Health Policy is Partisan, But It’s Also Personal
 It makes sense if you think about it for a second. The three big health care programs—Medicaid, Medicare, and the Affordable Care Act (ACA)—provide popular benefits valued by Americans from across the political spectrum, even as debate about policy proposals to “reform” them can be sharply polarized. If any of the big policy ideas percolating now just beneath the surface in think tanks and in the campaign make it to legislation in a new Congress, they will spark hotly contested legislative debates. People will react as partisans and take cues from their partisan representatives, as always. But they will also react as beneficiaries and consumers and patients, worried most about the impact legislation will have on them and their families. When it comes to basic questions like whether their premium will go up or down, or their cost sharing, or whether they will lose their coverage, people (and voters as the 2026 midterms loom) may be less partisan and more focused on their benefits and their pocketbooks.
It makes sense if you think about it for a second. The three big health care programs—Medicaid, Medicare, and the Affordable Care Act (ACA)—provide popular benefits valued by Americans from across the political spectrum, even as debate about policy proposals to “reform” them can be sharply polarized. If any of the big policy ideas percolating now just beneath the surface in think tanks and in the campaign make it to legislation in a new Congress, they will spark hotly contested legislative debates. People will react as partisans and take cues from their partisan representatives, as always. But they will also react as beneficiaries and consumers and patients, worried most about the impact legislation will have on them and their families. When it comes to basic questions like whether their premium will go up or down, or their cost sharing, or whether they will lose their coverage, people (and voters as the 2026 midterms loom) may be less partisan and more focused on their benefits and their pocketbooks.
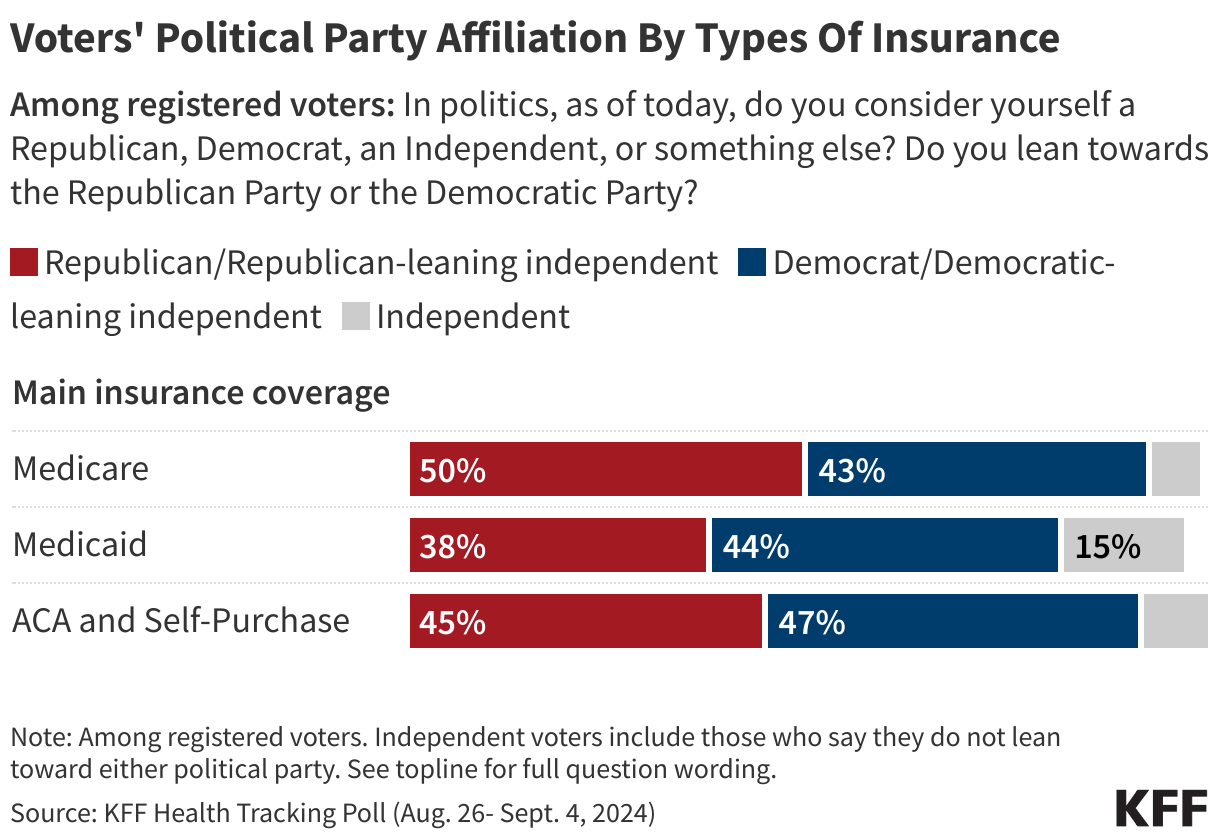
We usually look at Medicare, Medicaid, and ACA enrollees by income, race, or age ranges. We don’t usually think about their partisan makeup. The graphic shows what that looks like. As you might expect, these proposals would affect significant numbers of people from both parties as well as many Independents. More than 50 million Republicans and a similar number of Democrats are represented in the three bars in the graphic (which doesn’t capture family members on the programs).
Imagine legislative debates about such sweeping ideas as converting Medicare to a voucher-like premium support program, block granting Medicaid and significantly cutting federal funding, imposing lifetime limits on Medicaid eligibility, or perhaps the hottest one of all—replacing protections for the 56 million people with pre-existing conditions with some other approach that may or may not work as well for sick people—a proposal implied by comments made by Senator JD Vance. Some of the ideas that could emerge during a Harris administration could also spark big debates, such as making the enhanced ACA premium subsidies permanent. About 20 million people benefit from the enhanced premium subsidies. Republicans in Congress oppose doing this even as a lot of Republicans in states like Texas and Florida could face higher health insurance costs or find their coverage unaffordable if the enhanced subsidies go away.
If these policy ideas make it to legislative form after the election the one question voters will want an answer to above all others is: “What will this mean for me and my family?”. Many will hold their representatives responsible for the impact legislation has on them. Polling about these ideas will change once the arguments for and against them start to fly in a real-world debate and on TV ads, and consequences become more clear.
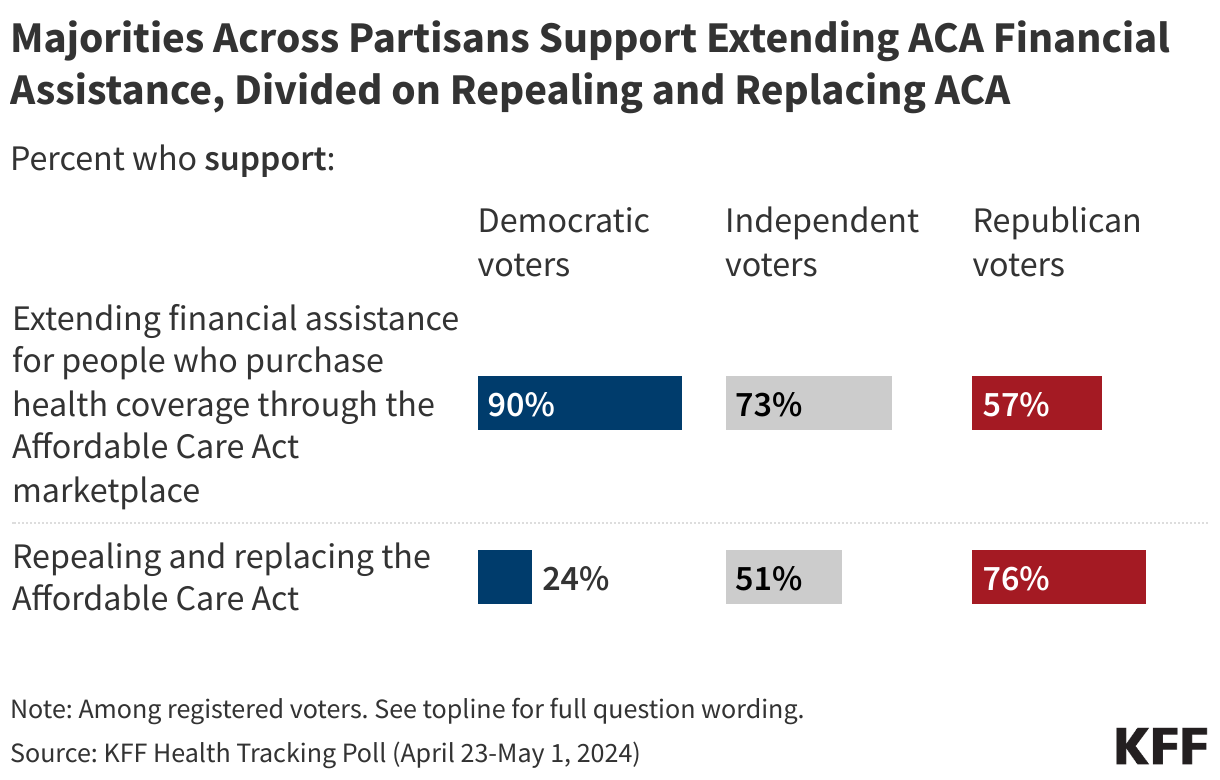
We can’t know for sure what will happen if self-interest collides with ideological predisposition and partisan affiliation for some voters. And the American people are capable of holding all kinds of conflicting views at the same time. For example, Republicans benefiting from the ACA enhanced premium subsidies could oppose discontinuing them while still supporting ACA repeal (not making the connection and still treating the ACA as a symbol of big government, President Obama, and liberalism they are conditioned to oppose even as they like specific ACA benefits). We saw exactly this in one of our recent tracking polls.
As is inevitable with any major piece of health policy legislation, some people will be better off, but others will be worse off. That tradeoff is inherent in risk pooling, where the healthy pay somewhat more so the sick can pay less, ensuring their own lower rates if they too become sick someday. But it’s often the case that the losers from a policy change scream louder than the winners, especially on such a personal issue as health care, and the media takes notice. A small number of losers can smear a policy even if there are many more winners.
The Congressional Budget Office focuses mainly on the impact of legislation on the federal budget, not people. That means a lot depends on how the media disentangles the impact of legislative proposals for the public, and the record on that is mixed (it’s not a “he said, she said” exercise, nor does it lend itself to panels of pundits). This is also a challenge for a few organizations like ours, which are in the business of determining the impact of health policy legislation on people.
When—or if—debate moves from think tank proposals and campaign talking points to legislation after the election, voters may become self-interested consumers as well as partisans.