Medicaid and People with HIV
Key Facts
- Medicaid is the largest source of insurance coverage for people with HIV in the United States, covering an estimated 40% of the nonelderly adults with HIV, compared to just 15% of the nonelderly adult population overall.
- Medicaid covers a broad range of services, many of which are important for people with and at risk for HIV, including prescription drugs, inpatient and outpatient care, and preventive services.
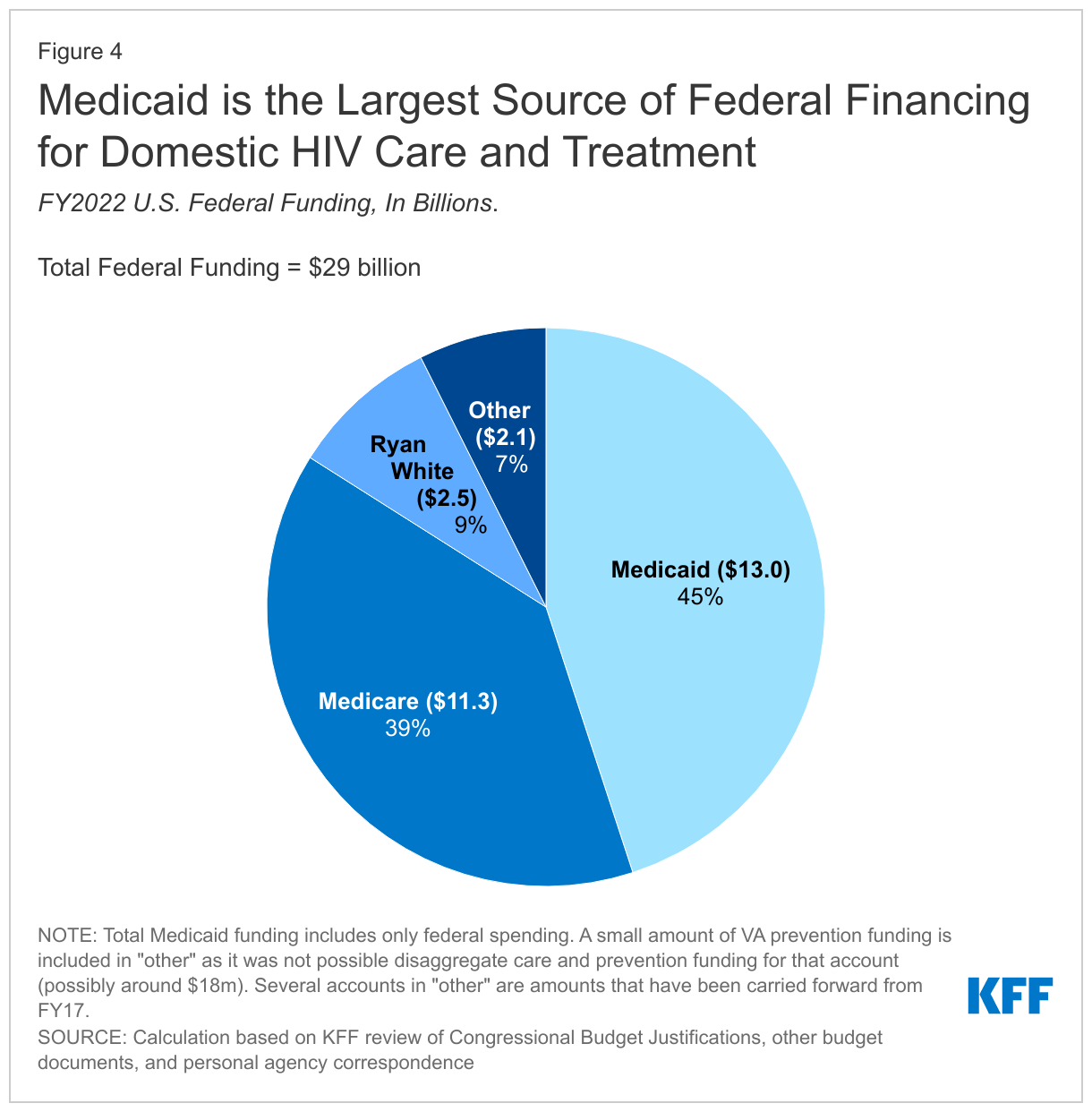
- Medicaid accounted for 45% of all federal HIV spending in FY221 and it is the largest source of public spending for HIV care in the U.S. In FY22, the federal government spent an estimated $13 billion on Medicaid services for people with HIV. Additionally, state Medicaid spending totaled an estimated $5.4 billion in FY22.2 Spending has increased over time, reflecting the growing numbers of enrollees with HIV and the rising cost of care and treatment.
- Medicaid enrollment among people with HIV has grown over time as people with HIV are living longer and new infections continue to occur. The expansion of the program under the Affordable Care Act (ACA) has also increased coverage for people with HIV.
- Medicaid enrollees with HIV are more likely to be male, dually eligible for Medicare, and to qualify based on disability, compared to enrollees overall.
Overview
Medicaid, the largest public health insurance program in the United States, covering health and long-term care services for 83.9 million low-income individuals, has played a critical role in HIV care since the HIV epidemic began. It is the single largest source of coverage for people with HIV in the U.S., and its role has grown over time as people with HIV are living longer, new infections continue to occur, and due to the program’s expansion under the Affordable Care Act (ACA) (see Figure 1).
Medicaid Beneficiaries with HIV
Medicaid is the largest source of insurance coverage for non-elderly adults with HIV, estimated to cover 40% of population, compared to just 15% of the nonelderly adult population overall. This number of people covered is higher today due in part to the ACA’s Medicaid expansion, which has been a key factor in recent gains among people with HIV. In addition, new HIV infections continue to occur and people with HIV are living longer, which also contributes to a growing population. While Medicaid is a significant source of coverage for enrollees with HIV, this group represents less than 1% of the overall Medicaid population.
The demographics of Medicaid enrollees with HIV vary significantly from the demographics of the Medicaid population overall:3
- Medicaid enrollees with HIV are more likely to be male (64% vs. 44%) and between the ages of 45-64 (50% vs. 17%) than the Medicaid population overall (data on race/ethnicity is not available due to data limitations).
- One-in-four (25%) are dually eligible for both Medicaid and Medicare, compared to 14% of the Medicaid population as a whole; dually eligible enrollees are among the most chronically ill enrollees and have the highest spending, with many having multiple chronic conditions and requiring long-term care.
- Enrollees with HIV also have a higher prevalence of certain co-morbidities. Nine percent (9%) have a hepatitis diagnosis compared to just 1% of the general Medicaid population, a decrease from 14% in 2013, potentially reflecting the impact of curative treatment for hepatitis C.
- Enrollees older than 18 with HIV also face significant mental health and substance use disorder comorbidities, including 46% who have such a diagnosis compared to 25% of all other Medicaid enrollees older than 18 (see Figure 2).
Medicaid Eligibility for People with HIV
Most Medicaid enrollees with HIV (41% in 2019) qualify for coverage through a disability pathway, compared to just 11% of the Medicaid population overall. The remaining share qualify through multiple other mandatory and optional pathways (see Table 1 for a discussion of pathways).
| Table 1: Medicaid Eligibility Pathways for People with HIV | ||
| Category | Criteria | Mandatory / Optional |
| SSI Enrollees | States must generally provide Medicaid to those receiving Supplemental Security Income (SSI) benefits; some states elect the Section 209(b) option to use more restrictive eligibility criteria. To be eligible for SSI, enrollees must have low incomes (about 74% of the federal poverty level [FPL]), limited assets, and a significant disability. | Mandatory, though as of 2022, 8 are more restrictive Section 209(b) states. |
| Children | States required to cover children <19 up to 138% FPL; all states currently cover up to higher incomes with a median eligibility level of 255% (upper limits ranging from 175% FPL in ND to 405% FPL in NY). | Mandatory |
| Pregnant Women | States required to cover pregnant women up to 138% FPL; most cover at higher limits with a median eligibility level of 200% FPL in 2022 (upper limits ranging from 138% FPL in ID, LA, OK, SD to 380% FPL in IA). | Mandatory |
| Parent/Caretaker Relatives | States are required to provide coverage to certain parents (known as Section 1931 parents). States that have expanded Medicaid fulfill that requirement. States that have not expanded Medicaid offer coverage at income thresholds ranging from 16% FPL (TX) to 100% FPL (WI) in 2022. In addition, two expansion states offer coverage above the ACA expansion level (CT, & DC). | Mandatory for Section 1931 parents with state option to expand beyond federal income minimum. |
| Low-income Adults | ACA expansion group for adults under 65 years old up to 138% FPL, regardless of disability status. | Mandated by ACA; effectively state option due to SCOTUS ruling.
(40 states including DC offer coverage, 11do not as of November 2022) |
| Seniors and Persons with Disabilities up to 100% FPL | State option to provide Medicaid to seniors and people with disabilities whose income exceeds SSI limits, up to 100% FPL. | Optional (22 states in 2022) |
| Medically Needy (MN) | State option to extend Medicaid to those who meet categorical eligibility, such as disability status, but need to “spend down” by incurring medical expenses to meet state’s income criteria. | Optional (34 states including DC as of 2022) |
| Buy-in for Working People with Disabilities | State option to provide Medicaid to working individuals with disabilities at higher income/asset limits. Limits and income related premiums/cost-sharing vary by state (median 250% FPL in 2022). | Optional (48 States as of 2022) |
| SOURCES: Kaiser Family Foundation. State Health Facts. https://www.kff.org/state-category/medicaid-chip/; Musumeci, M., et al. Kaiser Family Foundation. Medicaid Financial Eligibility in Pathways based on Old Age or Disability in 2022: Findings from a 50-State Survey, 2022. https://www.kff.org/report-section/medicaid-financial-eligibility-in-pathways-based-on-old-age-or-disability-in-2022-findings-from-a-50-state-survey-appendix/ ; Brooks T., et al. Kaiser Family Foundation. Medicaid and CHIP Eligibility and Enrollment Policies as of January 2022: Findings from a 50-State Survey, 2022. https://www.kff.org/report-section/medicaid-and-chip-eligibility-and-enrollment-policies-as-of-january-2022-findings-from-a-50-state-survey-tables/ | ||
Prior to the ACA, to qualify for Medicaid an individual had to be both low income and “categorically eligible,” such as being a person with a disability or pregnant. This presented a “catch-22” for many low-income people with HIV who could not qualify for Medicaid until they were already quite sick and disabled, despite the fact that early access to treatment could help stave off disability and significantly improve health outcomes.
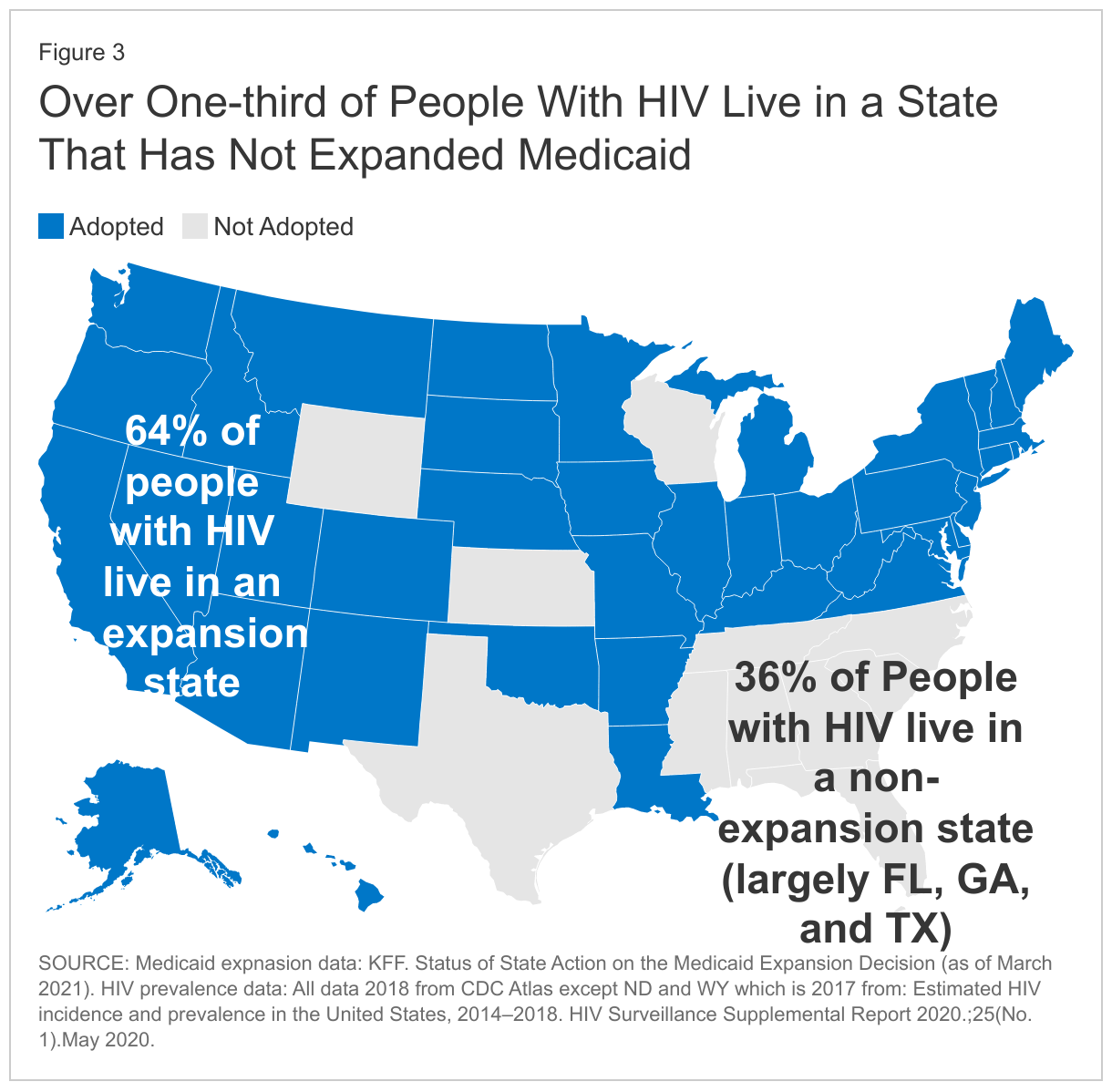
The ACA sought to fundamentally change this by requiring states to expand their Medicaid programs to nearly all individuals with incomes at or below 138% of poverty ($20,120 for an individual in 2023). However, a 2012 Supreme Court ruling on the constitutionality of the ACA effectively made expansion a state option. As of November 2022, 40 states including Washington, D.C. have adopted the ACA Medicaid expansion, where approximately two thirds (64%) of people with HIV live. Eleven states have not expanded their programs, where 36% of people with HIV live, most of whom are in Florida, Georgia, and Texas.
More recently, Congress passed emergency relief legislation during the COVID pandemic which lead to an increase in Medicaid enrollment overall (30.4% in the past two years) and likely among people with HIV as well. This provision will end on March 31, 2023. As a result, enrollment could decline if individuals are no longer eligible or face administrative barriers during renewal (see Figure 3).
Medicaid Spending on People with HIV
Medicaid is a means-tested entitlement program, jointly financed by the federal and state governments. In the traditional (non-expansion) program, the federal government matches state Medicaid spending at rates ranging from 56% to 85% (using a formula based on state per capita income). Under the ACA, the federal match for the expansion population began at 100% in 2014 and phased down to 90% in 2020 and thereafter. Additionally, the above mentioned COVID relief legislation provided states with an additional 6.2 percentage point federal match during the public health emergency, until amended by the FY23 Omnibus.
In FY 2022, federal Medicaid spending on HIV was estimated to total $13.0 billion and increasing from $5.5 billion in 2013.4 Medicaid spending on people with HIV accounted for an estimated 45% of all federal spending on HIV care and is the largest source of public financing for HIV care in the U.S, followed by Medicare (see Figure 4). Still, in FY 2022 federal Medicaid spending on HIV represents less than 2% of total federal Medicaid spending. In addition, the states’ share of Medicaid spending on HIV was estimated to be an additional $5.4 billion in FY 2022.5 Medicaid spending on HIV has increased over time, reflecting growing numbers of enrollees with HIV and the rising cost of care and treatment.
Average annual per capita spending on Medicaid fee-for-services enrollees with HIV was $13,725 in 2019, more than three times that of Medicaid enrollees overall ($3,087)6. In addition, Medicaid enrollees with HIV have different spending patterns than enrollees overall (see Figure 5), and spending on HIV treatment, due to the high cost of HIV medications, has an outsized impact on the program.7
While less than half of one percent of Medicaid enrollees have HIV, in 2019, spending on antiretrovirals, drugs used to treat and prevent HIV totaled $5 billion and accounted for 7% of gross Medicaid outpatient drug spending. Gross spending on antiretrovirals is disproportionate to their utilization and reflects the high cost of these drugs. In addition, another $1.2 billion was spent on treatment for hepatitis C. Both hepatitis C treatment and antiretrovirals are part of the antiviral drug class which is consistently the most costly drug group in the program.
Medicaid Benefits
Medicaid covers a broad range of benefits, many of which are important for people with and at risk for HIV (described below). Medicaid benefits are offered on a fee-for-service basis, through capitated managed care organizations (MCOs), or through a combination of these benefit designs. In fee-for-service programs, states pay providers for covered services delivered to enrollees and in managed care programs, states make a capitated payment to a managed care plan on behalf of each enrollee.
Recognizing the high cost of drugs, especially those used for treating certain conditions, such as HIV, some managed care states “carve-out” prescription drug benefits from these plans, instead using their fee-for-service program to deliver this benefit. In FY22, of the 41 states that deliver some care through MCOs, 6 (CA, ND, MO, WI, TN, WV) carve-out pharmacy benefits and 2 (MI and DC) specifically carve-out antiretrovirals used to treat HIV. In FY20, Maryland went from carving out antiretrovirals to carving them in.
States are permitted to require “nominal” cost-sharing by some groups of enrollees, although many states do not do so; other groups and services are exempt altogether. Generally, even in states with cost-sharing policies, enrollees are not denied services based on inability to pay, though they may be held liable for unpaid copayments.
While most states that have expanded their Medicaid programs have fully aligned the benefits in their traditional program with the benefits for the expansion population, there are technically different requirements between the two, with potential implications for HIV care and prevention.
Traditional Medicaid Programs
Under traditional Medicaid, states must cover certain mandatory services, specified in federal law, in order to receive federal matching funds, though they have some flexibility in determining the scope of services. They may also cover optional services. (See Table 2.)
| Table 2: Traditional Medicaid Service Categories | |
Required Services Include:
|
Optional Services Include:
|
In addition, traditional Medicaid programs also cover certain preventive services including ones that are important to people with HIV:
- Programs must cover “medically necessary” HIV testing (i.e. indicated due to risk) and may cover routine HIV testing (screening regardless of risk). In a 2021 survey, of 42 responding jurisdictions, 40 states and DC report covering routine HIV testing while just one state, Florida, reported covering only “medically necessary” testing. Nine states did not respond, including 3 that reported covering only ‘medically necessary” testing in a prior survey (GA, NE, and SD)
- States must also cover pre-exposure prophylaxis (PrEP), the drug used to prevent HIV among those at increased risk.
Under the ACA, states are incentivized to cover a full suite of preventive services receiving an “A” or “B” rating from the United States Preventive Services Task Force (USPSTF), including routine HIV testing and PrEP, without cost-sharing through their traditional programs in exchange for a 1% increase in the federally matching rate for those services. As of November 2021, 16 states (CA, CO, DE, HI, KY, LA, MA, MT, NH, NJ, NV, NY, OH, OR, WA and WI) cover all USPSTF “A” and “B” graded these services under Sec. 4106 of the ACA.
Medicaid Expansion Programs
Most enrollees who gain access to Medicaid through the ACA expansion receive the same benefits as traditional enrollees because most states have elected to align their traditional and expansion programs. However, there are technical differences and expansion enrollees must receive services that fall into the ACA’s ten “essential health benefit” (EHB) categories, many of which are important for HIV care (see Table 3):
| Table 3: Essential Health Benefit Categories |
|
Benefits within these categories are largely defined through a state-based benchmarking process using a plan of the state’s choosing from federally mandated options or from an alternative plan through a waiver. Most states have used a waiver to select the traditional state Medicaid plan as the benchmark and align traditional and expansion benefits. Preventive services in expansion programs are unique in that they are specifically defined to include services receiving an “A” or “B” rating from USPSTF, including routine HIV screening and PrEP, which must be offered without cost-sharing.
Medicaid Health Homes
The ACA also gave states an option to provide Medicaid health home services to enrollees with chronic conditions (and receive a temporary enhanced federal match of 90% for the first two program years). Health homes encompass a range of services designed to help manage care for those who are chronically ill, such as comprehensive care management and care coordination. The law named several chronic conditions that could be targeted for health homes, and CMS considers others, including HIV, for states pursuing this option. As of March 2022, 34 health homes had approval in 19 states and DC. Among these, two states (WA, MI) included HIV among other qualifying conditions for enrollment into the health home and one state, Wisconsin, designed a health home specifically for enrollees with HIV/AIDS.
Waivers
States also have the ability to seek waivers from certain Medicaid requirements, such as Section 1115 Medicaid demonstration waivers to experiment with approaches to delivering benefits in ways that differ from what is allowed under statute and could impact people with HIV. Waivers can serve to both promote or restrict access to the program or certain services and proposals and approvals often reflect priorities and policy positions of states and the federal government. For example, Maine has an approved 1115 waiver for individuals with HIV/AIDS that allows for a limited package of “essential” services, including case management services that are not otherwise available under the state plan. Recent waivers have also allowed states to purchase marketplace health plans for the expansion population, increase cost-sharing, provide additional benefits or offer benefits to new populations (e.g., substance use treatment, family planning, etc.), and transform how care is delivered or paid for.
States also have the option to apply for a “home and community-based services (HCBS)” waiver. Medicaid HCBS waiver authorities include Sec. 1915 (c) and Sec. 1115, both of which allow states to expand financial eligibility and offer HCBS to seniors and people with disabilities who would otherwise qualify for an institutional level of care. HCBS waivers have been important for people with HIV and are used by several states to serve this population. As of 2021, 5 states had an HCBS designed specifically for or inclusive of people with HIV, serving over ten thousand people with HIV.
In some cases, people with HIV may not have access to all the health services needed to stay healthy through Medicaid alone and rely on support from other payers or programs, including the Medicare program for those who are dually eligible, and the Ryan White HIV/AIDS Program, the federal safety-net program for people with HIV who are uninsured and underinsured.
Future Outlook
As the single largest source of health coverage for people with HIV, Medicaid has played a significant role for this population since the HIV epidemic began and its role has continued to grow. In particular, many low-income people with HIV who could not previously qualify for Medicaid because they did not meet categorical eligibility criteria, such as disability, have gained access under the ACA. Going forward, it will be important to continue to assess the impact of Medicaid coverage on people with and at risk for HIV, particularly given that states are still electing to expand their programs, including through voter led ballot initiatives. At the same time, as continued eligibility through the COVID emergency relief legislation ends in April 2023, millions of people are expected to lose coverage which for those with and at risk for HIV could lead to treatment interruptions, threatening the therapeutic and preventive benefits of antiretrovirals.
Endnotes
Calculation based on KFF review of Congressional Budget Justifications, other budget documents, and personal agency correspondence.
Data received via personal communication with CMS. Amounts are pre-rebate.
Unless otherwise noted, findings are based on KFF analysis of 2019 Release 1 T-MSIS Transformed Medicaid Statistical Information System (T-MSIS). Medicaid enrollees with HIV in 2019 were identified using ICD-10 codes for HIV (B20, Z21, B97.53) and NDC codes for ARV utilization.
Data received via personal communication with CMS. Amounts are pre-rebate.
Data received via personal communication with CMS.
The amount of drug spending described here represents the pre-rebate amount and actual program spending is likely substantially lower, but the negotiated discounts are proprietary and not publicly available.
Categorical spending estimates for enrollees covered by managed care are unavailable due to data limitations.