What Do We Know About People with HIV Who Are Not Engaged In Regular HIV Care?
Key Findings
An ongoing challenge to ending the HIV epidemic in the U.S. is reaching people with HIV who are not receiving regular HIV care and are not virally suppressed. Being engaged in HIV care, including being on antiretroviral therapy, promotes optimal individual health outcomes and viral suppression, which in turn prevents transmission of HIV to others. To date, however, robust and representative data on people with HIV who are not receiving regular HIV care have been limited, making it difficult to understand who they are and what barriers they face. This analysis aims to help fill this gap, using nationally representative data to assess the characteristics and experiences of people with HIV who are out of regular HIV care, defined as those who had less than two CD41 . or viral load tests at least 3 months apart within a 12-month period and were not virally suppressed.
Overall, we find that one-in-five (21%) adults with diagnosed HIV were out-of-care and, compared to their in-care counterparts, they were more likely to report challenges in their interactions with the health system, multiple and complex barriers to access, and unmet needs for ancillary care; they are also more likely to be members of population groups already facing longstanding health disparities. Specifically, we find that:
- People with HIV who were out-of-care were more likely to be Black, young, and to report poorer health status than those in-care. They were also more likely to be uninsured, experience changes in their usual source of care related to insurance changes, and were less likely to have a regular provider or to receive support from the Ryan White Program. There were no statistically significant differences based on state Medicaid expansion status or census region.
- Those out-of-care were more likely to report barriers to care engagement, including in the areas of finances, mental health, and getting to a doctor’s office, as well as more dissatisfaction with care than those in-care. They were also more likely to report unmet needs for ancillary social and support services in three domains: clinical, non-HIV medical/behavioral, and subsistence services, with more than half reporting at least one unmet need.
- Whereas virtually all people with HIV in-care were on antiretroviral therapy, a fifth of those out-of- care were not on ARVs, and among those who were, they were more likely to report missing treatment doses. In addition, smaller shares reported being familiar with the concept of treatment as prevention (TasP) than those in-care, though there were substantial knowledge gaps for both groups.
- Identifying people with HIV who are out-of-care, and better understanding the barriers they face, are first steps towards engaging or reengaging them in-care, addressing their unmet needs, and improving their health status. Doing so could play a role in advancing the goals in the national HIV/AIDS Strategy and the federal Ending the HIV initiative.
Introduction
An ongoing challenge to ending the HIV epidemic in the U.S. is reaching people living with HIV who are out of regular HIV care and not virally suppressed. Being engaged in HIV care, including being on antiretroviral therapy, promotes optimal individual health outcomes and viral suppression, which also prevents transmission of HIV. Indeed, an estimated 43% of HIV transmissions are estimated to result from people who were aware of their HIV status but not engaged in care. To date, however, robust and representative data on people with HIV who are not engaged in regular HIV care and the barriers they face have been limited. One exception is a nationally representative analysis that assessed barriers to care faced by people with HIV who felt they had not received enough care. The current analysis aims to add to this knowledge base, using nationally representative data from the Centers for Disease Control and Prevention’s Medical Monitoring Project (MMP). The MMP is a cross-sectional, nationally representative survey of adults with diagnosed HIV in the United States and includes data drawn from both in-depth interviews and medical record abstraction.
For this analysis, we defined people with HIV as not being in care if they (1) had less than two CD4 or viral load tests at least 3 months apart within a 12-month period and (2) did not have sustained viral suppression (see box). This definition differs from the one used by the Centers for Disease Control and Prevention which only focuses on lab testing frequency regardless of viral suppression status.2 By taking this approach, we aimed to identify the most vulnerable individuals within this group, including those who may have the greatest need for targeted engagement efforts. The analysis is limited to adults and is based on data collected between 2018 and 2020 (see Methodology for details).
| Table 1: Key Terms | |
| Term | Definition |
| Out-of-care | Received fewer than two CD4 or viral load tests at least 3 months apart within a 12-month period AND had any viral load test where they were virally unsuppressed in the preceding 12 months. |
| In-care | Received two or more CD4 or viral load tests at least 3 months apart within a 12-month period OR was virally suppressed at all tests in the preceding 12 months (regardless of lab test frequency). |
| Sustained viral suppression | No unsuppressed viral load test results in the preceding 12 months |
Findings
Population
Based on the definition described above, 21% of adults with diagnosed HIV were out-of-care during the 2018 to 2020 period. This group was not virally suppressed and had a suboptimal number of recommended lab tests. The remaining 79%, who serve as our comparison group (i.e. those “in-care”), include all those virally suppressed, regardless of the number of lab tests they have received, and others with regular CD4 or viral load labs.
Demographics
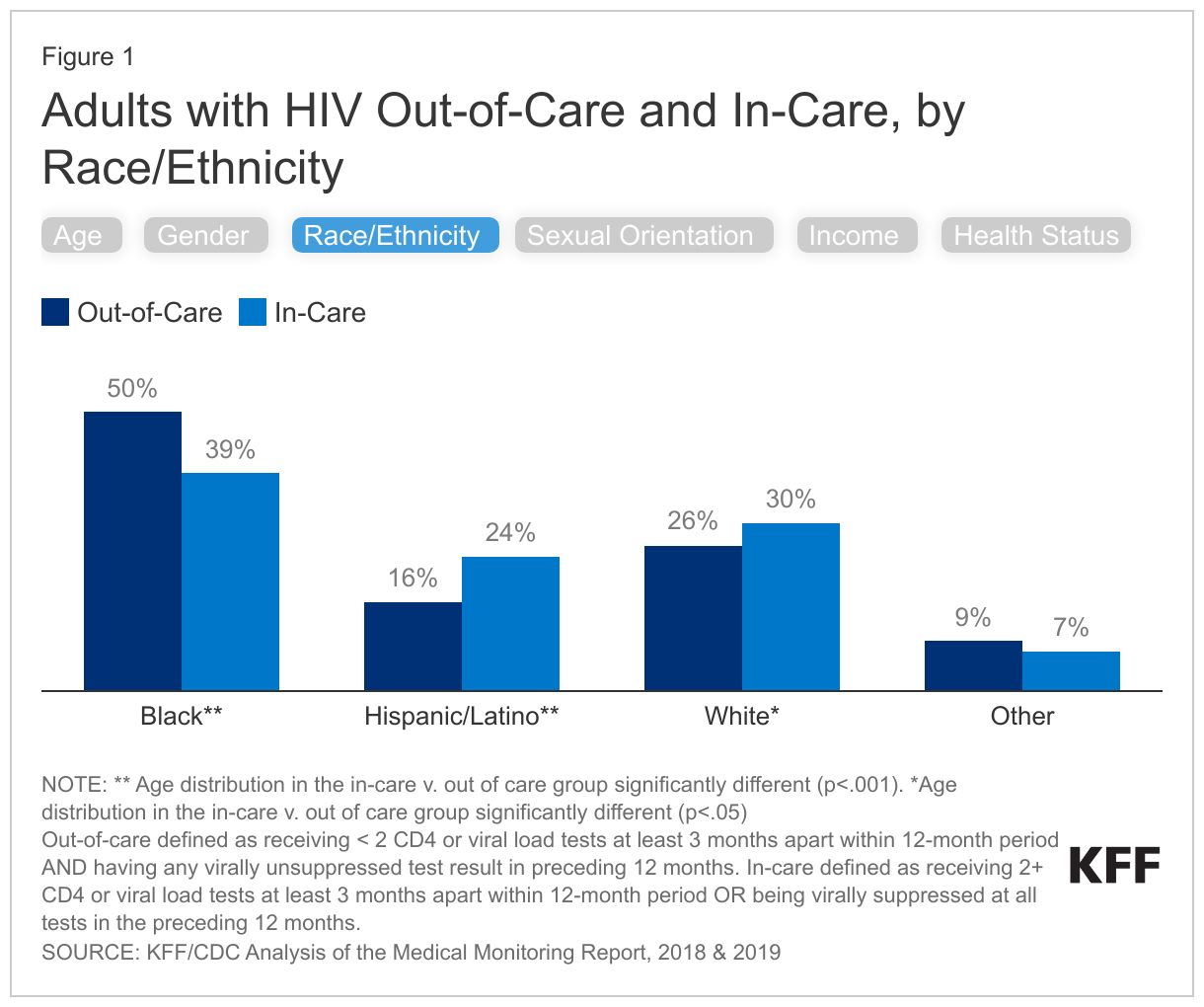
People with HIV who were out-of-care differed demographically from those in-care. They were more likely to be Black, younger, and to report poorer self-rated physical health, among other differences (see Figure 1).
- People with HIV who were out-of-care were more likely to be Black (50% of those out of care v. 39% of those in care) and less likely to be Hispanic/Latino (16% v. 24%) or White (26% v. 30%) than those in-care.
- They were also younger than their in-care counterparts, with greater shares between the ages of 18-29 (12% v. 8%) and 30-39 (20% v. 16%). This finding echoes other data demonstrating lower levels of care engagement among younger people in across certain measures.
- In addition, they were more likely to report “fair or poor” health (35% v. 27%) and less likely to report “excellent or very good” health (28% v. 37%) than those in-care.
- Finally, compared to those in-care, they were somewhat less likely to identify as gay or lesbian (37% v. 42%), have incomes above 400% FPL (9% v. 12%), or be male (72% v. 75%), but there were no other differences in other sexual orientation, poverty, or gender categories.
- There were no statistically significant differences based on state Medicaid expansion status or census region.
Health Coverage and Ryan White Support
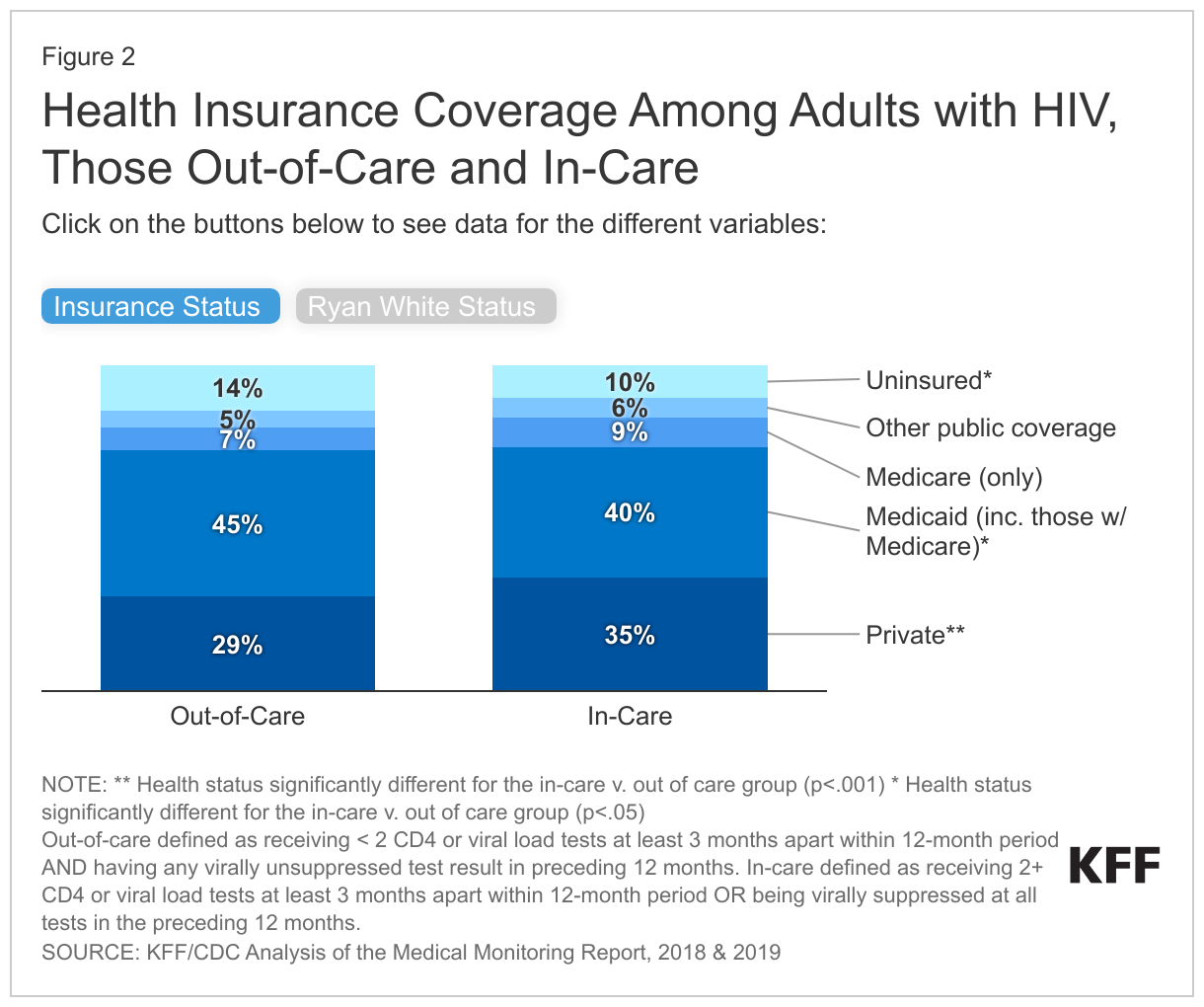
People with HIV who were out-of-care were more likely to be uninsured and less likely to have private insurance than those in-care, but also less likely to receive Ryan White support (see Figure 2).
- People with HIV who were out-of-care were more likely to be uninsured (14% v. 10%) or have Medicaid (45% v. 40%) than those in-care, and less likely to have private coverage (29% v. 35%).
- While both groups were similarly likely to report changes to their insurance coverage over the past 12-month period (14% v. 13%), those out-of-care were twice as likely to say this led to a change in their usual source of HIV care (40% v. 19%).
- Finally, compared to their in-care counterparts, those who were out-of-care had significantly lower levels of support from the Ryan White HIV/AIDS Program (39% v. 50%), the nation’s HIV safety-net program that provides outpatient HIV care, treatment, and support services to people with HIV who were underinsured and uninsured.
Accessing care
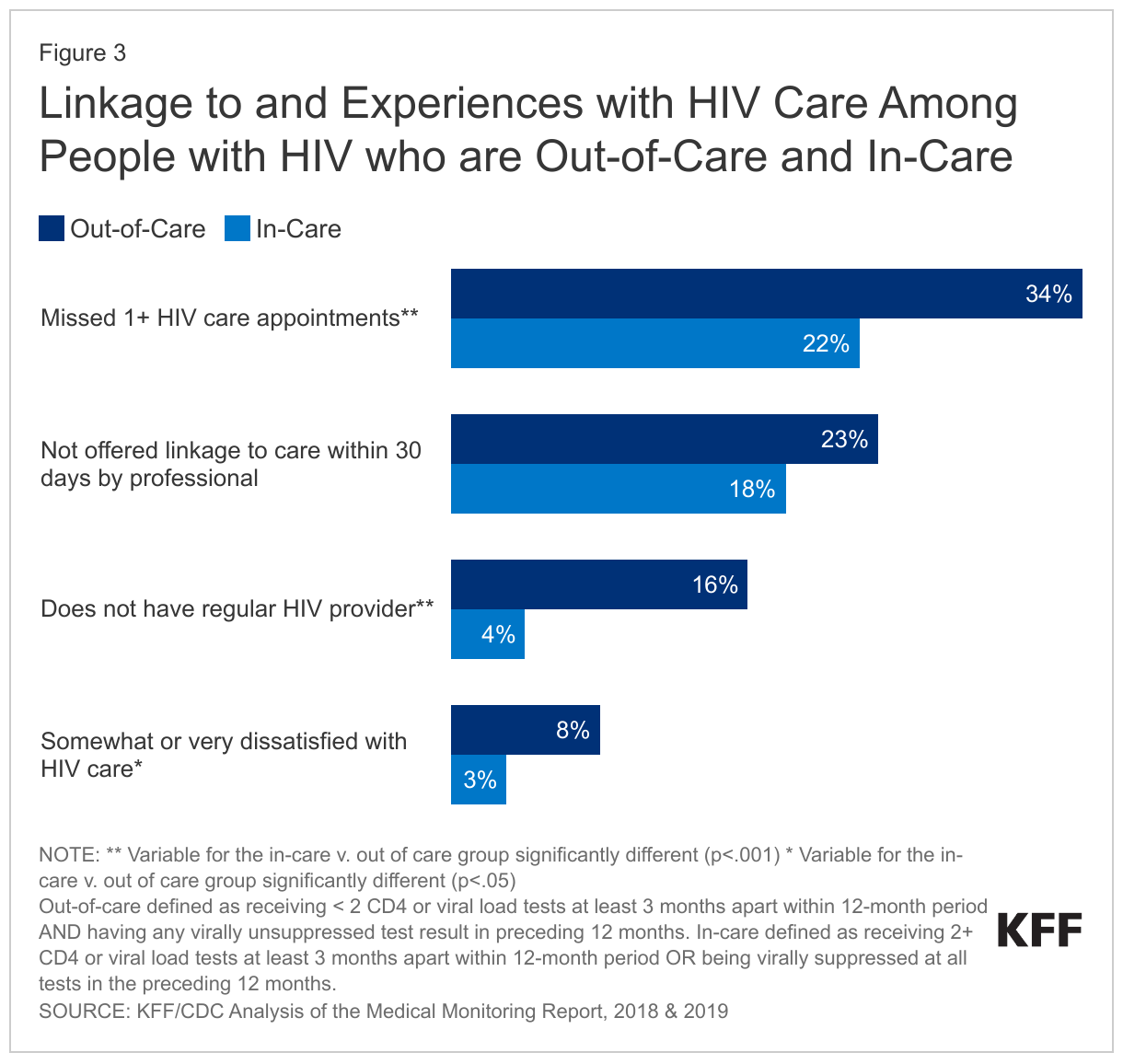
People with HIV who were out-of-care care were less likely to have a regular provider, more likely to be dissatisfied with recent care that they had received, and more likely to have missed appointments, than those in-care.
- While similar shares reported they were not offered assistance in finding HIV care within 30 days of diagnosis by a professional (23% v. 18%), those who were out-of-care were about four times as likely to report not having a regular HIV provider (16% v. 4%).
- In addition, about one-third (34%) of those out-of-care reported missing one or more HIV care appointments in the 12 months prior to the interview compared to one-in-five of those in care (22%).
- They were also more likely to report being “very or somewhat” dissatisfied with the HIV care they received over the preceding 12 months (8% v. 3%).
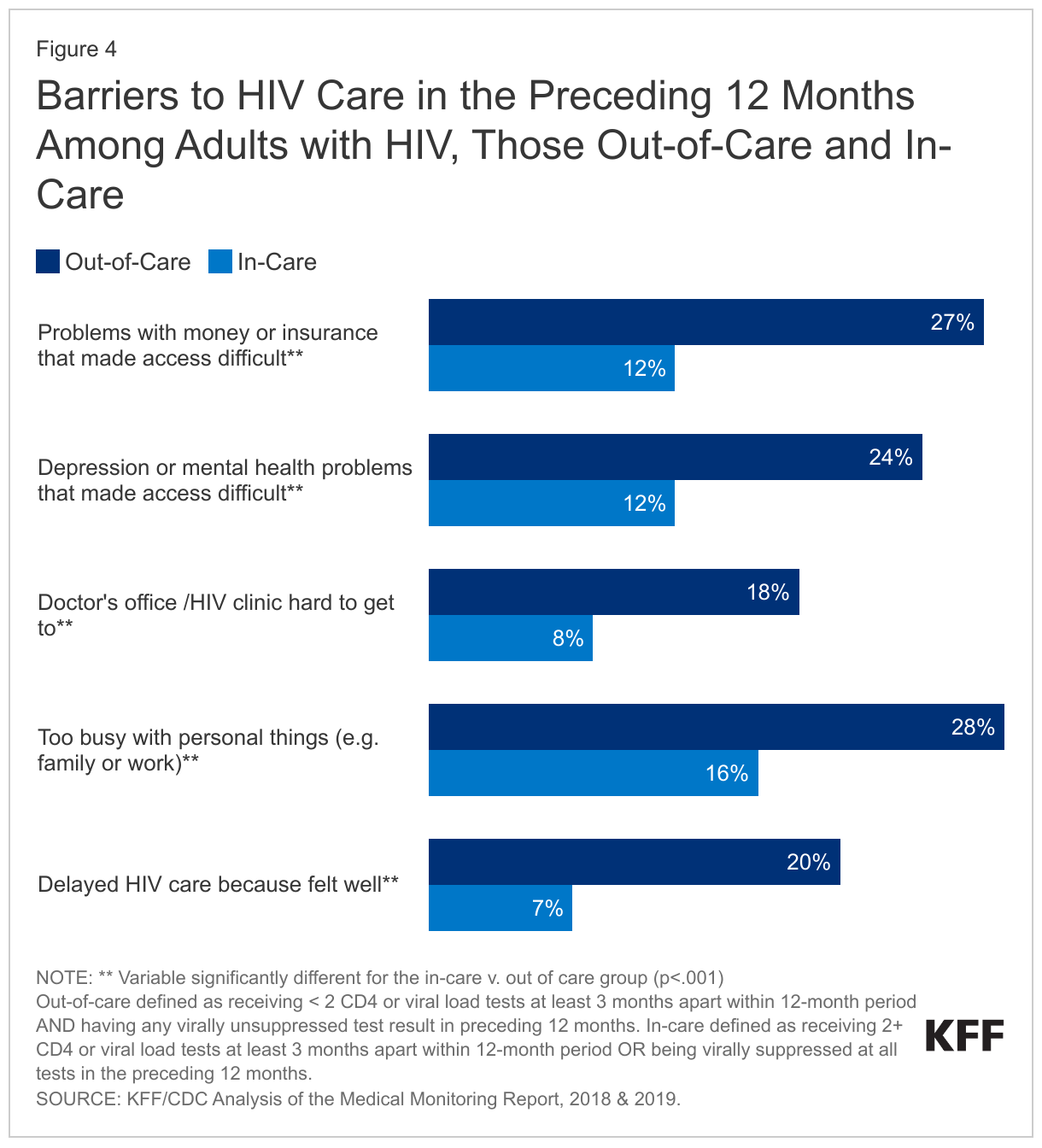
People with HIV who were out-of-care were also more likely to report certain barriers to care engagement, including in the areas of finances, mental health, and getting to a doctor’s office than those in-care.
- Over one-quarter of those reported that problems with money or insurance were barriers to HIV care, compared to just over one-in-ten of those in-care (27% v. 12%). Those out-of-care were also more likely to report facing problems paying medical bills (data not shown).
- In addition, they were twice as likely to report that depression or other mental health problems made it difficult to get HIV care (24% v. 12%), and were more likely to say that personal issues, such as family or work, were barriers to care (28% v 16%).
- About one-in-five (18%) reported that difficulty getting to a doctor’s office was a barrier to HIV care, more than double the share of those in care (8%).
- While those out-of-care generally reported more barriers to access, they were also more likely to say they delayed care because they felt well, compared to their in-care counterparts (20% v. 7%).
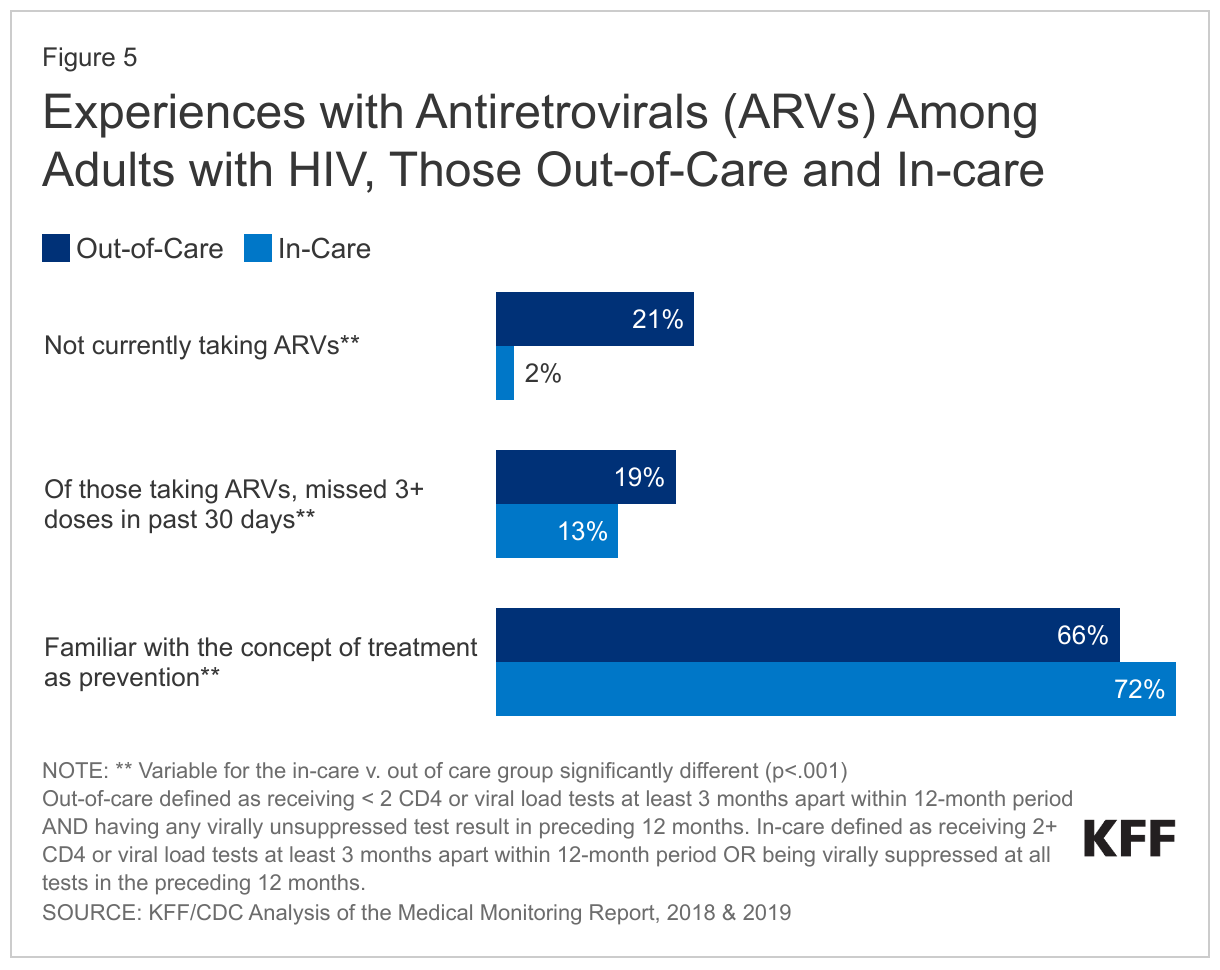
People with HIV who were out-of-care were less likely to report being on antiretroviral therapy, despite the recommendation that such treatment be started as soon as possible after diagnosis, and were more likely to report missing ARV treatment doses.
- One-in-five (21%) of those out-of-care reported they were not currently taking ARVs compared to just 2% of those in-care.
- In addition, of those who did report taking ARVs, 19% reported missing three or more doses in the past 30 days, compared to 13% of those in-care.
- While 66% of those who were out-of-care were familiar with the concept of treatment as prevention (i.e. that when someone is virally suppressed due to consistent ARV use, they cannot transmit HIV), one-third were not. In contrast, nearly three-quarters (72%) of those in-care were familiar with the concept.
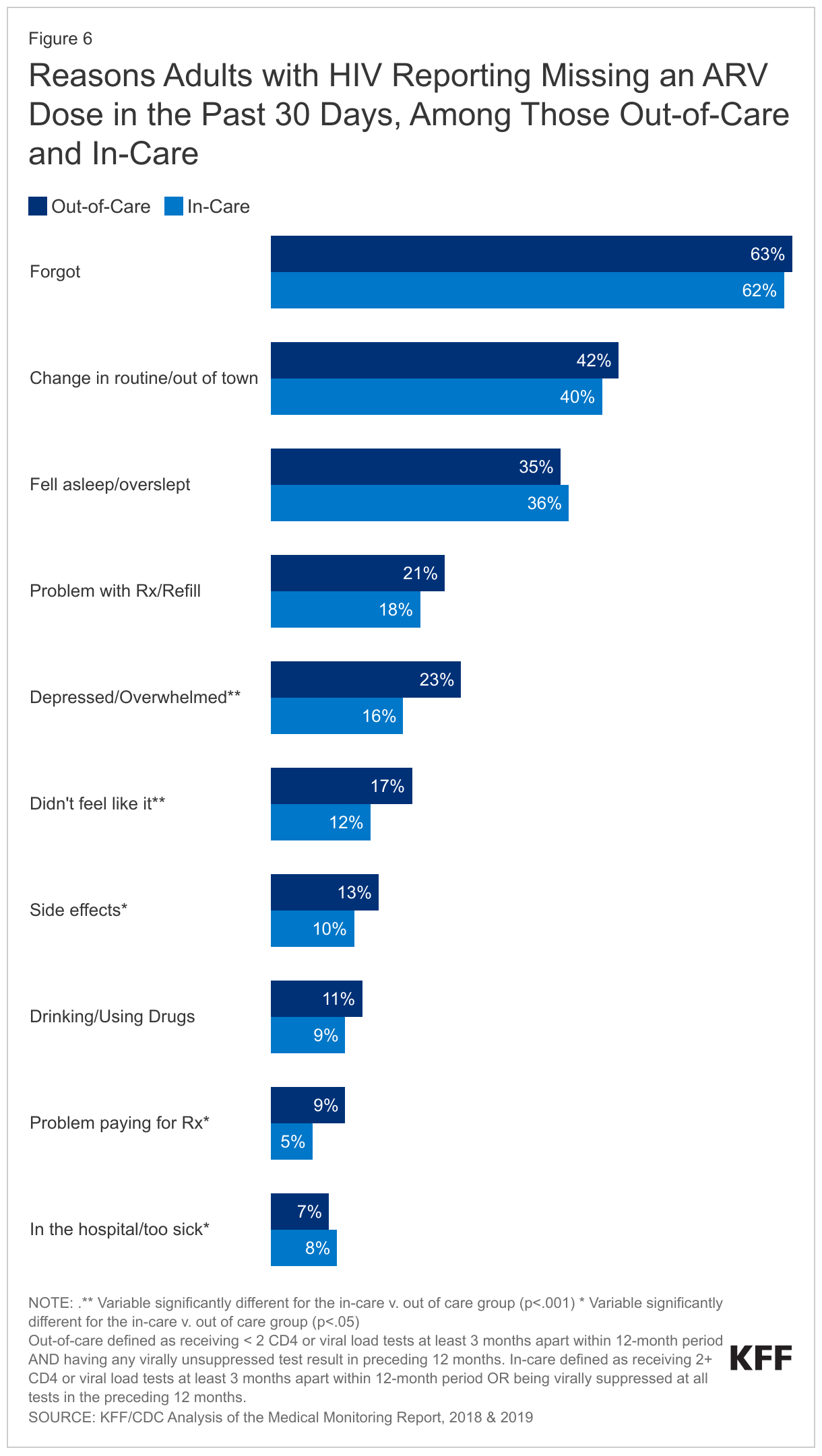
Reasons for missing ARV doses were generally similar between those in and out of care, although there were some exceptions, particularly with respect to mental health challenges.
- For those who were out-of-care, the most common reported reason for missing an ARV dose was forgetting it (63%), followed by a change in daily routine or being out of town (42%), and being asleep (35%). Additionally, about one-in-five reported they had a problem getting a prescription or a refill (21%). Others reported that use of alcohol or drugs (11%) or being too sick or in the hospital (7%) got in the way of taking ARVs. In each case, these were similar to reports from those in-care.
- However, those who were out-of-care were more likely to report the following reasons for not taking ARVs than those in-care: feeling depressed or overwhelmed (23% v. 16%), not feeling like taking the medications (17% v. 12%), , experiencing side effects (13% v. 10%), and having problems paying for the medication (9% v. 5%).
Unmet needs for HIV ancillary services
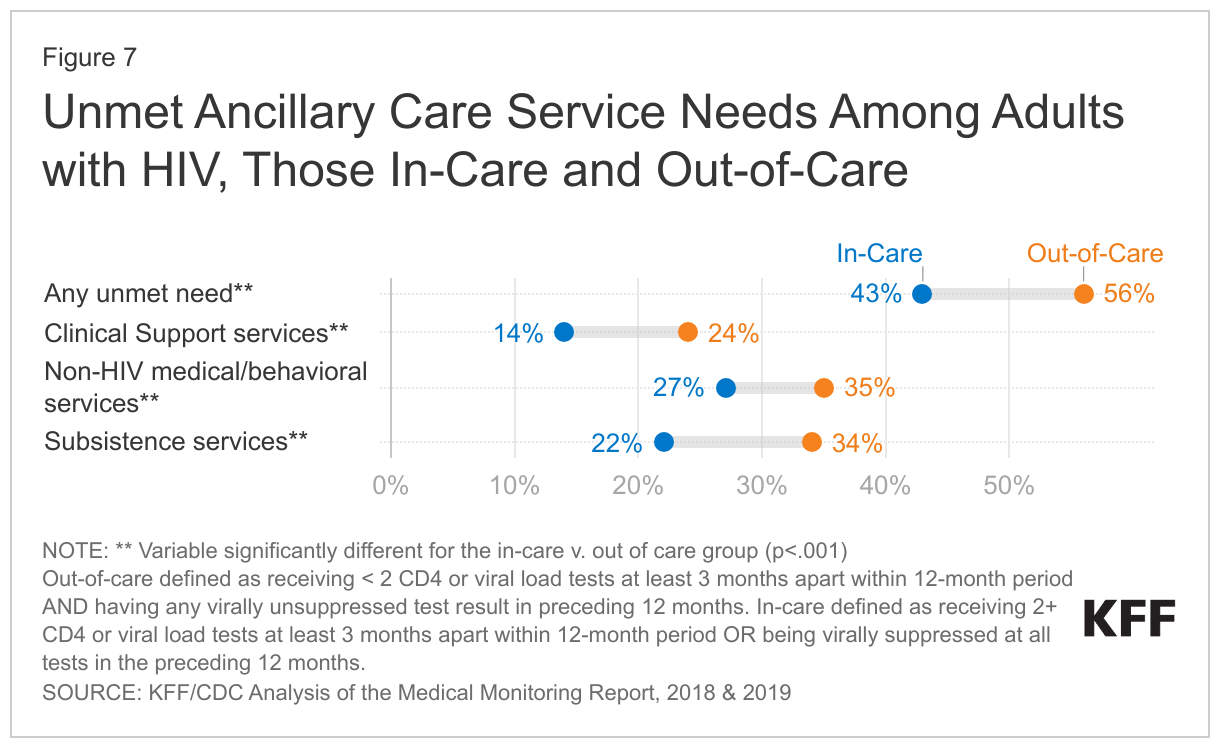
More than half (56%) of people with HIV who were out-of- care had at least one unmet ancillary care need, across three domains, compared to 43% of the in-care population. Unmet need was higher overall as well as in each domain:
- Clinical support services, including case management, adherence counseling, medication through ADAP, peer group, patient navigation services (24% v. 14%)
- Non-HIV medical/behavioral services, including dental care, mental health services, drug/alcohol counseling/treatment, and domestic violence services (35% v. 27%)
- Subsistence services, including SNAP, WIC, meal or food services, transportation assistance, or shelter/housing services (34% v. 22%).
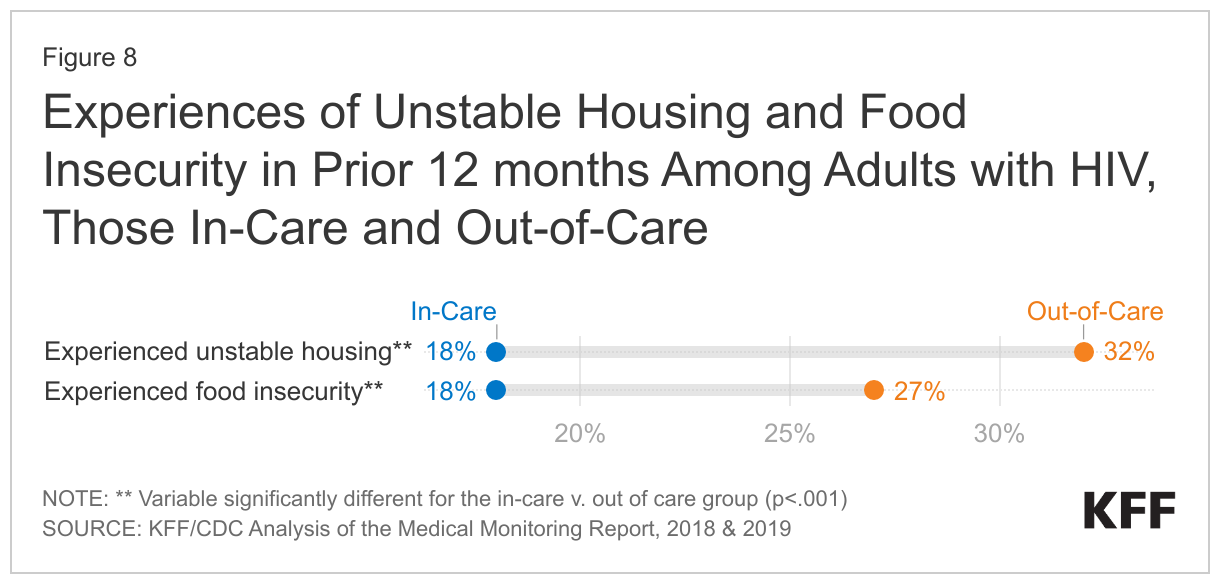
- Specifically, people with HIV who were out-of-care had higher levels of unstable housing or homelessness (32% v. 18%) and hunger/food insecurity (27% v. 18%) over the preceding 12 months.3
Discussion
Identifying people with HIV who are not in HIV care is a first step towards engaging or reengaging them and addressing their unmet needs. While relevant demographic details may help to better design programs for and reach these individuals, there has been limited data available on this population. This analysis provides nationally representative data on people with HIV who are out-of-care, defined as those who were not virally suppressed and did not receive a minimum number of laboratory tests within the prior year, to better understand their demographics and experiences. We find that in the 2018 to 2020 period, this population was disproportionally younger, uninsured, lower income, and Black. They were also much less likely to be on antiretroviral therapy and many faced overlapping and intersectional structural barriers that can further challenge HIV care engagement and prioritization, including unmet needs for basic, subsistence services such as food, housing, and financial security. That fact that those who were out-of-care were also less likely to be receiving services from the Ryan White Program is notable because the program is a potential resource for reaching this very population with engagement and retention services and in addressing at least some unmet ancillary care needs, though the program is constrained by financial limitations. Additionally, there were substantial knowledge gaps with respect to treatment as prevention, information that may help encourage care engagement when individuals learn they are able to prevent transmission of HIV to sexual partners.
Unless large shares of people with HIV are engaged in care and treatment, it will not be possible to meet most of the goals in the national HIV/AIDS Strategy and the Ending the HIV initiative (e.g. preventing new infections, reducing disparities, etc.). Progress on these efforts has been somewhat stalled in the U.S., which lags behind peer countries in terms of the national viral suppression level. Reaching and engaging people with HIV who are not engaged in care and not yet virally suppressed, will involve addressing the complex, systemic barriers they face, and which have impeded not only their health and wellbeing but the HIV response in the U.S. more broadly.
Methodology
Data on people with HIV are based on 2018 and 2019 data cycles (which cover data through part of 2020) from the Medical Monitoring Project (MMP), a Centers for Disease Control and Prevention (CDC) surveillance system which produces national and state-level representative estimates of behavioral and clinical characteristics of adults with diagnosed HIV in the United States.
MMP employs a two-stage, complex sampling design. First, jurisdictions are selected from all U.S. states, the District of Columbia, and Puerto Rico using a probability proportional to size sampling strategy based on AIDS prevalence at the end of 2002, such that areas with higher prevalence had a higher probability of selection. Next, adults (aged 18 years and older) with diagnosed HIV were sampled from selected jurisdictions from the National HIV Surveillance System (NHSS), a census of U.S. persons with diagnosed HIV. During the 2018 and 2019 MMP data cycles, data came from: California (including the separately funded jurisdictions of Los Angeles County and San Francisco), Delaware, Florida, Georgia, Illinois (including the separately funded jurisdiction of Chicago), Indiana, Michigan, Mississippi, New Jersey, New York (including the separately funded jurisdiction of New York City), North Carolina, Oregon, Pennsylvania (including the separately funded jurisdiction of Philadelphia), Puerto Rico, Texas (including the separately funded jurisdiction of Houston), Virginia, and Washington.
Data used in this analysis were collected via telephone or face-to-face interviews and medical record abstractions during the following periods:
- 2018 data was collected between June 1, 2018–May 31, 2019
- 2019 data was collected between June 1, 2019–May 31, 2020
The response rate was 100% at the first stage, and was 45% for each of the 2 cycles included in this analysis. Data were weighted based on known probabilities of selection at state or territory and patient levels. In addition, data were weighted to adjust for non-response using predictors of person-level response, and post-stratified to NHSS population totals by age, race/ethnicity, and sex at birth. This analysis includes information on 7,642 adults with HIV.
Of the 7,642 adults sampled, 1,215 were identified as being out-of-care (having fewer than two CD4 or viral load tests at least 3 months apart within a 12-month period) and also being virally unsuppressed (having a viral load of equal to or more than 200 copies of HIV per milliliter of blood).
Because respondents in MMP may indicate more than one type of coverage, we relied on a hierarchy to group people into mutually exclusive coverage categories as follows:
- Private coverage overall (with breakouts for employer coverage and marketplace coverage)
- Medicaid coverage, including those dually eligible for Medicare
- Medicare coverage only
- Other public coverage, including Tricare/CHAMPUS, Veteran’s Administration, or city/county coverage
- Uninsured
Differences between groups were assessed using prevalence ratios with predicted marginal means.
It is important to note that insurance coverage data were self-reported by respondents and not verified, as was receipt of Ryan White support. In addition, by relying on a hierarchy to group individuals into coverage categories, it is possible individuals were grouped into a coverage category that was not their dominant payer over the course of a year.
Acknowledgments
The authors wish to thank Dr. Sharoda Dasgupta, Stacy Crim, Tamara Carree, and Dr. Linda Beer of the Centers for Disease Control and Prevention (CDC), who were instrumental in this work in providing access to data, guidance, and conducting statistical analysis.
- A CD4 test is a laboratory test that measures the number of CD4 cells (also known as T cells) in a blood sample. CD4 count is a key laboratory indicator of immune function and indicates HIV stage progression as well as response to HIV treatment. ↩︎
- For example, see: Centers for Disease Control and Prevention. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 dependent areas, 2020. HIV Surveillance Supplemental Report 2022;27(No. 3). https://www.cdc.gov/hiv/library/reports/hiv-surveillance/vol-27-no-3/index.html ↩︎
- People were considered to have experienced unstable housing if they reported any of the following during the preceding 12 months: moving in with others due to financial issues, moving 2 or more times, or being evicted. People were considered to have experienced homelessness if they experienced any of the following during the preceding 12 months: living on the street, in a shelter, in a single-room–occupancy hotel, or in a car. People were considered to be food insecure if they reported being hungry and not eating because they did not have enough money for food during the past 12 months Centers for Disease Control and Prevention. Data Tables: Quality of Life and HIV Stigma— Indicators for the National HIV/AIDS Strategy, 2022–2025, CDC Medical Monitoring Project, 2017–2020 Cycles. HIV Surveillance Special Report 30. Published September 2022. https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-special-report-number-30.pdf. ↩︎