5 Key Facts About Medicaid Expansion
Congress has passed a budget resolution that targets up to $880 billion or more in federal spending cuts from Medicaid over ten years. While specific proposals are not yet known, policies under discussion could limit financing and coverage for the Affordable Care Act (ACA) expansion group. Recent KFF polling shows there is little support for cuts to federal Medicaid spending overall, and a majority of adults (59%) oppose eliminating the enhanced federal match rate for adults covered under Medicaid expansion specifically.
The ACA expanded Medicaid coverage to nearly all adults with incomes up to 138% of the Federal Poverty Level ($21,597 for an individual in 2025) and provided states with an enhanced federal matching rate (FMAP) of 90% for their expansion populations over time, which is greater than the matching rate for Medicaid generally. While federal funding finances 90% of spending on the expansion population, states are responsible for the remaining 10% of costs for enrollees eligible under Medicaid expansion. As a result of a Supreme Court ruling in 2012, the expansion is effectively optional for states, and as of April 2025, all but 10 states have adopted the expansion. While expansion has led to higher government spending on Medicaid, a large body of literature shows that it is linked to reduced rates of uninsurance, increased health care affordability, improvements in access and health and outcomes, and economic benefits for states and providers. KFF polling shows that of people living in non-expansion states, two-thirds (66%) said their state should expand Medicaid to cover more low-income uninsured people.
This issue brief examines Medicaid expansion enrollment and Medicaid spending in expansion and non-expansion states and describes the characteristics of adults covered by the Medicaid expansion.
1. Medicaid expansion is widely adopted by both red and blue states.
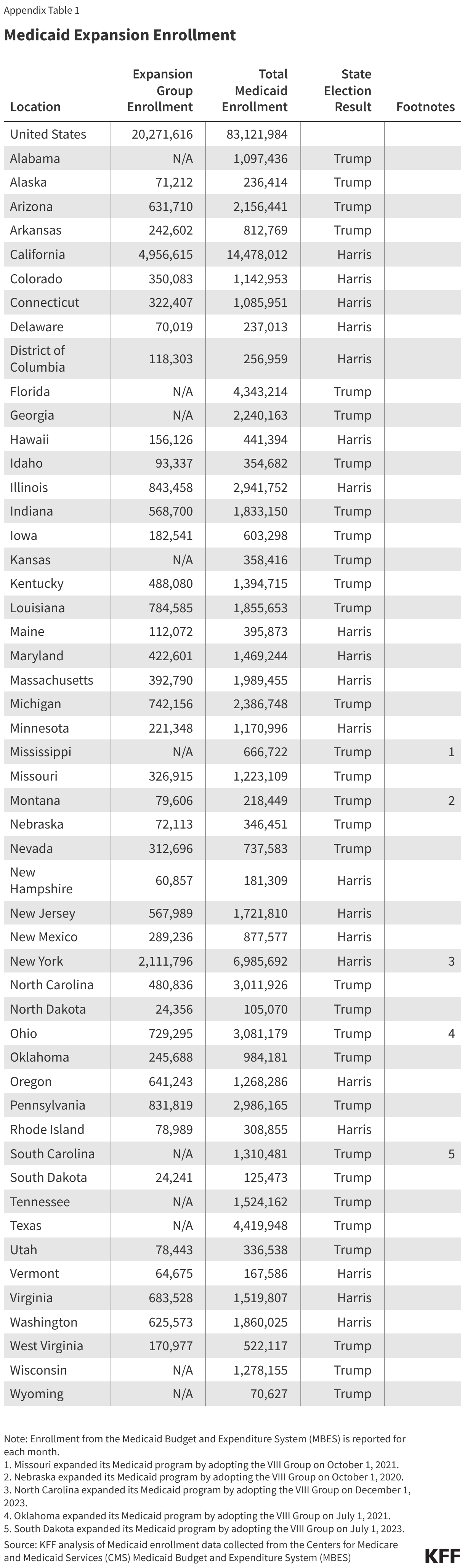
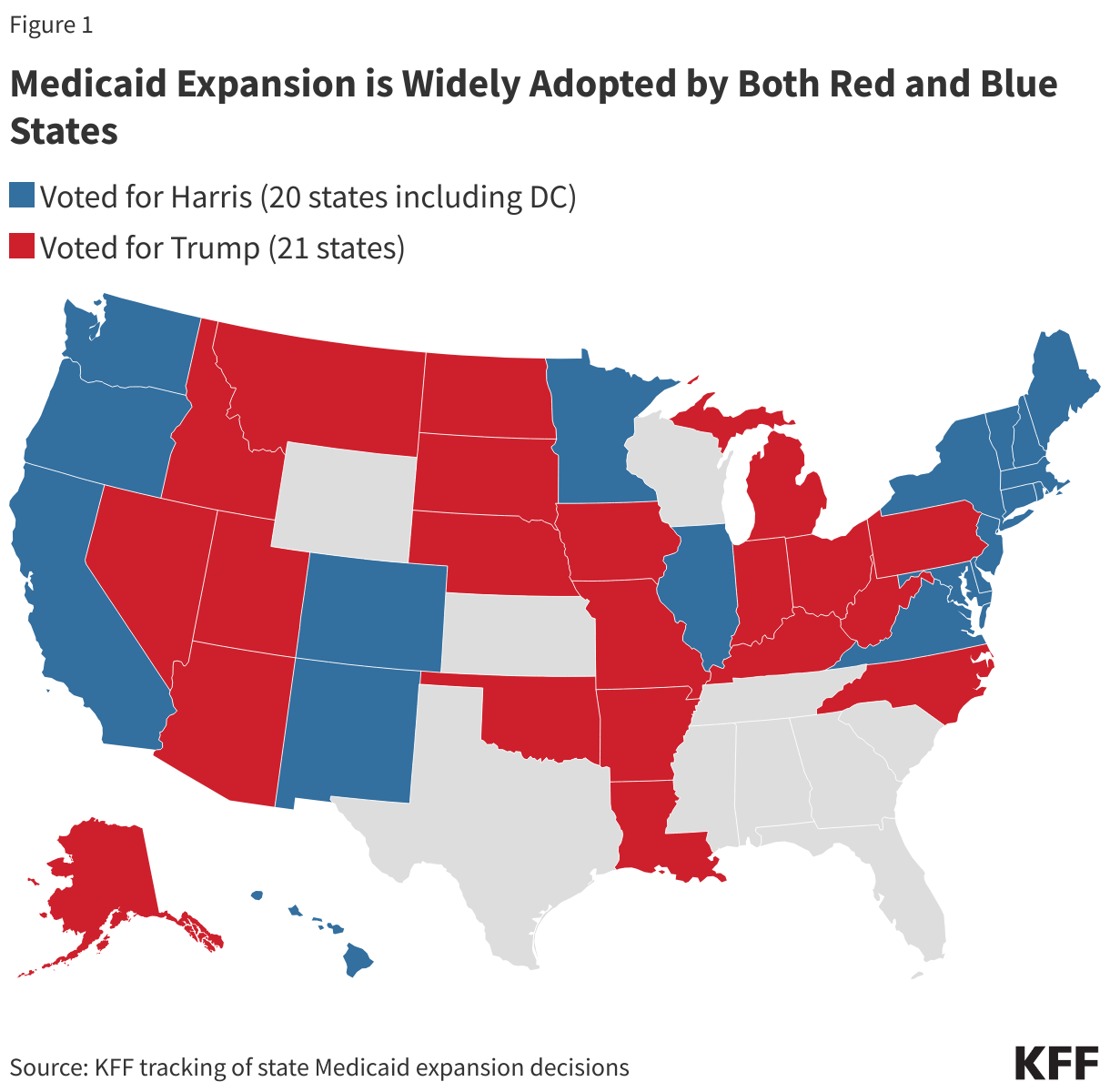
Over the past 11 years, Medicaid expansion has been broadly adopted. The 41 states including the District of Columbia that have adopted Medicaid expansion are split nearly evenly between states that voted for Trump (21 states) and those that voted for Harris (20 states) in the 2024 Presidential election (Figure 1). Over half (27) of states adopted Medicaid expansion in 2014, while 14 states have implemented expansion since 2014, with South Dakota and North Carolina adopting most recently in 2023. Most states adopted expansion through legislation; however, in seven states, the expansion was adopted via a ballot measure. As of June 2024, over 20 million people were enrolled through Medicaid expansion, representing nearly a quarter of total Medicaid enrollment across all states and 31% of total enrollment in expansion states.
Medicaid expansion is linked to gains in coverage, access, increased health care affordability, and economic benefits for states and providers. Although establishing direct causality between health insurance and health outcomes is complex, evidence generally shows Medicaid expansion is associated with improved health outcomes, including increased early-stage cancer diagnosis, improved disease management, and lower mortality rates for many chronic conditions.
2. Medicaid median income eligibility for children, pregnancy, and parents, and Medicaid spending per enrollee are higher in expansion states compared to non-expansion states.
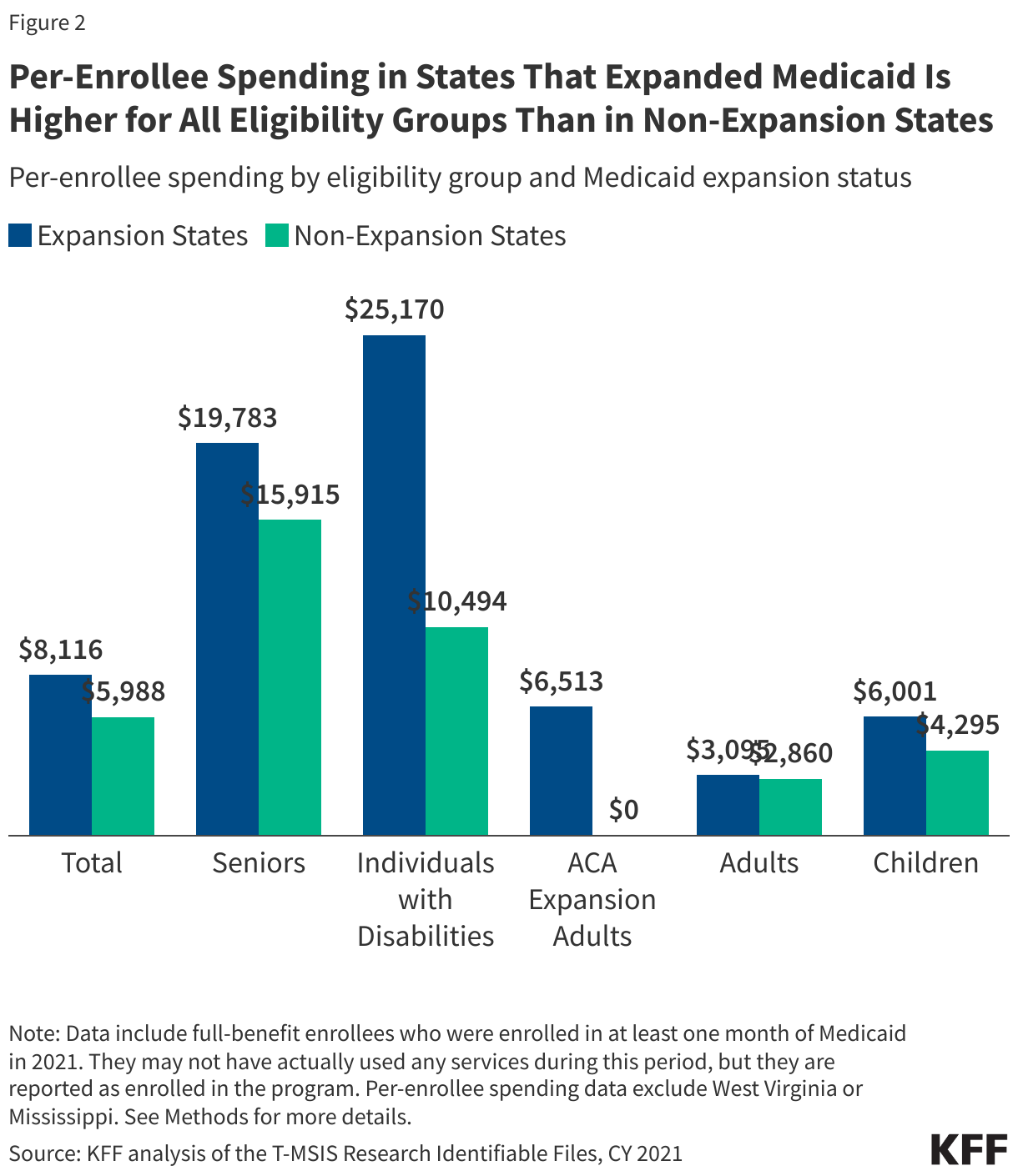
Overall, per enrollee spending for the expansion group was higher than for other adults and children but well below per enrollee spending for enrollees over age 65 and people with disabilities. While some critics of Medicaid expansion have argued that expansion diverts resources away from other groups of Medicaid enrollees, including people with disabilities and children, data show that expansion states spend more per enrollee overall and on each eligibility group than non-expansion states. Per enrollee spending for people with disabilities in expansion states is nearly 2.5 times the spending in non-expansion states ($25,170 per enrollee vs. $10,494) (Figure 2). The difference in per-enrollee spending for expansion and non-expansion states holds true for more detailed eligibility pathways for people based on age or disability. Expansion states also spent nearly $2,000 more per child enrollee than non-expansion states ($6,001 vs $4,295). The differences in per enrollee spending may reflect state policy choices about benefits and eligibility, in addition to payment rates, regional variation in health care costs, and state demographics.
In addition to difference in spending, expansion states have higher median income-based eligibility limits compared to non-expansion states for children (266% FPL in expansion states compared to 234% in non-expansion states), pregnant individuals (213% FPL compared to 203% FPL), and parents (138% FPL compared to 33% FPL). There is substantial variation in adoption of optional eligibility and other policies for seniors and people with disabilities, with state expansion status not a strong predictor of these policy choices.
3. Nearly four in ten women of reproductive age and over six in ten 50-64 year olds enrolled in Medicaid are covered through Medicaid expansion.
Medicaid expansion provides coverage across age groups for those 19 to 64 (Figure 3). Many expansion adults are working; however, they work for employers and in industries that are less likely to offer health insurance, leaving them without affordable health coverage options. As discussed below, older enrollees are more likely to have chronic conditions and may face more barriers to work.
Medicaid expansion also provides an important eligibility pathway for women of reproductive age, covering 38% of women ages 19-49 enrolled in Medicaid. For those who become pregnant, Medicaid coverage prior to pregnancy can promote pre-pregnancy health care, which can lead to healthier pregnancies and help reduce the risk of complications. Previous KFF analyses show that in expansion states, pregnant individuals are more than twice as likely to be enrolled in Medicaid prior to pregnancy (59%) than in non-expansion states (26%) (the difference in income eligibility levels for pregnant adults vs. other adults is large in non-expansion states, explaining the difference in pre-pregnancy enrollment rates). Medicaid expansion can provide stable coverage to pregnant individuals after the postpartum coverage period ends. Medicaid expansion coverage of parents also increases enrollment of their children: evidence shows that if children are eligible for Medicaid or CHIP coverage but unenrolled, when their parents gain coverage through Medicaid expansion it has a spillover, or “welcome mat” effect, increasing the number of children who enroll in health coverage. Medicaid expansion also covers adults as they age – more than six in ten Medicaid enrollees ages 50-64 are covered through expansion – and before they become eligible for Medicare.

4. One third of Medicaid expansion enrollees have a chronic physical health condition and a quarter have a chronic behavioral health condition.
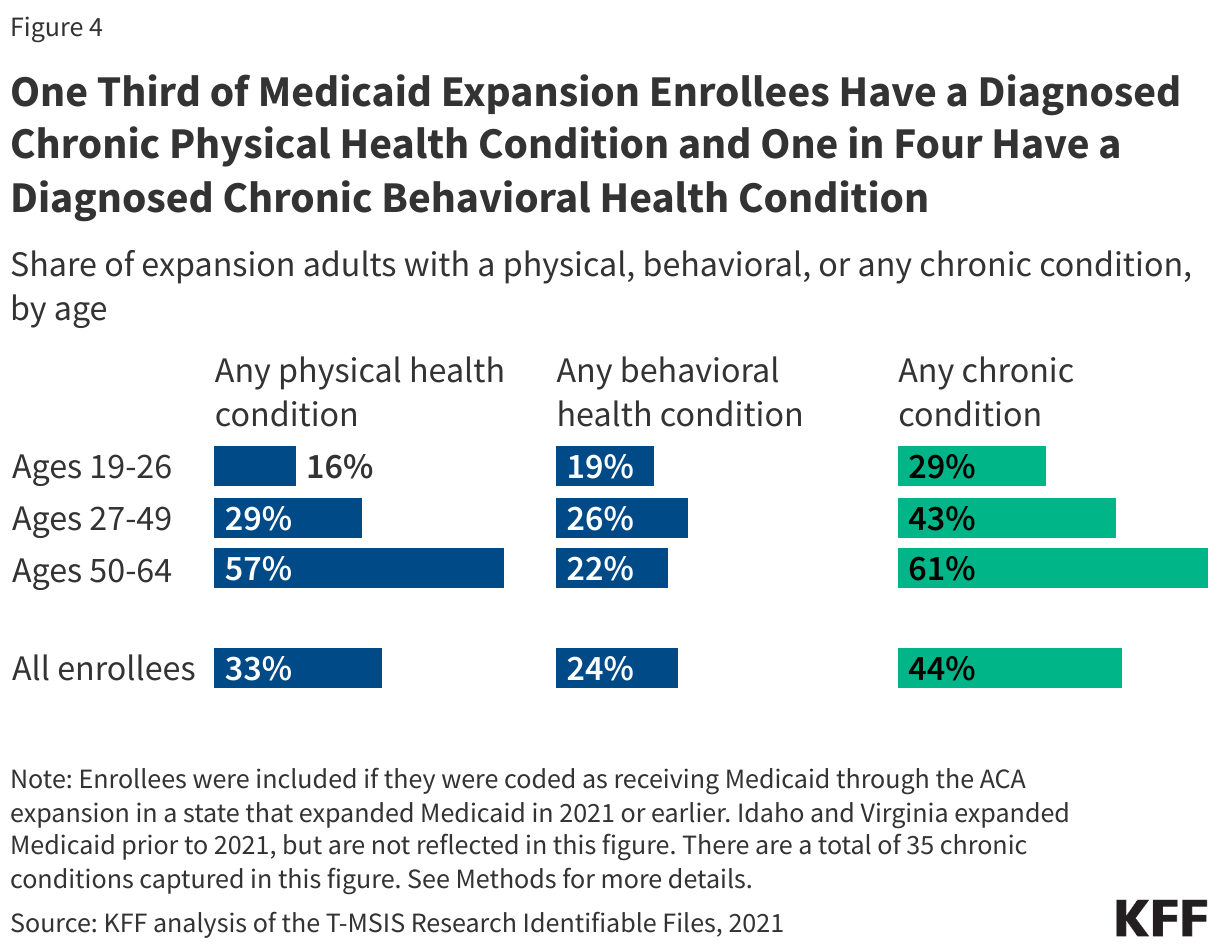
Nearly half (44%) of expansion adults have at least one chronic condition, including 33% that have a chronic physical condition and 24% that have a behavioral health condition. Of Medicaid enrollees with at least one chronic condition, 53% are enrolled through Medicaid expansion (data not shown). Similar to all adults on Medicaid, the share of expansion adults with at least one chronic physical condition increases with age (Figure 4). Nearly six in ten (57%) expansion adults ages 50-64 have at least one physical health condition compared to just 16% of expansion adults ages 19-26. While the share of expansion adults with physical health conditions increases with age, the share with behavioral health conditions remains relatively stable, ranging from 19% to 26% across age groups.
Research finds that expansion is associated with improved access to care and outcomes related to behavioral health conditions. For other chronic conditions, expansion has positive impacts on access to care and may improve certain health outcomes. Medicaid coverage helps expansion enrollees manage chronic conditions and supports workforce participation. Medicaid expansion also provides coverage to individuals who have chronic conditions or disabilities that may limit their ability to work. Although some people with disabilities qualify for Medicaid because they receive Supplemental Security Income, most are eligible for Medicaid through other pathways, including the expansion group. While many adults who need long-term care may qualify for coverage through other Medicaid pathways, Medicaid expansion covers some individuals with costly health needs who may otherwise be unable to afford care; two percent (2%) of expansion enrollees, or 395,000 individuals, use long-term care services (LTC) which support activities of daily living such as eating, bathing, or dressing (data not shown). Medicaid expansion is also the primary pathway for Medicaid coverage for people with HIV.
5. Policy changes targeting Medicaid expansion would reduce government spending but also could put coverage for 20 million enrollees at risk.
There are several options under consideration in Congress to reduce federal Medicaid spending that could have implications for enrollees in the expansion group, including work requirements and changes in financing for the expansion. Congress may debate federal legislation requiring states to impose work requirements as a condition of Medicaid coverage. Most adult Medicaid enrollees are already working without a work requirement; estimates of national work requirements show $109 billion in federal savings over 10 years, and an increase in the number of uninsured, but no increase in employment. Beyond legislative changes, a number of states are pursing waivers to condition Medicaid expansion coverage on meeting work requirements since work requirement waivers were encouraged and approved during the first Trump administration.
Congress may also consider proposals that would alter the financing for the Medicaid expansion. Any approach to reduce federal Medicaid spending for the expansion would shift costs to states, forcing governors to make tough choices about whether to drop the ACA Medicaid expansion, provide alternative coverage options or make up the loss of federal funding by cutting other state programs or raising taxes. Twelve states have “trigger” laws in place that would automatically end expansion or require other changes if the share of federal funding drops below 90%, and two additional states, Ohio and South Dakota, are considering similar action. But all states, including those without trigger laws in place, would examine their ability to maintain the ACA Medicaid expansion if Medicaid expansion financing was altered. An analysis of the impact on Medicaid enrollment if all states eliminated the expansion shows the decline in enrollment would vary across states, ranging from 19% in Massachusetts, Minnesota, North Carolina, and South Dakota to 49% in Oregon (Figure 5).

If states eliminate the Medicaid expansion, individuals with incomes 100-138% FPL would be eligible for subsidies in the Marketplace, but could face barriers transitioning to Marketplace coverage and could face higher out of pocket costs, especially if the enhanced subsidies expire at the end of 2025. However, current Medicaid expansion enrollees with incomes below 100% FPL are not eligible for subsidies in the Marketplace and could fall into the “coverage gap” and become uninsured if they are unable to qualify for Medicaid under a different eligibility pathway, for example based on a disability. Currently, 1.4 million adults are in the coverage gap in the ten non-expansion states; however, that number would likely increase significantly under proposed policy changes targeting the Medicaid expansion. Eliminating the Medicaid expansion could have additional spillover effects, including children whose eligibility status is unchanged but become uninsured after their parents lose Medicaid coverage. People without insurance have more difficulty accessing care and are more likely to have medical debt, with almost one in four uninsured adults in 2023 not receiving needed medical treatment due to cost. Uninsured individuals are also less likely than those with insurance to receive preventive care and treatment for major health conditions and chronic diseases.
Methods |
| Medicaid Claims Data: This analysis uses the 2021 T-MSIS Research Identifiable Demographic-Eligibility and Claims Files (T-MSIS data) to identify Medicaid expansion enrollees, spending, and chronic conditions in Figures 2-4.
State Inclusion Criteria:
Enrollee Inclusion Criteria: Enrollees were included if they were ages 19-64, had full Medicaid coverage for at least one month, and were not dually enrolled in Medicare. Dually enrolled individuals were excluded from these calculations since they may not have had sufficient claims in T-MSIS to identify chronic conditions. Calculating Spending (Figure 2): This figure reflects spending from all states except Idaho, Virginia, West Virginia, and Mississippi. Average annual per capita spending calculations include fee-for-service spending and payments to managed care plans. Spending was calculated by summing the total spending of all claims per enrollee in the T-MSIS claims files. Estimates here do not include prescription drug rebates and most supplemental payments to providers. Defining Chronic Conditions (Figure 4): This figure reflects chronic conditions from all expansion enrollees in expansion states that expanded prior to 2021 except for Idaho and Virginia. This analysis used the CCW algorithm for identifying chronic conditions (updated in 2020). This analysis also included in its definition of chronic conditions substance use disorder, mental health, obesity, HIV, hepatitis C, and intellectual and developmental disabilities. In total, 35 chronic conditions were included and were further grouped into 3 broad categories: behavioral health, physical health, and cognitive impairment conditions. Specific conditions within these groupings include:
|
Appendix