Medicaid Expansion is a Red and Blue State Issue
Although health care did not figure prominently in the 2024 presidential election, with President-elect Trump returning to the White House and Republicans controlling Congress, significant changes to Medicaid are expected. One potential target for federal spending reductions is the Affordable Care Act’s (ACA) Medicaid expansion. The ACA expanded Medicaid coverage to nearly all adults with incomes up to 138% of the Federal Poverty Level ($20,783 for an individual in 2024) and now provides states with an enhanced federal matching rate (FMAP) of 90% for their expansion populations. While the expansion was originally mandatory for states, a Supreme Court decision in 2012 effectively made it optional and as of November 2024 all but 10 states have adopted the expansion. Twelve states have “trigger” laws in place that would automatically end expansion or require other changes if the federal match rate were to drop below 90%.
Rather than repealing the ACA outright, some conservative and Republican proposals would instead lower the federal match rate for the expansion population from 90% to the standard Medicaid match rate, which is calculated based on a state’s per capita income and ranges from 50% to 83%. The Congressional Budget Office estimated in 2022 that reducing the match rate for the expansion group would save the federal government $631 billion over 10 years. This financing change would shift a substantial amount of Medicaid spending from the federal government to states. States would then need to decide whether to use states funds to make up for the lost federal funding or cut coverage. Given the challenges states would face replacing substantial lost federal funds, the health coverage implications would likely be significant and could reverse gains in financial security, access to care, and health outcomes. A large body of prior research shows that Medicaid expansion has helped to reduce the uninsured and improve access, affordability, and financial security among the low-income population. More recent research shows improvements in health outcomes and continues to show positive effects for providers (particularly rural hospitals) and for sexual and reproductive health.
Because of the widespread adoption of the Medicaid expansion across states, the financial and coverage impacts will be felt by both states that voted for President-elect Trump and those that voted for Vice President Harris. This data note provides key facts on the Medicaid expansion using enrollment data as of March 2024 and FY 2023 spending data from the Medicaid Budget and Expenditure System (MBES).
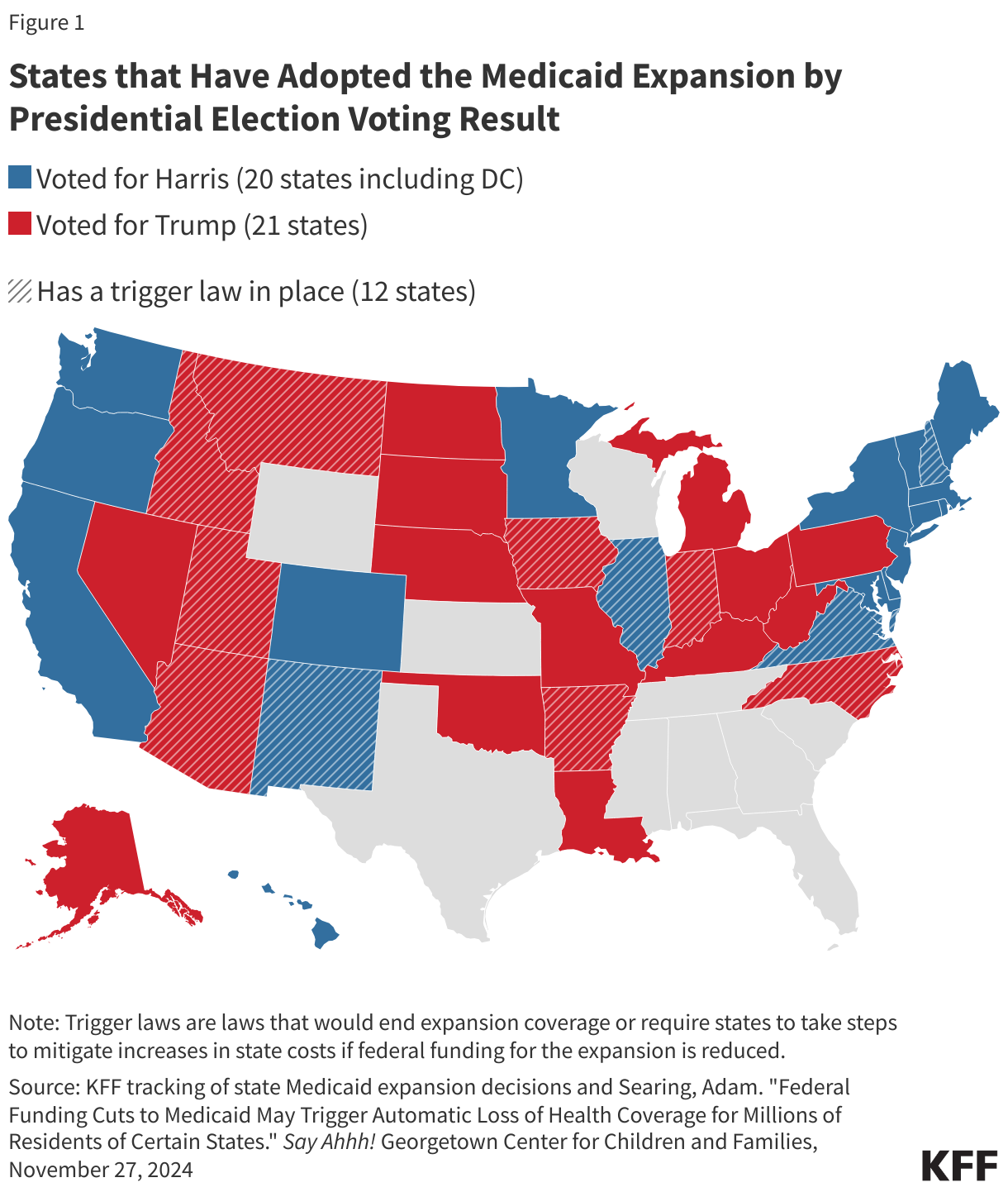
Medicaid expansion has been adopted by 41 states including the District of Columbia, split nearly evenly between states that voted for Trump (21 states) and those that voted for Harris (20 states) (Figure 1). Over the past ten years, Medicaid expansion has been broadly adopted by states led by Republicans and Democrats. Consequently, any changes to the Medicaid expansion authority or financing structure will affect both red and blue states. While the data are presented by states that voted for Trump or Harris in the November 2024 elections, there are five states with Democratic governors that voted for Trump (Arizona, Kentucky, Michigan, North Carolina, and Pennsylvania) and three Republican-led states that voted for Harris (New Hampshire, Virginia, and Vermont). In total, there are 19 expansion states with Republican governors, and 22 expansion states (including DC) headed by Democrats. Ultimately, it will be state governors and legislatures that will respond to any federal policy changes.
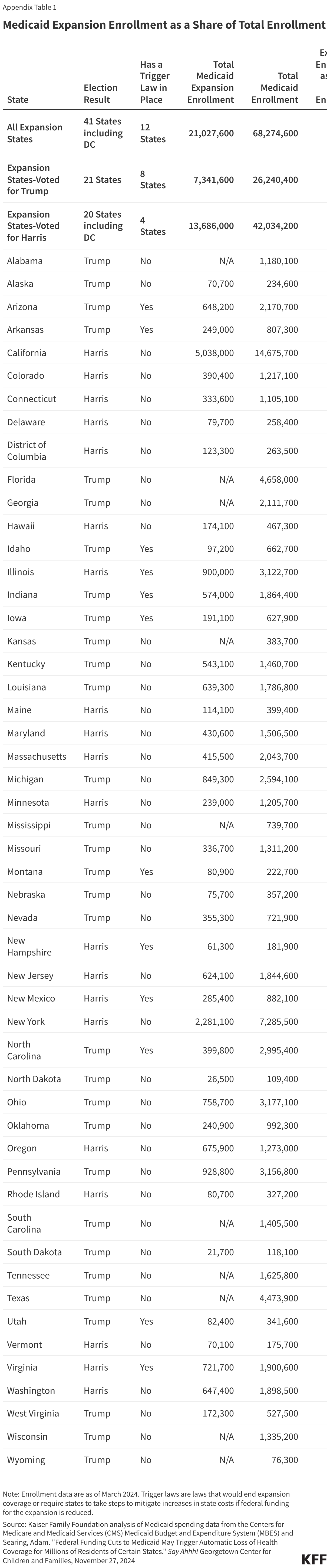
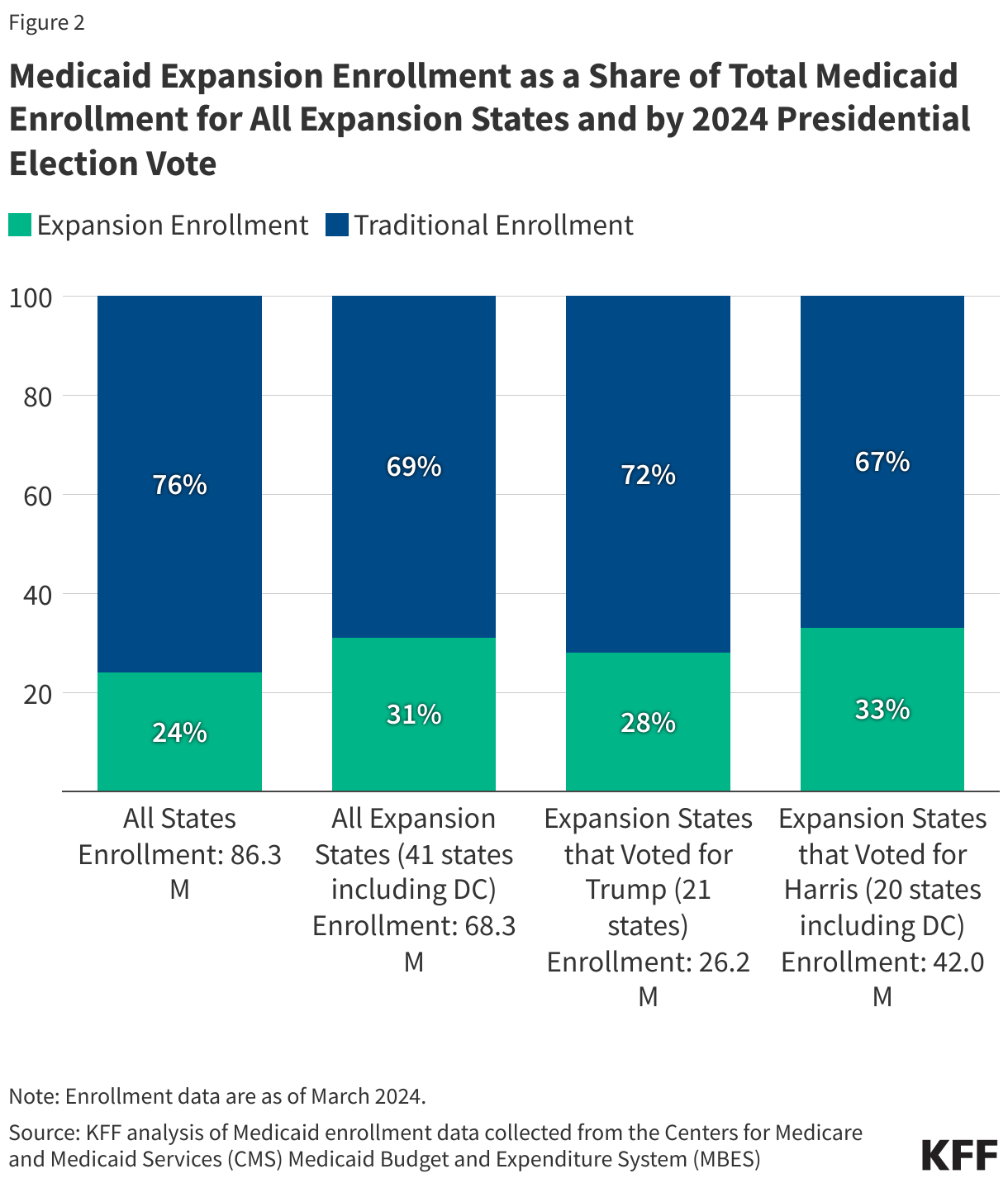
As of March 2024, over 21 million people were enrolled through the Medicaid expansion representing nearly a quarter of enrollment across all states and about three in ten Medicaid enrollees in expansion states (Figure 2). Medicaid expansion enrollment totaled 7.3 million in states that voted for Trump and 13.7 million in states that voted for Harris. Across all Medicaid expansion states, total Medicaid enrollment was 68.2 million and the majority of people (69%) were enrolled through traditional eligibility pathways. Medicaid expansion enrollment comprised a slightly larger share of enrollment in states that voted for Harris (33%) than in states that voted for Trump (28%). Expansion enrollment ranged from a high of 53% of total enrollment in Oregon to a low of 13% in North Carolina, which implemented Medicaid expansion coverage in December 2023 (Appendix Table 1). The variation across expansion states likely reflects several factors, including different poverty distributions and economic conditions across states as well as variation in state Medicaid eligibility levels for expansion and traditional groups.
About 4.3 million expansion enrollees live in states with some type of trigger law that would end expansion coverage or require review of expansion coverage to mitigate increases in state costs if federal funding for the expansion is reduced. Trigger laws require states to automatically end Medicaid expansion coverage or require them to take actions to ensure state costs do not increase if the federal matching rate for the Medicaid expansion drops below 90% or below a specified threshold. Not all of the laws would immediately end the Medicaid expansion, but enrollees in states with trigger laws are at greater risk of losing coverage, although some may be able to maintain coverage through other eligibility pathways in some states. Currently, nine states (Arizona, Arkansas, Illinois, Indiana, Montana, New Hampshire, North Carolina, Utah, and Virginia) have laws that require termination of the expansion if the share of federal funding drops. Laws in three additional states (Idaho, Iowa, and New Mexico) require the states to take some action to mitigate the fiscal impact of the loss of federal funds. Of the 12 states with trigger laws, eight states voted for Trump (Arizona, Arkansas, Idaho, Indiana, Iowa, Montana, North Carolina, and Utah) and four states voted for Harris (Illinois, New Hampshire, New Mexico, and Virginia). While laws in the so-called “trigger” states require action, the substantial loss of federal funding would likely force all states to reassess whether to continue the expansion coverage.
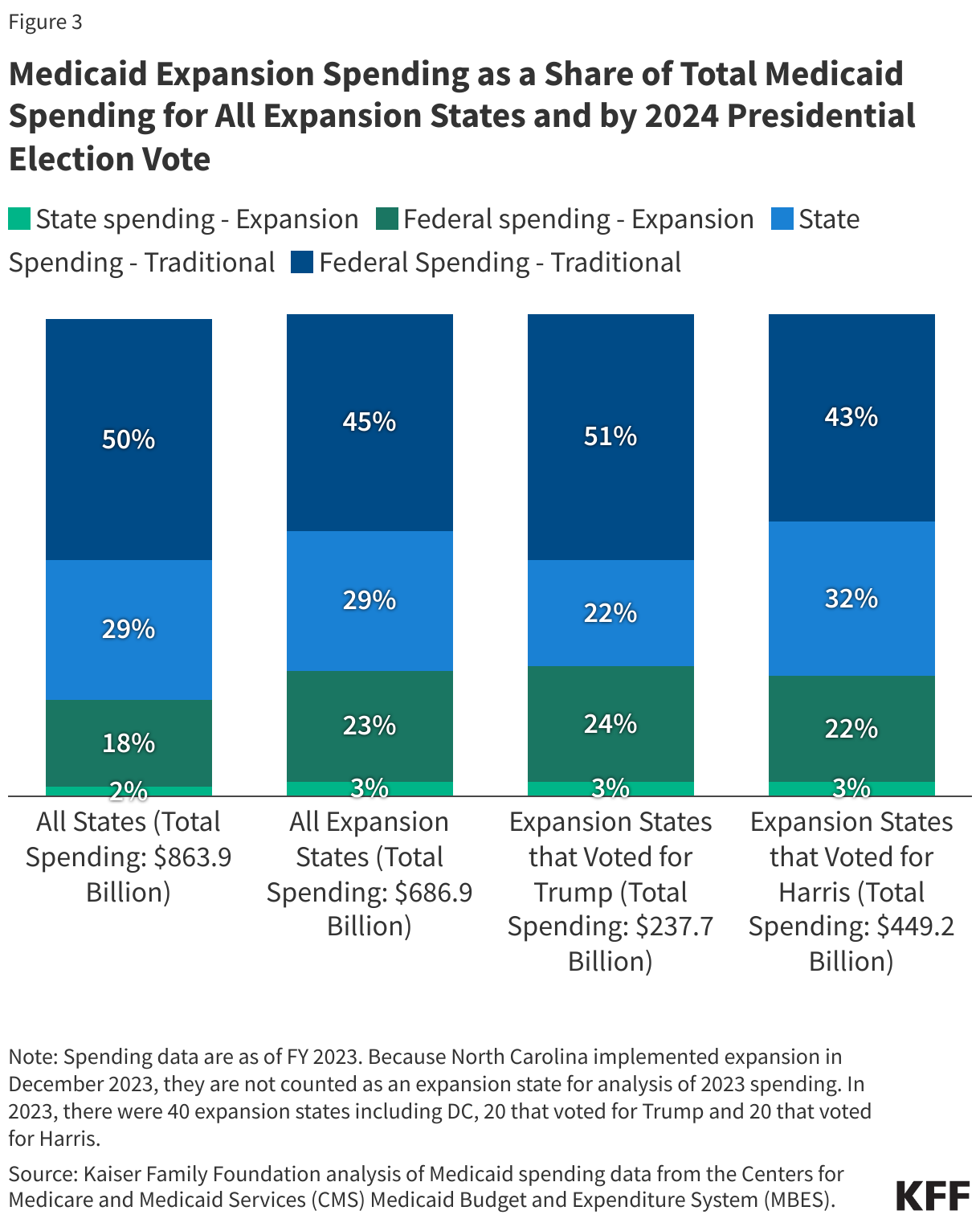
In FY 2023, spending on the expansion group represented 20% of Medicaid spending across all states and over a quarter of Medicaid spending in expansion states (Figure 3). Medicaid spending totaled $863.9 billion for all states and $686.9 billion in the 40 states that had implemented expansion in 2023 (North Carolina did not implement expansion until December 2023 and, consequently, is not counted as an expansion state during FY 2023). Spending on the expansion group totaled $178.2 billion, or 26% of total Medicaid spending in those states, and federal spending was $158.3 billion. Due to the 90% federal match for expansion, federal spending represents a larger share of spending for the expansion group than for traditional enrollees. The share of spending for the expansion group is lower than its share of enrollment (26% vs. 31%), in part, because the traditional Medicaid group includes populations such as those with disabilities and seniors who have higher per-enrollee spending. Similar to enrollment, expansion spending as a share of total spending varied across states from a high of 43% in Montana to a low of 16% in Massachusetts (Appendix Table 2).
Appendix Tables