Getting into Gear for 2014: Shifting New Medicaid Eligibility and Enrollment Policies into Drive
New Options to Facilitate Enrollment and Renewal
To facilitate processing applications for large numbers of people who become newly eligible for Medicaid on January 1, CMS has offered states five strategies to help manage the transition. Highlighted in a May 17, 2013 letter to state officials,1 these approaches are intended to promote enrollment and retention, while smoothing the administrative burden as states shift to new eligibility processes. A state may adopt any of these facilitated enrollment approaches regardless of whether it plans to implement the Medicaid expansion, and as of October 1, a number of states have taken up at least one of these options (Figure 10 and Appendix Table 9).
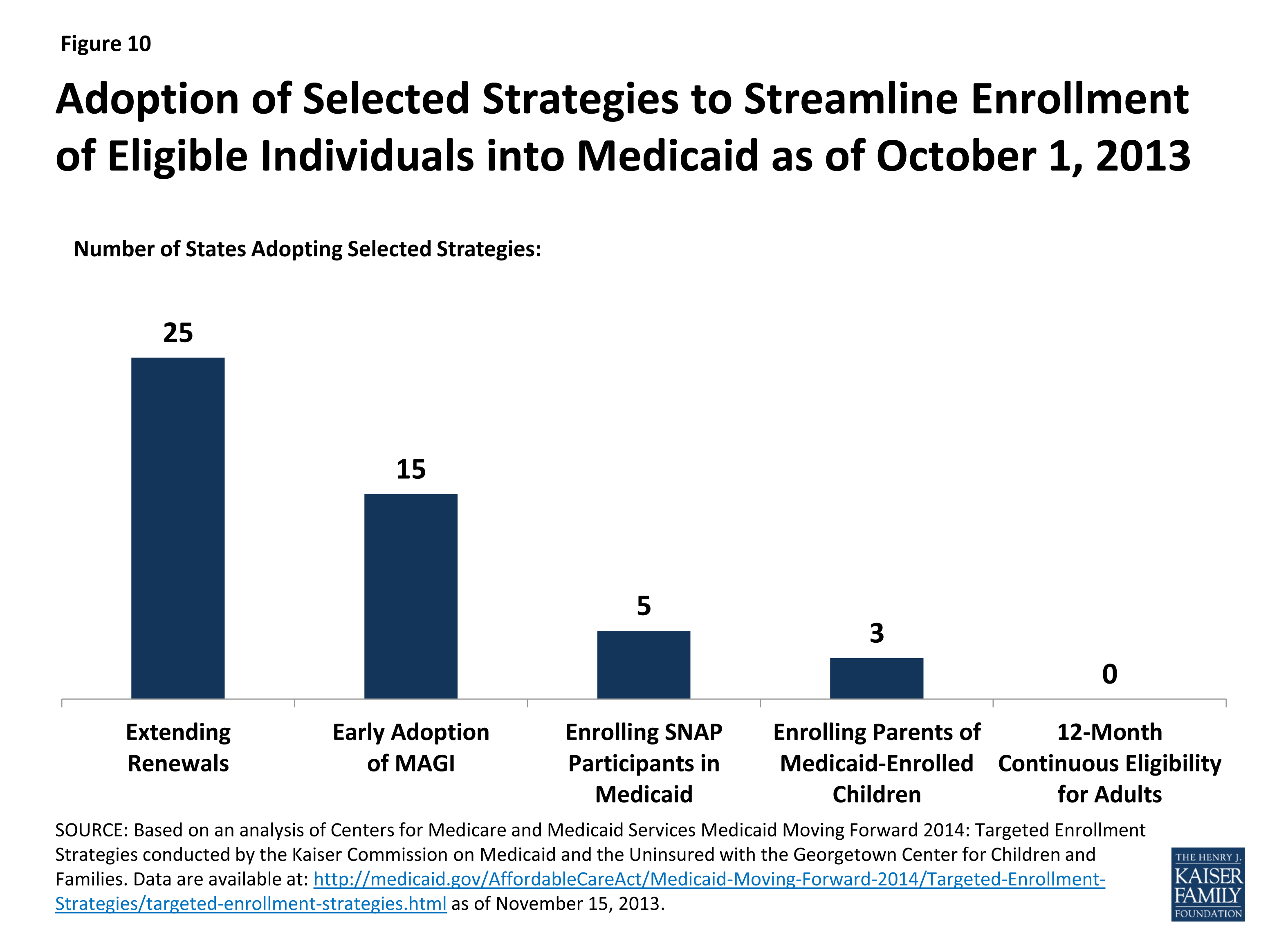
Figure 10: Adoption of Selected Strategies to Streamline Enrollment of Eligible Individuals into Medicaid as of October 1, 2013
Overall, 30 states have adopted at least one of the strategies, and 11 have adopted two or more of these approaches. Three (3) states (NJ, OR, and WV) have adopted four of the five. These strategies include:
- Extending Renewal Periods. The ACA protects individuals currently enrolled in Medicaid from losing coverage solely as a result of the conversion to MAGI-based eligibility until March 31, 2014 or their next renewal date (whichever is later). To abide by this provision, states would need to apply both the new MAGI rules and the existing rules to determine eligibility for those whose coverage is up for renewal between before March 31, 2014. To avoid this duplication of effort, CMS offered states the option to extend renewal dates beyond this three-month transition period and begin applying only MAGI-based eligibility rules to all regularly scheduled renewals beginning on April 1, 2014. States have flexibility to structure how the delays will take place, for example, by delaying renewals for 90 days, as long as they establish a reasonable timeframe within which the renewals will be completed. Twenty-five (25) states have taken up this strategy, many adopting it over a longer timeframe than those scheduled for the first quarter of 2014.
- Early Adoption of MAGI Eligibility. Through the initial months of open enrollment (October through December 2013), all individuals applying for or renewing Medicaid/CHIP coverage should have their eligibility determined under existing rules and also be assessed for eligibility using the new MAGI-based methodologies to determine if they will be eligible for coverage as of January 1, 2014. To avoid having to utilize two sets of eligibility rules, and possibly two different eligibility systems during this time, CMS offered states the option to adopt the MAGI methodology as of October 1 for all eligibility determinations going forward, which 15 states accepted.2
- Enrolling Eligible Supplemental Nutrition Assistance Program (SNAP) Participants in Medicaid. This temporary option is available to states through the end of 2015, and allows them to use data available from SNAP (also known as food stamps) to enroll eligible participants in Medicaid. To qualify for SNAP, a household’s gross income cannot generally exceed 130 percent of the FPL, which aligns well with the new Medicaid threshold of 138 percent of the FPL, although states may use this option for a subset of SNAP participants. Because SNAP enrollment data include verified information for many of the criteria necessary to determine Medicaid eligibility, a state can use that information along with a signed letter or phone call as a Medicaid application and enroll individuals once certain non-financial information, including citizenship or immigration status, is verified. Five (5) states (AR, IL, NJ, OR, and WV) have adopted this approach.
- Enrolling Parents in Medicaid Based on their Children’s Eligibility Data. In 2010, 3.5 million uninsured parents who could gain Medicaid coverage under the ACA expansion already had a child who was enrolled in Medicaid or CHIP.3 CMS offered states a temporary opportunity to expedite the enrollment of these parents. States can adopt this option by reactivating recent parent applications that have been denied or by reviewing children’s cases to identify eligible parents and requesting any additional information needed to make an eligibility determination. States may also send parents a pre-populated application or ask for additional information from the parent on the child’s renewal form. Three (3) states (NJ, OR, and WV) have moved forward with this approach.
- 12-Month Continuous Eligibility for Parents and Other Adults. States have long had the option to provide 12-month continuous eligibility for children regardless of certain changes in family circumstances, including fluctuations in income. Almost half of states (23) have adopted this option in Medicaid, strengthening the continuity of care and promoting ongoing coverage of children. CMS has offered to extend this effective retention strategy to adults and is working on implementation details.4
Two of these strategies, enrolling eligible SNAP participants and enrolling parents based on their children’s eligibility data, allow states to get a jump-start on their Medicaid expansions by significantly streamlining the process and utilizing data already available to states. Experiences in the four states that have already launched these strategies indicate they can be highly successful in connecting people to coverage, reaching a significant share of adults eligible for the Medicaid expansion while minimizing burdens for both eligibility staff and individuals and reducing traffic through enrollment systems. Overall, in these four states, over 223,000 individuals have been enrolled through these strategies as of November 15, 2013.5