There are two types of financial assistance available to Marketplace enrollees. The first type, called the premium tax credit (or premium subsidy), reduces enrollees’ monthly payments for insurance coverage. The second type of financial assistance, the cost-sharing reduction (CSR), reduces enrollees’ deductibles and other out-of-pocket costs when they go to the doctor or have a hospital stay. To receive either type of financial assistance, qualifying individuals and families must enroll in a plan offered through a health insurance Marketplace. In addition to the federal subsidies discussed here, some states that operate their own exchange markets offer additional state-funded subsidies that further lower premium payments and/or deductibles or other forms of cost-sharing.
Premium Subsidies
Premium tax credits can be applied to Marketplace plans in any of four “metal” levels of coverage: bronze, silver, gold, and platinum. Bronze plans tend to have the lowest premiums but have the highest deductibles and other cost sharing, leaving the enrollee to pay more out-of-pocket when they receive covered health care services, while platinum plans have the highest premiums but very low out-of-pocket costs. There are also catastrophic plans, usually only available to younger enrollees, but the subsidy cannot be used to purchase one of these plans.
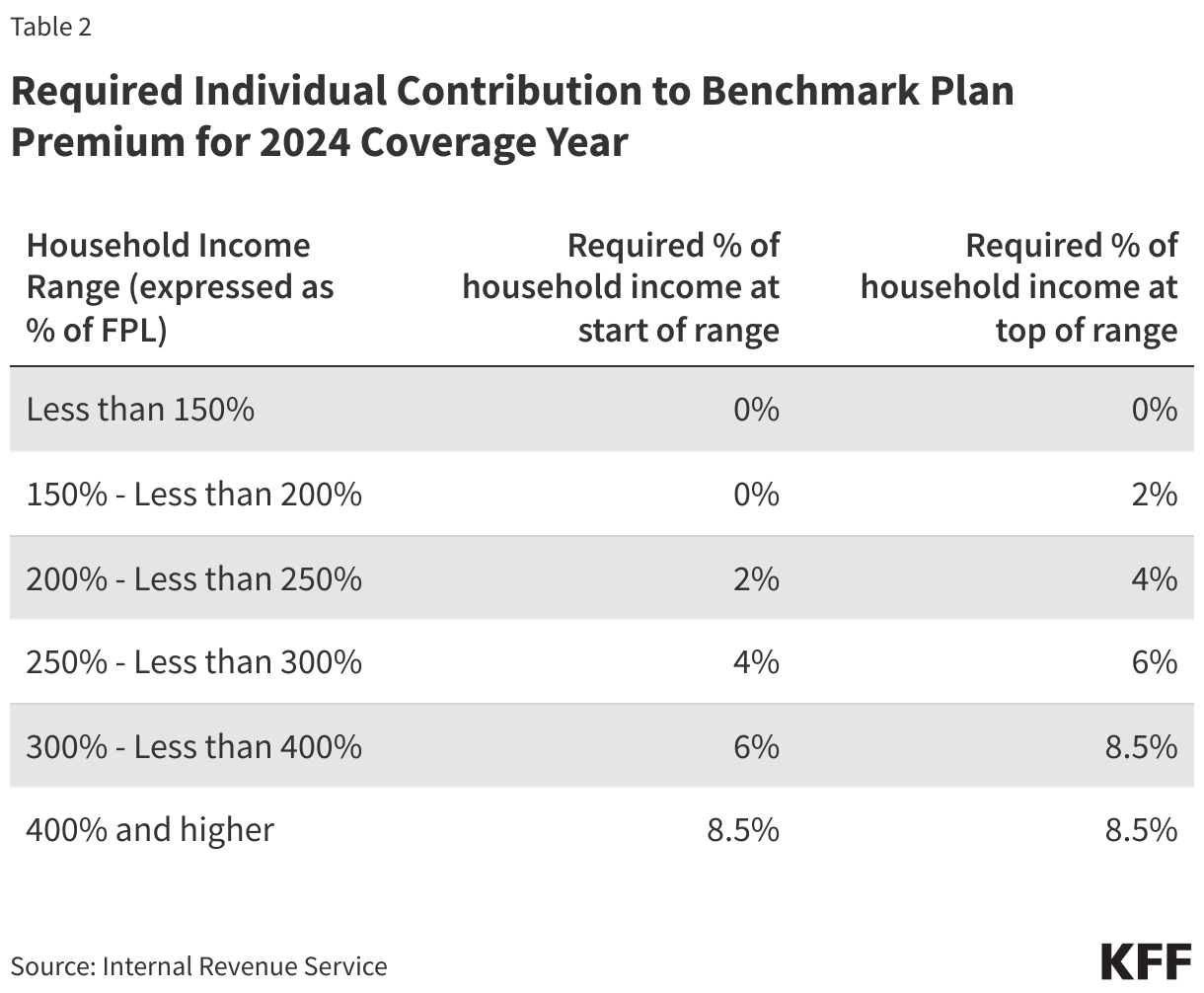
The premium tax credit works by limiting the amount an individual must contribute toward the premium for the “benchmark” plan – or the second-lowest cost silver plan available to the individual in their Marketplace. This “required individual contribution” is set on a sliding income scale. In 2024, for individuals with income up to 150 percent FPL, the required contribution is zero, while at an income of 400 percent FPL or above, the required contribution is 8.5 percent of household income.
These contribution amounts were set by the American Rescue Plan Act (ARPA) in 2021 and temporarily extended by the Inflation Reduction Act (IRA) through the end of 2025. Prior to the ARPA, the required contribution percentages ranged from about two percent of household income for people with poverty level income to nearly 10 percent for people with income from 300 to 400 percent of poverty. Before the ARPA was passed, people with incomes above 400 percent of poverty were not eligible for premium tax credits. If Congress does not act to extend the IRA subsidies before the end of 2025, they will expire, and the original ACA premium caps will return.
The amount of tax credit is calculated by subtracting the individual’s required contribution from the actual cost of the “benchmark” plan. So, for example, if the benchmark plan costs $6,000 annually, the required contribution for someone with an income of 150 percent FPL is zero, resulting in a premium tax credit of $6,000. If that same person’s income equals 250 percent FPL (or $36,450 in 2024), the individual contribution is four percent of $36,450, or $1,458, resulting in a premium tax credit of $4,542.
The premium tax credit can then be applied toward any other plan sold through the Marketplace (except catastrophic coverage). The amount of the tax credit remains the same, so a person who chooses to purchase a plan that is more expensive than the benchmark plan will have to pay the difference in cost. If a person chooses a less expensive plan, such as the lowest-cost silver plan or a bronze plan, the tax credit will cover a greater share of that plan’s premium and possibly even the entire cost of the premium. When the tax credit exceeds the cost of a plan, it lowers the premium to zero and any remaining tax credit amount is unused.
As mentioned above, the premium tax credit will not apply for certain components of a Marketplace plan premium. First, the tax credit cannot be applied to the portion of a person’s premium attributable to covered benefits that are not essential health benefits (EHB). For example, a plan may offer adult dental benefits, which are not included in the definition of EHB. In that case, the person would have to pay the portion of the premium attributable to adult dental benefits without financial assistance. In addition, the ACA requires that premium tax credits may not be applied to the portion of premium attributable to “non-Hyde” abortion benefits. Marketplace plans that cover abortion are required to charge a separate minimum $1 monthly premium to cover the cost of this benefit; this means a consumer who is otherwise eligible for a fully subsidized, zero-premium policy would still need to pay $1 per month for a policy that covers abortion benefits. Finally, if the person smokes cigarettes and is charged a higher premium for smoking, the premium tax credit is not applied to the portion of the premium that is the tobacco surcharge.
Cost-Sharing Reductions
The second form of financial assistance available to Marketplace enrollees is a cost-sharing reduction. Cost-sharing reductions lower enrollees’ out-of-pocket cost due to deductibles, copayments, and coinsurance when they use covered health care services. People who are eligible to receive a premium tax credit and have household incomes from 100 to 250 percent of poverty are eligible for cost-sharing reductions.
Unlike the premium tax credit (which can be applied toward any metal level of coverage), cost-sharing reductions (CSR) are only offered through silver plans. For eligible individuals, cost-sharing reductions are applied to a silver plan, essentially making deductibles and other cost sharing under that plan more similar to that under a gold or platinum plan. Individuals with income between 100 and 250 percent FPL can continue to apply their premium tax credit to any metal level plan, but they can only receive the cost-sharing subsidies if they pick a silver-level plan.
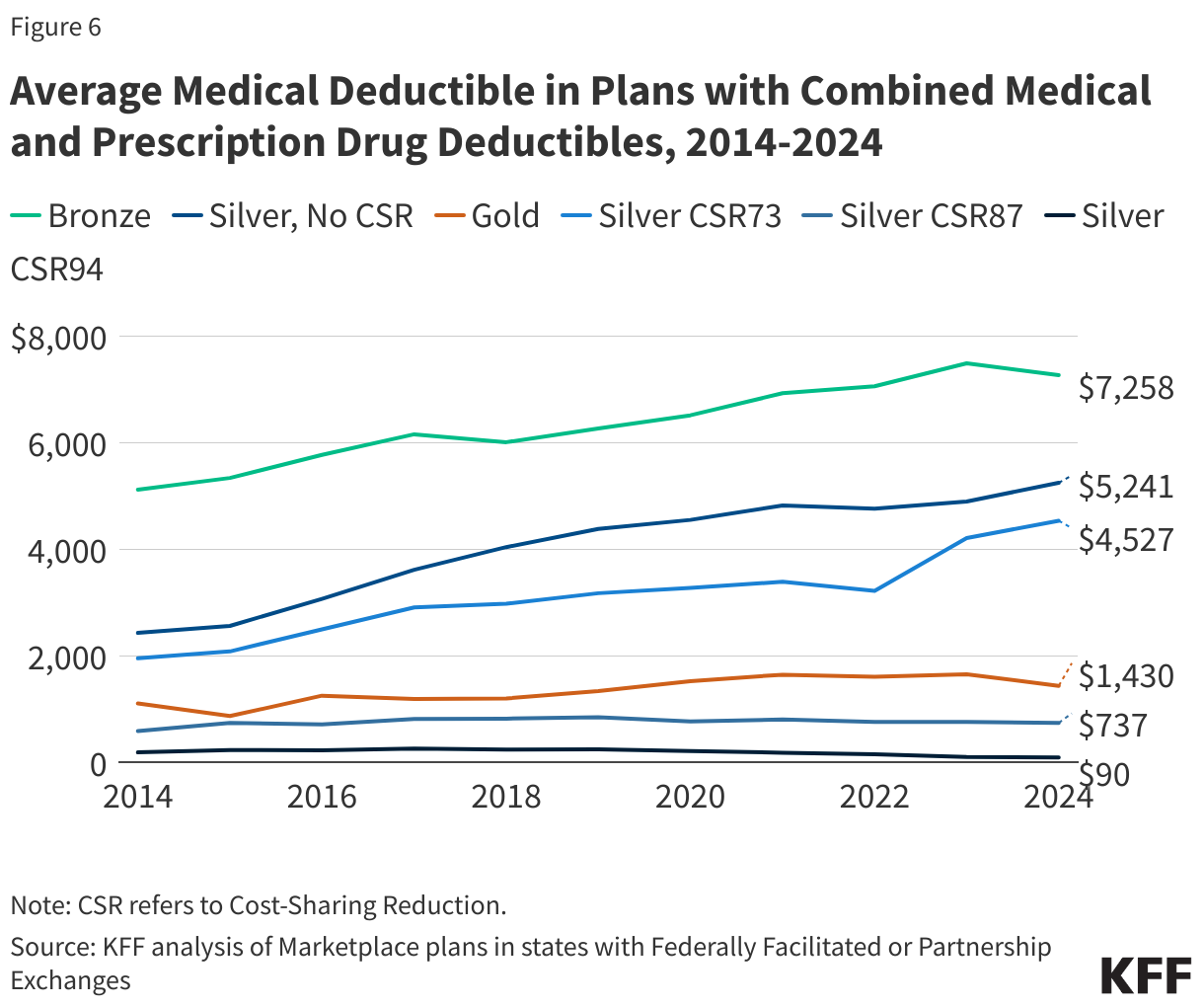
Cost-sharing reductions are determined on a sliding scale based on income. The most generous cost-sharing reductions are available for people with income between 100 and 150 percent FPL. For these enrollees, silver plans that otherwise typically have higher cost sharing are modified to be more similar to a platinum plan by substantially reducing the silver plan deductibles, copays, and other cost sharing. For example, in 2024, the average annual deductible under a silver plan with no cost-sharing reduction is over $5,000, while the average annual deductible under a platinum plan was $97. Silver plans with the most generous level of cost-sharing reductions are sometimes called CSR 94 silver plans; these plans have 94 percent actuarial value (which represents the average share of health spending paid by the health plan) compared to 70 percent actuarial value for a silver plan with no cost-sharing reductions.
Somewhat less generous cost-sharing reductions are available for people with income greater than 150 and up to 200 percent FPL. These reduce cost sharing under silver plans to 87 percent actuarial value (CSR 87 plans). In 2024, the average annual deductible under a CSR 87 silver plan was about $700.
For people with income greater than 200 and up to 250 percent FPL, cost-sharing reductions are available to modestly reduce deductibles and copays to 73 percent actuarial value (sometimes called CSR 73 plans). In 2024, the average annual deductible under a CSR 73 silver plan was about $4,500.
Insurers have flexibility in how they set deductibles and copays to achieve the actuarial value under Marketplace plans, including CSR plans, so actual deductibles may vary from these averages.
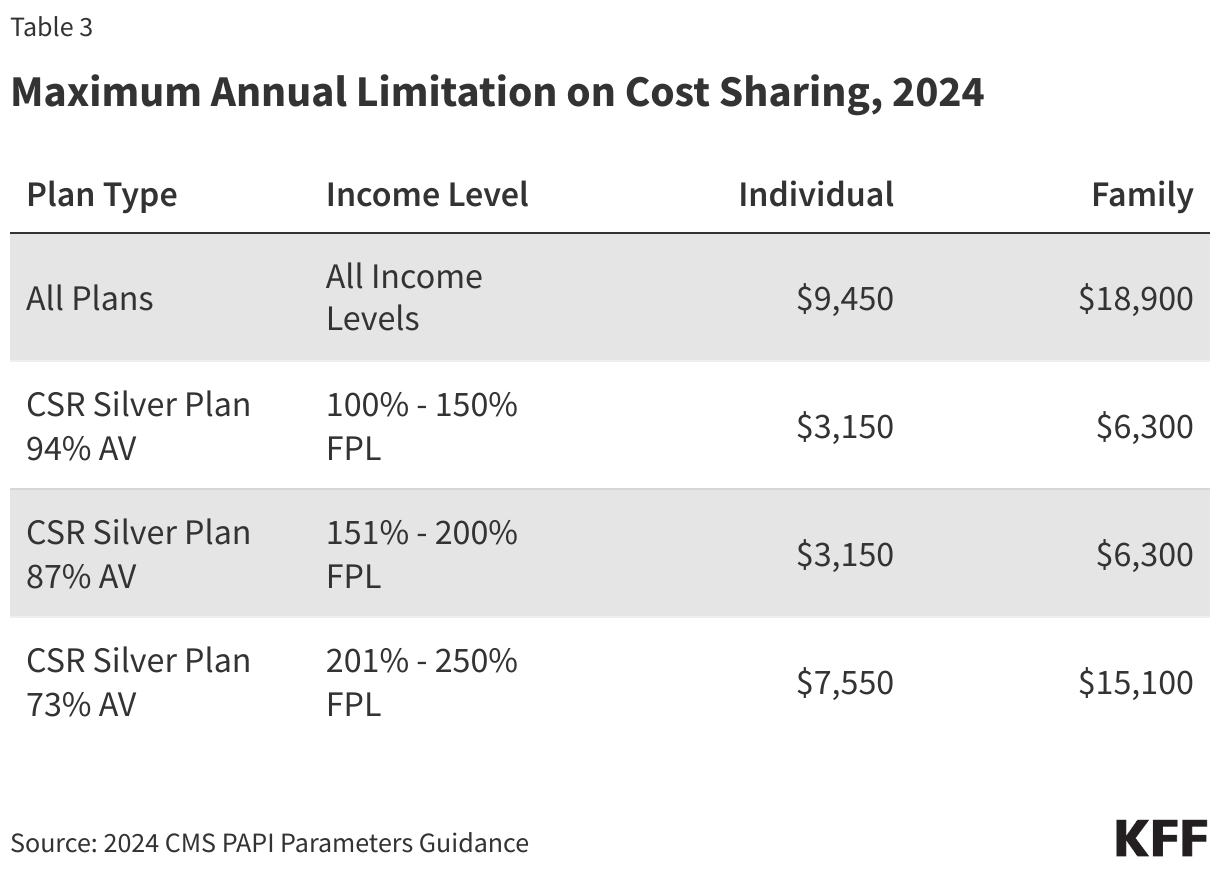
The ACA also requires maximum annual out-of-pocket spending limits on cost sharing under Marketplace plans, with reduced limits for CSR plans. In 2024, the maximum OOP limit is $9,450 for an individual and $18,900 for a family for all QHPs. Lower maximum OOP limits are permitted under cost-sharing reduction plans.
Cost-sharing reductions work differently for Native American and Alaska Native members of federally recognized tribes. For these individuals, cost-sharing reductions are available at higher incomes and can be applied to metal levels other than silver plans.