The International Health Regulations and the U.S.: Implications of an Amended Agreement
This brief was updated on June 18 to reflect developments at the 2024 World Health Assembly.
In 2022, due to challenges and gaps exposed by the COVID-19 pandemic, member states of the World Health Organization (WHO) agreed to a process to review and potentially revise an existing international legal agreement known as the International Health Regulations (IHR). This agreement outlines rights and responsibilities of WHO and governments, including the U.S., in handling international public health events and global health emergencies such as pandemics. The IHR are separate from, though somewhat overlapping with, the potential “pandemic agreement” that has also been negotiated in parallel by WHO member states. The IHR negotiation process reached its conclusion at this year’s World Health Assembly (WHA) meeting, with member states formally approving a number of revisions to the IHR on June 1, 2024 (at the same time, member states did not reach consensus on a pandemic agreement text and those negotiations will continue into 2025).
The U.S. government, already a party to the IHR, was actively engaged in the negotiations since they began, with Biden Administration officials highlighting a number of U.S. priorities, many of which are in the final revised document. At the same time, Republican lawmakers have criticized the IHR, calling for comprehensive WHO reform before having the U.S. support any IHR amendments. More generally, the outcome of U.S. elections in November stands to significantly affect U.S. engagement with the WHO; if President Trump is elected, he is expected to initiate a process to end U.S. membership in the WHO, as he did when he was President, and as recommended by Project 2025, widely seen as a blueprint for another Trump administration.
Here we review what the IHR agreement is, the revisions that have been approved, and the role of and implications for the United States.
What are the International Health Regulations (IHR)?
The IHR are an international legal agreement adopted by all 194 member states1 of the WHO, authorized under Article 21 of the WHO Constitution, which allows the adoption of regulations concerning “sanitary and quarantine requirements and other procedures designed to prevent the international spread of disease.” The agreement at WHO dates back to 1951 (when they were called the International Sanitary Regulations) and has been revised multiple times since then, including adoption of the IHR name as part of the revision in 1969. Before this year, the most recent version was approved in 2005, in the wake of the original SARS epidemic.
The agreement is legally binding for member states of the WHO, meaning parties have agreed to be subject to the implementation and other requirements in the IHR text (see below for further information on these requirements). However, there is no mechanism to ensure or enforce compliance by member states and WHO does not have a role in, or any means to, enforce their implementation in countries.
What are some key elements of the IHR?
The IHR set out definitions, principles, rules, and obligations for countries and the WHO in preparing for and responding to international public health emergencies. For example, through the IHR member states have agreed to:
- report all potential international health threats (according to an agreed-upon rubric in Annex 2 of the IHR) to WHO within 24 hours of their detection whether they occur naturally, accidentally, or intentionally,
- develop national “core capacities” to detect and respond to health threats, including in the areas of laboratories, surveillance, human resources, and national policy and legislation,
- designate a National IHR Focal Point available for 24/7 communications with WHO, and
- collaborate with and assist each other in meeting core capacity and other obligations, including through technical and financial assistance (especially in support of developing countries).
WHO roles and responsibilities under the IHR include:
- collecting and assessing information about potential public health emergencies of international concern (PHEICs) from member states and other sources,
- coordinating with and assisting, when applicable, member states to investigate and respond to potential PHEICs,
- following a process to officially declare a PHEIC, including having an Emergency Committee of external experts provide input and recommendations to the WHO Director-General,
- developing and regularly reviewing recommended health measures for countries to implement during PHEICs with input from an Emergency Committee, and
- providing guidance and assistance to countries affected or threatened by a PHEIC as requested.
What have been U.S. obligations under the prior version of the IHR?
The U.S. has been a supporter of and state party to the IHR since their inception. In 1996, President Clinton issued a Presidential Decision Directive calling for the U.S. to support the process to amend the IHR. In 2005, countries agreed to a number of revisions, and that version of the IHR went into effect for the U.S. in July 2007. The IHR (2005) was adopted as a sole executive agreement (which means it did not require review and consent from the Senate). At the time, the Bush administration did submit a formal reservation and three understandings to the agreement, citing concerns for implementation in the U.S. related to federalism and national security, among others.
As a state party to the IHR, the U.S. has already been obligated to meet certain requirements. One is to designate a National IHR Focal Point to serve as the main point of contact for communications with WHO. The U.S. National IHR Focal Point includes the HHS Secretary’s Operation Center (SOC), Office of Global Affairs (OGA), and Assistant Secretary for Preparedness and Response (ASPR). The OGA is responsible for event assessments, managing IHR National Focal Point policies and procedures, and IHR monitoring and evaluation, the SOC monitors IHR communications 24/7, and the ASPR is the authorizing official for formal communications and notifications to the WHO.
In addition, the U.S. is obligated to develop and maintain capacities related to detecting and responding to public health emergencies. These capacities include surveillance, laboratory systems, human resources, financing, among others. Each year, state parties, including the U.S., are expected to submit a self-assessment report (known as the IHR States Parties Self-Assessment Report, or SPAR) on their progress in reaching and maintaining these capacities. While SPAR is the only mandatory reporting requirement, there are numerous other resources available to state parties to assess their implementation of the IHR, including the Joint External Evaluation (JEE). The JEE involves a joint evaluation of public health emergency response capabilities between the state party’s own experts and an external team. Though voluntary, the U.S. completed a JEE in 2016, and is planning to conduct a new JEE by the end of 2024. The U.S. has also supported other state parties in developing national plans for health security following a JEE.
What changes are included in the newly revised IHR?
Following the COVID-19 pandemic, WHO member states and other key global health stakeholders acknowledged gaps and areas that could be improved in the existing IHR, and recommended strengthening the agreement to improve global health emergency preparedness and response for future outbreaks and pandemics.
Potential revisions to the agreement have been negotiated by member states via the member state-led Working Group on the International Health Regulations (WGIHR), which has convened eight formal sessions since November 2022. The most recent session occurred from April 22 to April 26; a draft of the proposed text changes was provided to member states by WGIHR on April 17, 2024, and final wording changes continued to be negotiated over the next six weeks. Member states were able to reach consensus on the proposed text, and on June 1, 2024, formally approved revisions to the agreement.
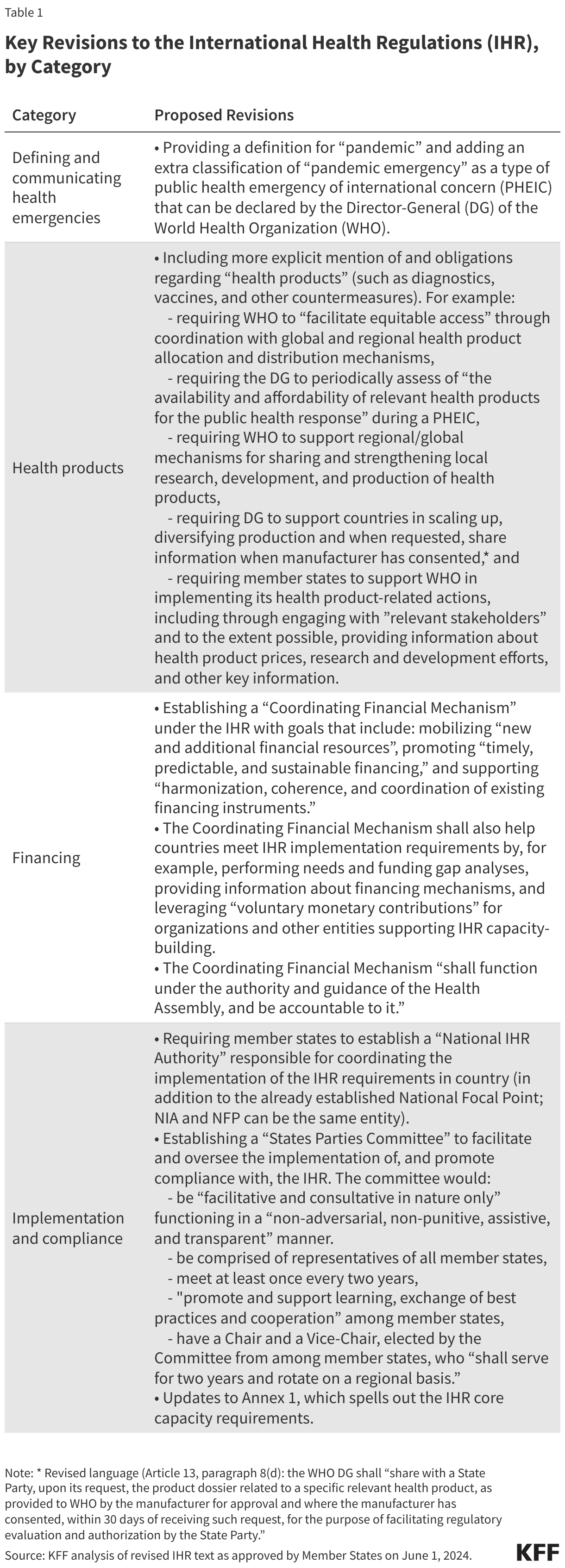
Some of the key revisions and additions in the updated IHR (2024) agreement are presented in Table 1.
How are the IHR and ‘Pandemic Agreement’ related?
The IHR and pandemic agreement negotiation processes have happened in parallel, both with facilitation from the WHO. Both instruments are focused on the same basic issues: improving global capacity and coordination to address the threat of health emergencies such as outbreaks and pandemics. They have similar statements of purpose: the IHR’s purpose as stated in the current (2005) version is to “to prevent, protect against, control and provide a public health response to the international spread of disease” (Article 2), while the language in the latest draft (from April 22) of the pandemic agreement defines its purpose as “to prevent, prepare for and respond to pandemics” (Article 2). Among other areas of overlap, both instruments discuss obligations for member states to commit to capacity-building and mobilizing financing, particularly for developing countries.
However, there are also differences. Elements unique to the IHR that the pandemic agreement does not address include:
- responsibilities and guidance for member states for reporting potential PHEICs, and the rules by which health emergencies are declared by WHO,
- rules on points of communication between states and WHO, and
- rules regarding points of entry and conveyances in the context of health emergencies.
- Elements unique to the draft pandemic agreement that the IHR do not address include:
- a proposed pathogen and benefits sharing (PABS) system,
- the establishment of a “coordinating” financial mechanism for pandemic prevention and response, and
- explicit inclusion of a “One Health” approach to pandemics (that addresses human, animal, and ecosystem considerations).
Further, the legal status of the two instruments could differ. While the IHR are considered a “regulation” that is authorized under Article 21 the WHO Constitution, the pandemic agreement is being positioned legally as a “treaty” authorized under Article 19. Approval of the pandemic agreement as a “treaty,” according to its advocates, would allow for it to be more ambitious and have a broader scope compared to the IHR, and potentially greater influence on the actions of member states.
How has the U.S. government been involved in IHR negotiations?
The U.S., under the Biden administration, was actively engaged in the process to amend the IHR. The U.S. Department of Health and Human Services (HHS) Office of Global Affairs (OGA) led the U.S. delegation in the negotiations. Additionally, the U.S. served as one of the vice-chairs for the WGIHR meetings. At the start of the negotiation process, the U.S. submitted a number of proposed amendments along with many other countries, and has identified the top U.S. priorities:
- “clarify early-warning triggers” for health emergencies, including allowing for a tiered warning system instead of a simple binary PHEIC or no PHEIC decision,”
- “ensure rapid information sharing,”
- “improve WHO’s ability to use publicly available information to assess global health threats,” and
- “create a mechanism to improve implementation and compliance with the IHR.”
These priorities are reflected in the revisions in the revised IHR. For example, the Director-General of WHO can now declare a “pandemic emergency”, which is considered to be a higher level of emergency compared to other PHEICs. The revisions also include a section creating a new States Parties Committee and have a new requirement that member states designate a National IHR Authority to help support implementation.
How might U.S. obligations change and what concerns have been raised?
Under the revisions in the revised IHR, there would be little expected change in terms of U.S. obligations, save for designating a National IHR Authority (likely to be at HHS where the current National IHR Focal Point is located) and providing the required implementation updates to WHO. In the event of a future PHEIC, U.S. obligations under the revised IHR would include supporting international efforts by providing information regarding U.S.-based health products and R&D, engaging with “relevant stakeholders” to contribute towards equitable global access to health products, and voluntarily assisting in the mobilization of financial resources for responses to health emergencies in developing countries.
Some U.S. policymakers, and conservative policy initiatives such as Project 2025 initiative, raised concerns about the IHR negotiations and what a new agreement could mean for the U.S. Below are the main issues that have been raised, and available evidence regarding these concerns:
- Concerns about how the IHR might impact U.S. sovereignty. Concerns have been raised about how the revisions to the IHR might impact U.S. sovereignty, such as requiring the U.S. to take certain actions during public health emergencies and that WHO or other multilateral organizations would have greater authority to ensure implementation of the IHR. The U.S. delegation to the WGIHR stated that they would not accept an agreement that in any way undermined U.S. sovereignty. Additionally, the WHO does not have authority or enforcement mechanisms to dictate countries’ domestic policies. Further, in the draft text, the States Parties Committee serves in a “non-punitive” manner and provide recommendations for country compliance, rather than serve as an enforcement mechanism. Lastly, one of the principles of the IHR acknowledges countries’ “sovereign right to legislate and to implement legislation in pursuance of their health policies.” This principle has not been changed in the draft revision.
- Concerns around the requirements to share health data and the potential impact on individuals’ privacy. Some raised concerns that a revised IHR could require additional health data sharing and negatively impact individuals’ privacy. The 2005 version of the IHR provides safeguards for the processing of individuals’ personal data, including keeping data confidential and anonymous, and requiring states to only keep individuals’ personal data for as long as necessary. Additionally, travelers must explicitly consent to providing their individual health data if required by another state party for entry. These requirements are not changed in the updated IHR.
- Concerns about transparency of the WGIHR process and worry that parties were not provided enough information about IHR amendments before governments voted on the revised version at the WHA. Concerns were raised that the WGIHR had not been transparent enough throughout the negotiating process, and that parties outside the negotiating rooms had not been able to see the package of amendments to be voted on with enough advance notice. While some WGIHR sessions were webcast and meeting materials made public, much of the negotiations did indeed take place in closed-door sessions among member states, and negotiating texts were released to the public infrequently, which made it a challenge for outside parties to track developments closely. Another concern raised is that according to the current IHR, member states were to have at least four months advance notice prior to voting on proposed amendments to the agreement. This requirement was met, however, because a full list of proposed amendments from member states was made available in 2022 and proposed revisions draw from this list; WGIHR negotiations focused on narrowing the set of amendments to be considered, and clarifying the exact language for inclusion in the revised agreement.
In addition to specific concerns raised about the IHR and the new revisions, some policymakers and stakeholders have called for broader reforms to the WHO following the COVID-19 pandemic. These calls for reform cite concerns related to WHO’s transparency and effectiveness, including WHO’s ability to promptly respond to conduct investigations and promptly respond to potential public health emergencies. Some policymakers have stated that the U.S. should focus on efforts to reform the WHO before adopting additional international agreements.
The outcome of the upcoming Presidential election will have significant implications for U.S. involvement with the WHO. If President Trump is re-elected, he may seek to initiate U.S. withdrawal from the WHO as he did in his last presidential term. If the U.S. were to withdraw from the WHO, this would have implications for the U.S.’s role in the governance of the WHO, as the U.S. currently serves as a member of the Executive Board. Additionally, a withdrawal may impact U.S. participation in the IHR.
What are the next steps for the IHR?
With countries approving a final set of IHR revisions on June 1, 2024, the updated text has now been formally adopted by WHO member states. The revisions do not take effect immediately, however, but will instead take effect according to an agreed upon timetable (expected to be two years after their recent approval).
The revision does not require further Congressional approval or ratification in the U.S. The U.S. can lodge reservations to the IHR revision (all member states have 18 months from time of approval to register reservations). The U.S. has frequently lodged reservations with international agreements and did so with the previous 2005 revision of the IHR.
Endnotes
The WHO has 194 member states, which includes all UN member states except Liechtenstein, as well as the Cook Islands and Niue. The IHR has 196 “states parties” which include the 194 WHO member states plus “observers” Liechtenstein and the Holy See. In the brief we use the terms “member states” and “parties” interchangeably to refer to the 196 governments for which IHR obligations apply. However, as observers Liechtenstein and the Holy See do not have voting power at WHO.