An Examination of Medicaid Renewal Outcomes and Enrollment Changes at the End of the Unwinding
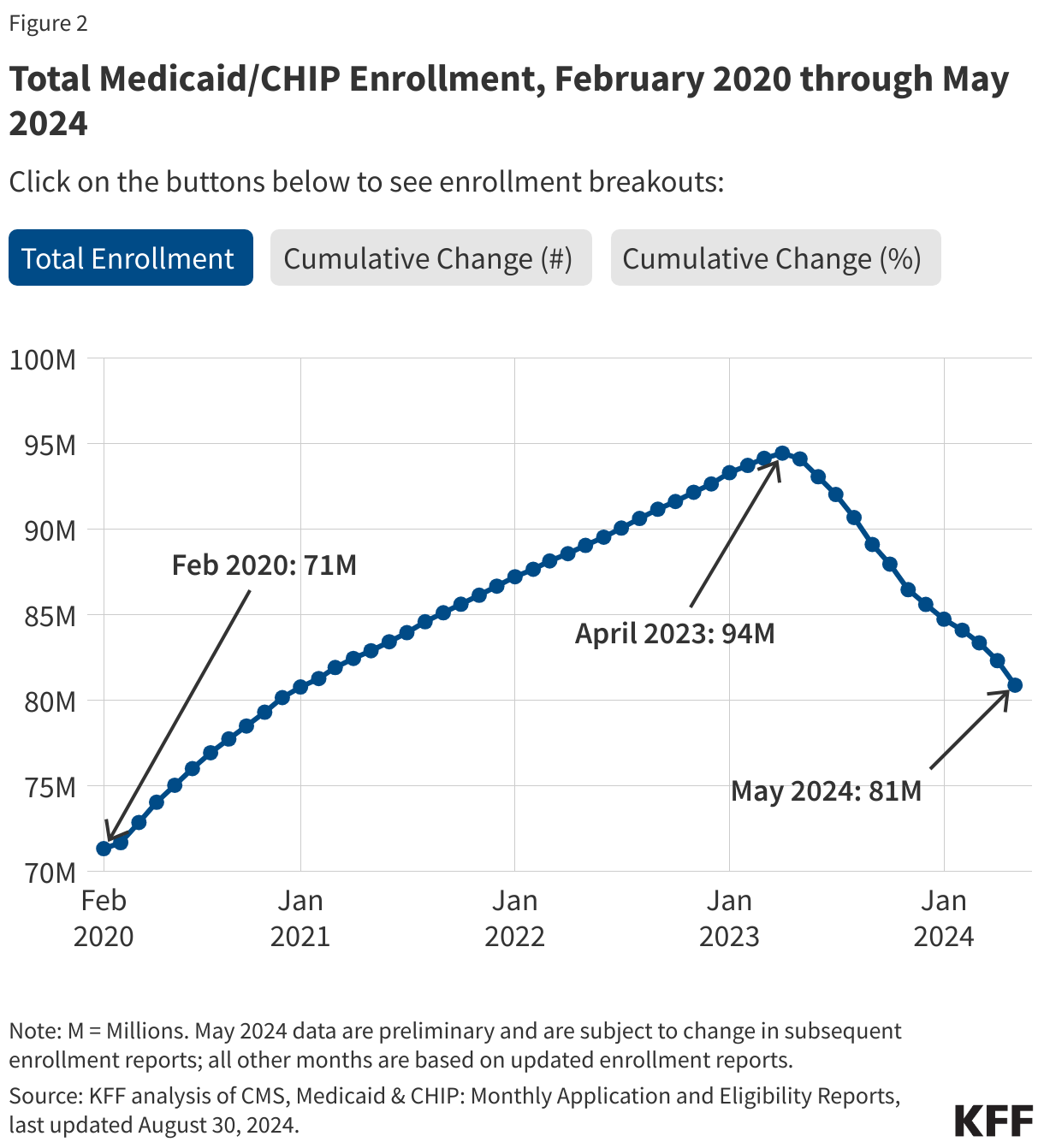
In April 2023, states began the process of unwinding the Medicaid continuous enrollment provision, a pandemic-era policy that protected Medicaid coverage for millions of enrollees. During the unwinding, states redetermined eligibility for everyone on the program and disenrolled those who were no longer eligible or who did not complete the renewal process. Before the start of the coronavirus pandemic in February 2020, there were 71 million people enrolled in Medicaid and CHIP. After the three-year pause in disenrollments, that number grew to a record high of 94 million people by April 2023, the month after the end of continuous enrollment. From the outset of the unwinding, there were major questions related to how many people would be disenrolled versus retain coverage and how that would affect overall Medicaid enrollment. Now that nearly all states have completed the unwinding of the Medicaid continuous enrollment provision, it is possible to take stock of overall renewal outcomes as well as where Medicaid enrollment stands and how current enrollment compares to pre-pandemic levels, nationally and across states. The Medicaid and CHIP enrollment data show more recent changes in enrollment that are not reflected in national survey data that report the overall uninsured rate in 2023 did not change from 2022, although there was an increase in the uninsured rate for children in 2023.
Using data from the KFF Medicaid Enrollment and Unwinding Tracker, this analysis reports data on unwinding renewal outcomes through June 2024 and examines Medicaid enrollment changes from February 2020 through May 2024, the most recent federal enrollment data available, nationally and across states. While the available data provide a nearly complete picture of renewals and disenrollments during the unwinding period, some data are preliminary with cases still pending in some states. These data mark the end of KFF’s independent effort to use state and federal data to monitor the Medicaid unwinding. Going forward, KFF will continue to track monthly Medicaid enrollment data reported by the Centers for Medicare and Medicaid Services (CMS).
Key Takeaways
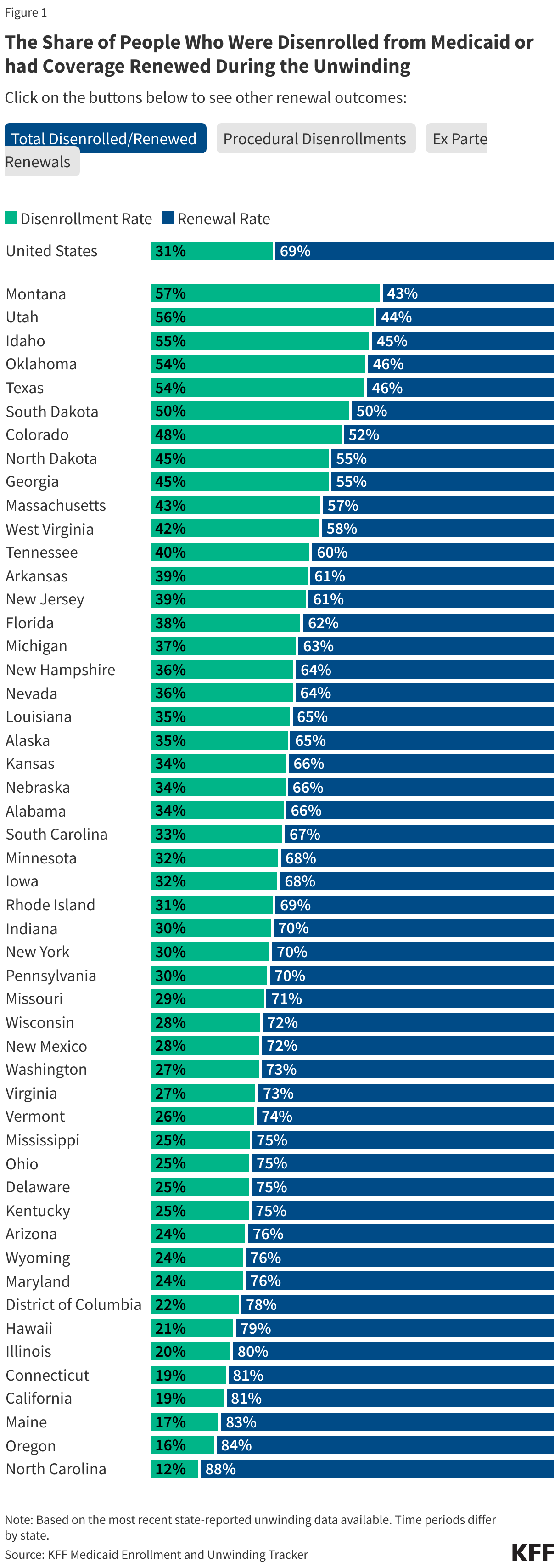
- During the unwinding of the Medicaid continuous enrollment provision, over 25 million people were disenrolled and over 56 million had their coverage renewed. Overall, 31% of people whose coverage was redetermined during the unwinding were disenrolled, but that share ranged widely across states. For example, five states—Montana, Utah, Idaho, Oklahoma, and Texas—have disenrollment rates over 50%, while five states—North Carolina, Maine, Oregon, California, and Connecticut—have disenrollment rates under 20%.
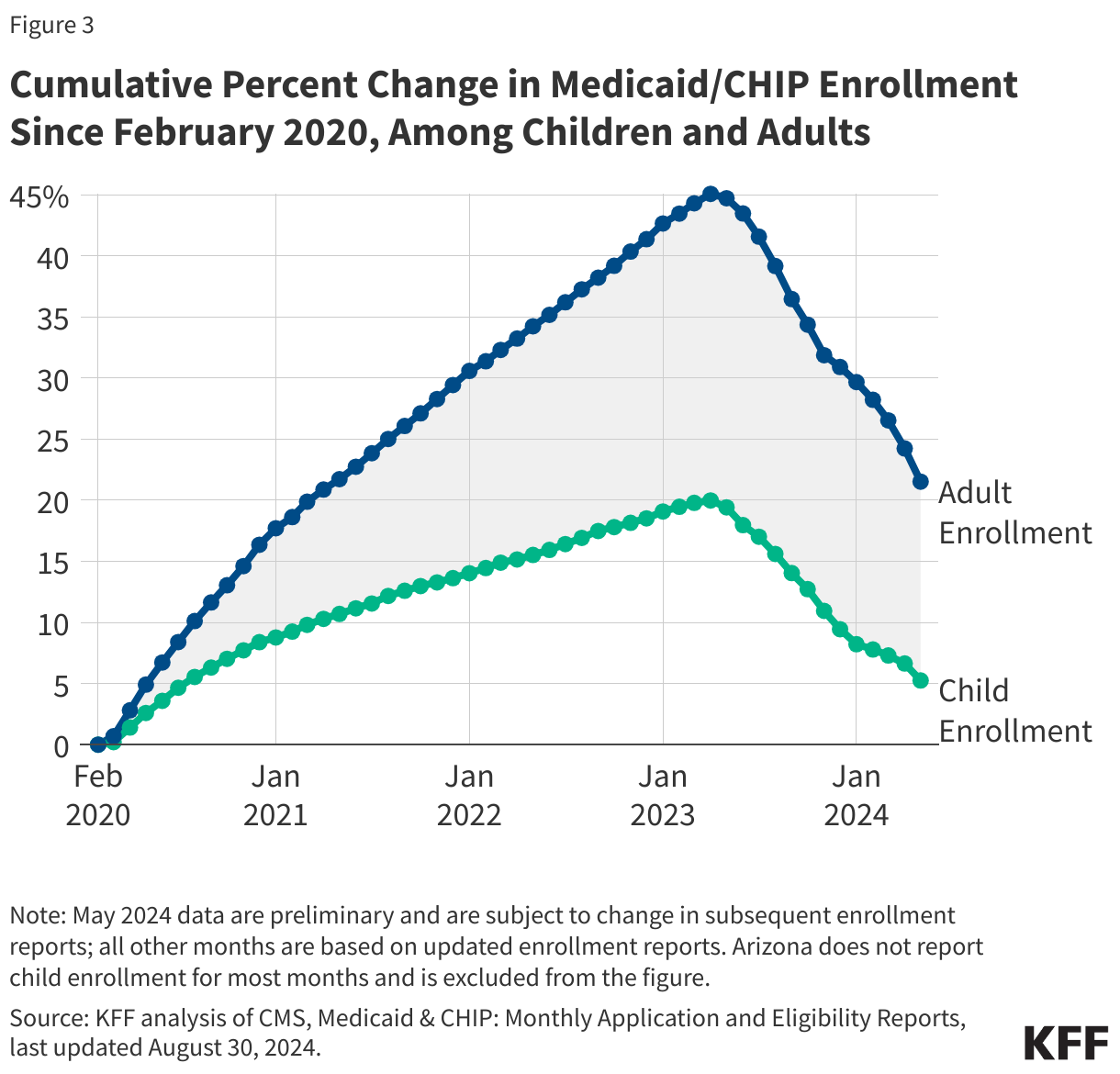
- Despite millions of disenrollments during the unwinding, nationally, nearly 10 million more people are currently enrolled in Medicaid/CHIP than at the start of the pandemic. While enrollment among adults is over 20% higher than in February 2020, child enrollment has nearly returned to pre-pandemic levels and is only 5% higher.
- Several factors likely explain the net growth in Medicaid enrollment. The pandemic may have encouraged some people who were previously eligible for Medicaid but not enrolled to newly enroll, and during the unwinding, many states took steps to improve their renewal processes to reduce the number of people who were disenrolled despite remaining eligible. In addition, several states expanded eligibility for certain groups, including five states that adopted Medicaid expansion since the onset of the pandemic.
- Similar to the national trend, Medicaid/CHIP enrollment in most states is higher than it was in February 2020; however, total Medicaid/CHIP enrollment has fallen below pre-pandemic enrollment in three states, Montana, Colorado, and Arkansas, and child enrollment is lower in 12 states.
A look back on both the period of continuous enrollment and the unwinding period provides numerous potential lessons for Medicaid policy:
The growth in Medicaid enrollment during the pandemic demonstrated that continuous enrollment can stabilize coverage by reducing churn in the program that occurs when eligible people are disenrolled and then reenroll within a short period of time. Beginning January 2024, states are required to provide 12 months of continuous eligibility for children (previously 12-month continuous eligibility for children was optional for states). Many states are expanding on that policy to provide multi-year continuous eligibility for young children, and in some cases, two-year eligibility for older children and adults even though these policies will likely increase state and federal Medicaid spending.
At the same time, providing continuous coverage increases spending and results in people being enrolled who are not necessarily eligible based on their current circumstances. Federal Medicaid spending increased with rising enrollment during the pandemic, but enhanced federal matching payments to states stabilized state Medicaid costs despite large gains in enrollment.
In addition, streamlining renewal policies and procedures, particularly increasing ex parte or automated renewal rates, can improve coverage retention, but eligibility system capacity and functionality also plays a role.
And, finally, having timely and reliable data on renewal outcomes and enrollment enables closer monitoring of state Medicaid programs to identify problems but also to inform the strategies and flexibilities that can help states improve their processes. In May, CMS extended monthly reporting of renewal outcomes data required during the unwinding period to allow for continued monitoring of state programs.
Renewal Outcomes During the Unwinding
At the end of the unwinding of the Medicaid continuous enrollment provision in most states, over 56 million people had their coverage renewed and over 25 million people have been disenrolled (Figure 1). Although some cases remain pending across states, the overall disenrollment rate during the unwinding was 31%. This rate is somewhat higher than KFF and other groups had estimated before the unwinding began and contributed to more people being disenrolled during the unwinding than had been predicted. Among those who were disenrolled, 69% were terminated for paperwork or procedural reasons. Despite efforts by states to reduce the procedural disenrollment rate by conducting additional outreach or pausing disenrollments altogether, the rate remained high throughout the unwinding. In a more positive development, among those who retained coverage, over six in ten (61%) were renewed through ex parte, or automated processes. These automated renewals reduce the paperwork burden on both enrollees and state workers and make it easier for eligible individuals to retain coverage.
There is significant variation in renewal outcome metrics across states (Figure 1). For example, five states—Montana, Utah, Idaho, Oklahoma, and Texas—have disenrollment rates over 50%, with Montana the highest at 57%, while five states—North Carolina, Maine, Oregon, California, and Connecticut—have disenrollment rates under 20%. The differences result from a variety of factors, including state renewal policies and procedures, system capacity, and the extent to which states adopted flexibilities designed to maintain coverage for eligible enrollees. The share of renewals completed on an ex parte basis may also play a role. The ex parte renewal rates range from a high of 90% or more in Arizona, North Carolina, and Rhode Island to a low of 11% or less in Pennsylvania and Texas.
National Medicaid Enrollment Trends
As of May 2024, 81 million people were enrolled in Medicaid, an increase of about 10 million compared to pre-pandemic enrollment (Figure 2). During the pandemic, Medicaid enrollment increased by 32% or 23 million people. Since the start of the unwinding, enrollment has dropped by about 13 million, wiping out over half of the pandemic-era enrollment gains. As a result, enrollment remains about 13% higher than it was before the start of the pandemic.
Adult enrollment in Medicaid/CHIP remains well above pre-pandemic enrollment; however, enrollment among children has nearly returned to pre-pandemic levels. While adult enrollment is still over 20% above enrollment in February 2020, child enrollment is only about 5% higher. Adults experienced much higher enrollment growth during the pandemic than children. From February 2020 to April 2023, enrollment among adults grew by 45% while child enrollment increased by a more modest 20%. With the downturn in the economy in the early months of the pandemic, more adults enrolled in Medicaid and then were not disenrolled even if their circumstances subsequently changed. Additionally, several states adopted Medicaid expansion, increasing eligibility for adults, either just before or during the pandemic, including Utah and Nebraska in 2020, Missouri and Oklahoma in 2021, and North Carolina and South Dakota in 2023. Although the rate of enrollment decline has been steeper for adults during the unwinding period compared to children, enrollment gains for adults remain higher than those for children.
Medicaid Enrollment Trends Across States
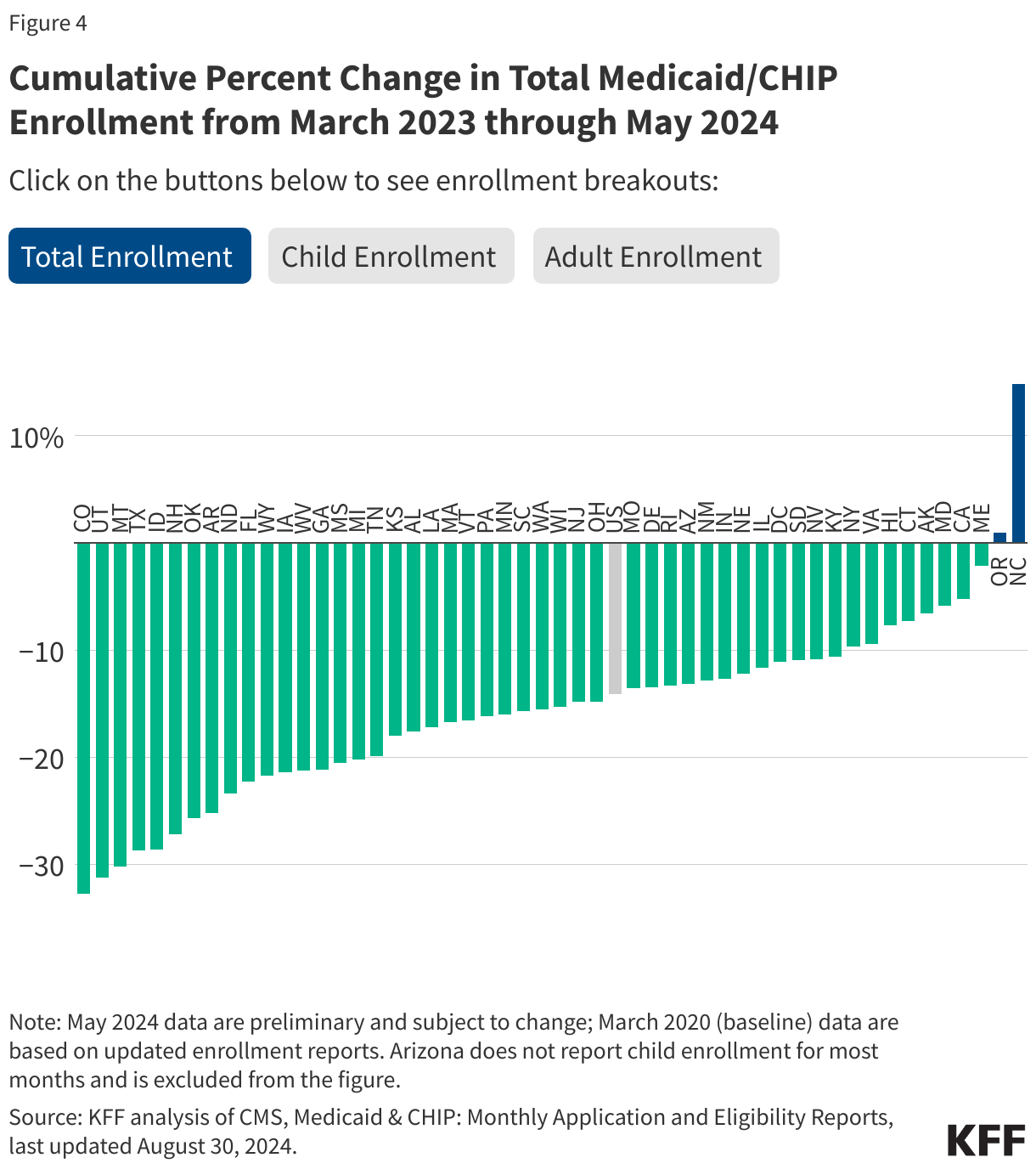
During the unwinding, Medicaid/CHIP enrollment declined in all but two states—North Carolina and Oregon (Figure 4). While enrollment dropped about 14% nationally from March 2023 to May 2024, across states where enrollment declined, the drop varied widely from 2% in Maine to over 30% in Montana, Utah and Colorado. In most states, the net decrease in enrollment was higher for adults than children, but, in general, states with the largest net decline in enrollment for adults also experienced the largest net decline in child enrollment.
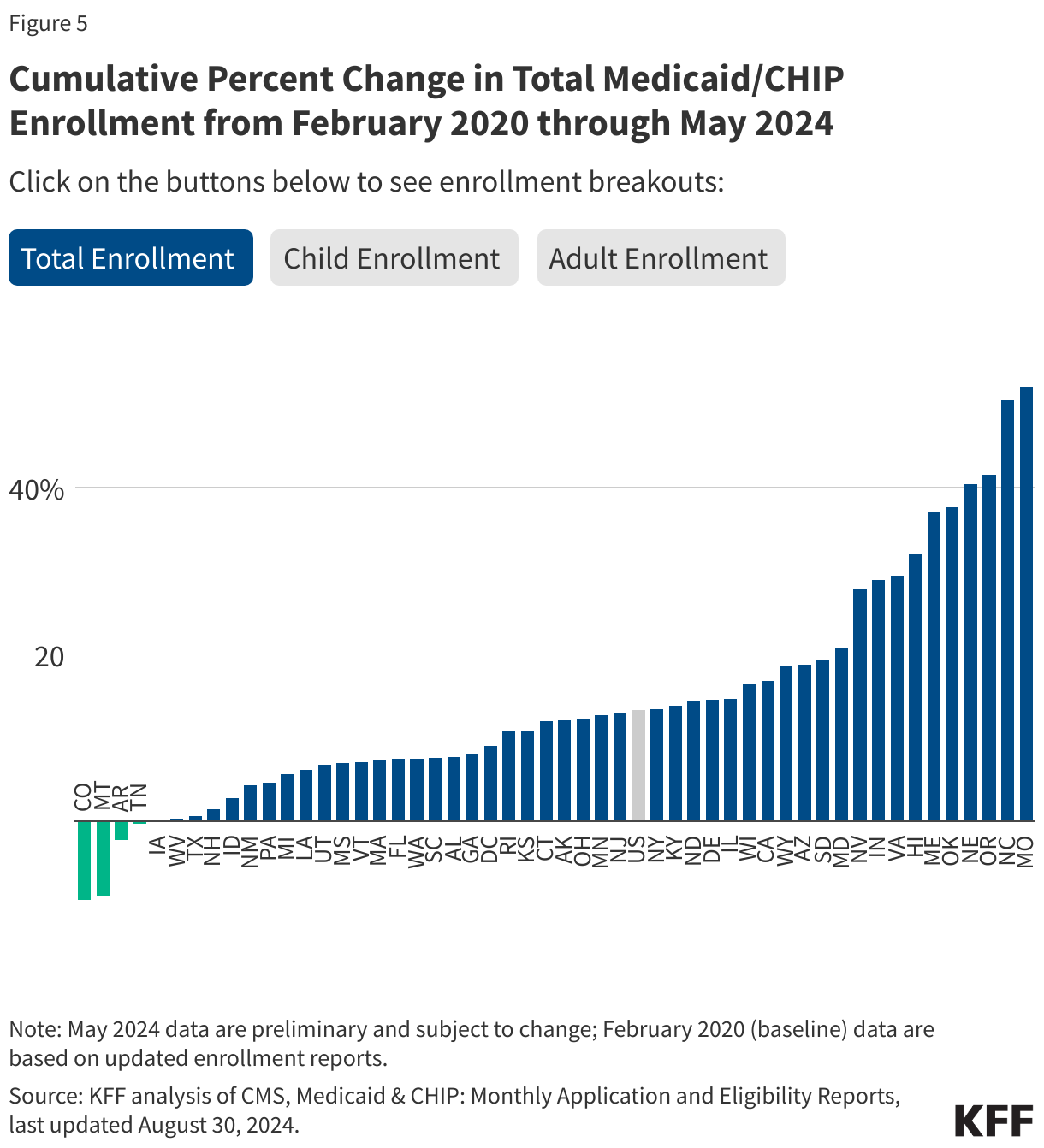
Compared to pre-pandemic levels, total Medicaid/CHIP enrollment remains higher in all but four states, and in seven states enrollment is 30% or more higher (Figure 5). Enrollment has dropped below pre-pandemic levels by 10% in Colorado, 9% in Montana, 2% in Arkansas, less than 1% in Tennessee, and remains essentially flat in Iowa. In these states, relatively moderate enrollment growth during the pandemic was offset by high disenrollment rates during the unwinding, though it is unclear what factors drove the higher disenrollment rates. In contrast, enrollment is 52% higher in Missouri and 50% higher in North Carolina. Among the ten states with the largest net increase in enrollment from February 2020 to May 2024, the increase has been driven by eligibility expansions during the unwinding in five of the states—the adoption of Medicaid expansion in Missouri, Nebraska, North Carolina, and Oklahoma, and a large increase in the eligibility level for children in Maine. The remaining five states—Hawaii, Indiana, Nevada, Oregon, and Virginia—all experienced large enrollment increases during the pandemic and retained much of the increased enrollment through the unwinding.
Children’s enrollment is below the pre-pandemic levels in 12 states as of May 2024, while adult enrollment is below pre-pandemic levels in four states. Enrollment in Medicaid/CHIP among children is down over 14% in Montana, between 6% and 10% in Colorado, Idaho, and Utah, and 3% or less in the remaining eight states. Enrollment is below pre-pandemic levels for both children and adults in Montana, Colorado, and Arkansas. In Tennessee, adult enrollment dropped below pre-pandemic enrollment, but child enrollment is slightly above the earlier level. Generally, it was expected that a greater share of children than adults would remain eligible and enrolled. However, the drop in child enrollment below pre-pandemic levels in so many states coupled with an increase in the child uninsured rate in 2023 suggests that that some children may have lost coverage despite still being eligible.