2023.
The federal funding from the enhanced FMAP was designed to support the costs of increased Medicaid enrollment and provide fiscal relief to states beyond the costs of enrollment growth. During economic downturns, enrollment in Medicaid grows, increasing state Medicaid costs while state tax revenues are declining. Congress enacted legislation to temporarily increase the federal share of Medicaid during the last two economic downturns prior to the pandemic. At the onset of the COVID-19 pandemic, states were projecting large revenue declines, but the enhanced FMAP provided new federal funding to states quickly by using an existing federal funding mechanism. Enhanced federal funding supported state Medicaid programs and helped free up state funds for other purposes including mitigating the need for widespread spending cuts on other services and filling gaps in state budget shortfalls.
How did Medicaid spending change during the pandemic?
State spending on Medicaid dipped below pre-pandemic levels even as enrollment in Medicaid increased by 23 million during the continuous enrollment period (Figure 1). The reduction in state spending reflected a sharp drop from $231 billion in 2019 to $214 billion in FY 2020, accompanied by an increase in federal spending of nearly $50 billion (from $393 billion to $444 billion). After 2020, state spending remained relatively stable while federal spending continued to increase due to the enhanced FMAP and total spending increased in conjunction with rising enrollment. State spending remained below 2019 levels in both expansion (defined as those having implemented Medicaid expansion as of 10/1/2021) and non-expansion states through the end of FY 2022. In the first six months of FY 2023—before the end of the continuous enrollment provision—we find that total and federal spending continued to increase while state spending returned to levels similar to the first two quarters of 2019. We expect spending and enrollment levels for the second half of 2023 to change, reflecting the end of the continuous enrollment period.
How much did states receive in enhanced federal funding during the continuous enrollment period?
During the continuous enrollment period, we estimate that states received over $117 billion in funding from the increased FMAP, with non-expansion states receiving a disproportionate share (Figure 2 and Appendix Table 1). Non-expansion states received 27% of the enhanced funding despite accounting for only 22% of all Medicaid spending because the enhanced FMAP does not apply to spending for people eligible through an ACA expansion. Across all states, the $117 billion in additional funding comprised an estimated 5% of total Medicaid spending and 7% of federal Medicaid spending during the continuous enrollment period (January 2020 through March 2023).
What might happen to Medicaid spending during the unwinding?
Although the size of the effects are quite uncertain, significant decreases in Medicaid enrollment are expected during the 14-month period in which states unwind the continuous enrollment period. KFF estimates that nationally Medicaid enrollment will decrease by 18% (17 million people) between March 2023 and May 2024 (based on a recent survey of states), but in practice, rates of enrollment decline will vary across states, depending on states’ approaches to unwinding. Early data from states shows substantial variation in disenrollment rates. While state Medicaid agencies report enrollment changes as the most significant factor driving changes in total Medicaid spending, they also note that factors such provider payment rate increases were putting upward pressure on spending. Overall, total Medicaid spending could decrease during the unwinding if the effects of enrollment losses are larger than the effects of other factors such as those.
Even with declining enrollment, state spending on Medicaid will likely increase as the enhanced FMAP expires. States are expecting the end of the enhanced FMAP to shift the state and federal spending shares, as has been the case in previous economic downturns when an enhanced FMAP expired. CBO estimates that federal spending will decrease by about 9% from FY 2023 to FY 2024. While states received substantial enhanced federal funding of $117 billion during the continuous enrollment period, they will likely see increases in state Medicaid spending as the enhanced federal matching funds expire at the end of the year.
The phase down of the enhanced FMAP was designed to provide continued financial support to states during the unwinding process and to mitigate sharp increases in state Medicaid spending. Before the CAA delinked the continuous enrollment provision and the enhanced FMAP from the PHE, the enhanced FMAP was set to expire at the end of the quarter when the PHE expired. The gradual phase-out of the FMAP through December 2023 recognizes that it will take states time to unwind the continuous enrollment provision and conduct redeterminations for all Medicaid enrollees. To be eligible for the enhanced match, states must meet certain eligibility, renewal, and reporting requirements. Recently, in a letter to CMS, Democratic lawmakers reiterated these beneficiary protections as well as CMS enforcement tools that were made available in the CAA, and CMS, in a letter to state governors, reiterated that states must comply with federal requirements to continue to draw down enhanced federal funds. The amount of the enhanced funding available to states during the unwinding will be smaller relative to the continuous-enrollment period, but it will still help mitigate the shift in funding from the federal government back to the states. As the enhanced federal funding is phased out and ultimately eliminated, the size of the increase in state Medicaid spending will depend on changes in total spending growth, which in turn will reflect how quickly people are disenrolled, how many new people come on to Medicaid, and how spending per person in the Medicaid program will change. These enrollment and spending changes will vary by state.
Appendix

| Methods |
| Data: This analysis uses the Medicaid CMS-64 new adult group expenditure data collected through MBES (CMS-64 data), the 2019 T-MSIS Research Identifiable Demographic-Eligibility and Claims Files (T-MSIS data), the May 2023 Congressional Budget Office (CBO) estimates of federal Medicaid spending per enrollee, and enrollment estimates from a prior KFF analysis.
Overview of Approach: To estimate total, federal, and state Medicaid spending as well as the enhanced federal funding states received from the increased FMAP, we:
Definitions and Limitations: While very similar at a national level, our estimates of the enhanced federal funding received over the period do not match those posted by the Medicaid CMS-64 FFCRA Increased FMAP Expenditure reports. There are a few reasons for this:
We provide more detail about each step in the process below. 1. Estimate Medicaid enrollment by eligibility group.
2. Prepare CMS-64 expenditure data and estimate spending per enrollee by eligibility group for FY 2019 – FY 2022 at the state level.
3. Estimate FY 2023 spending per enrollee. We only have full-year, detailed administrative expenditure data through June 2022, so we estimated expenditures for FY 2023.
4. Calculate total, federal, and state Medicaid spending during the pandemic with the enhanced FMAP.
5. Estimate enhanced federal funding.
|