Medicare Part D: A First Look at Medicare Prescription Drug Plans in 2022
During the Medicare open enrollment period from October 15 to December 7 each year, beneficiaries can enroll in a plan that provides Part D prescription drug coverage, either a stand-alone prescription drug plan (PDP) as a supplement to traditional Medicare, or a Medicare Advantage prescription drug plan (MA-PD), which covers all Medicare benefits, including drugs. In 2021, 48 million Medicare beneficiaries, or more than three-quarters (77%) of all Medicare beneficiaries, are enrolled in Medicare Part D plans, with half (50%) enrolled in stand-alone PDPs and the other half (50%) enrolled in Medicare Advantage drug plans. This issue brief provides an overview of the Medicare Part D marketplace in 2022 and key trends over time, focusing primarily on stand-alone PDPs. (A separate overview of the 2022 Medicare Advantage market is also available.) Unless otherwise noted, weighted estimates are based on August enrollment (see Methods box for additional details).
Highlights for 2022
- The average Medicare beneficiary has a choice of 54 Medicare plans with Part D drug coverage in 2022, including 23 Medicare stand-alone drug plans and 31 Medicare advantage drug plans.
- A total of 766 Medicare Part D stand-alone prescription drug plans will be offered in 2022, a 23% decrease from 2021, primarily the result of consolidations of PDP offerings sponsored by Cigna and Centene resulting in three fewer PDPs from each firm in each region.
- The estimated average monthly premium for Medicare Part D stand-alone drug plans is projected to be $43 in 2022, based on current enrollment, while average monthly premiums for the 16 national PDPs are projected to range from $7 to $99 in 2022. Among the 16 national PDPs, average monthly premiums are increasing for 12 PDPs, including 5 PDPs with increases exceeding $10.
- Most Part D PDP enrollees who remain in the same plan in 2022 will be in a plan with the standard (maximum) $480 deductible.
- Most PDP enrollees will face much higher cost sharing for brands than for generic drugs, including coinsurance for non-preferred drugs between 40% and 50% (the maximum coinsurance rate allowed for the non-preferred drug tier) in 12 of the 16 national PDPs.
- In 2022, 198 PDPs will be premium-free for enrollees receiving the Low-Income Subsidy (LIS) (benchmark plans), a smaller number than in any year since Part D started in 2006. The decrease between 2021 and 2022 is due to plan consolidations by Cigna and Centene, which offered benchmark PDPs in 2021 that will not be offered in 2022.
Part D Plan Availability
The Average Medicare Beneficiary Has a Choice of More Than 50 Medicare Plans with Part D Drug Coverage in 2022
The average Medicare beneficiary will have a choice of 23 stand-alone PDPs in 2022, 7 fewer PDP options than in 2021, a 24% decrease (Figure 1). Although the number of PDP options in 2022 is far lower than the peak in 2007 (when there were 56 PDP options, on average), beneficiaries in each state continue to have numerous stand-alone drug plan options.
In 2022, beneficiaries will also have access to 31 MA-PDs, on average, a 15% increase in MA-PD options since 2021. (This average excludes Medicare Advantage plans that do not offer the drug benefit; overall, an average of 39 Medicare Advantage plan options will be available in 2022, excluding plans not available to all beneficiaries, such as Special Needs Plans and group plans).
A Total of 766 Medicare Part D Stand-Alone Prescription Drug Plans Will Be Offered in 2022, a 23% Decrease From 2021 Primarily Due to Plan Consolidations
In 2022, a total of 766 PDPs will be offered by 16 firms in the 34 PDP regions (plus another 10 PDPs in the territories), a decrease of 230 PDPs (-23%) from 2021 (Figure 2). The relatively large decrease in the number of PDPs for 2022 is primarily the result of consolidations of plan offerings sponsored by Cigna and Centene resulting in the market exit of three national PDPs from each firm in each region (all three of Cigna’s Express Scripts PDPs and three of Centene’s six Wellcare PDPs). (Part D sponsors are limited to offering no more than three PDPs in each region.) This accounts for just over 200 PDPs offered in 2021 that will no longer be offered in 2022. Enrollees in these consolidated plans will be automatically switched to other plans offered by the same plan sponsor, although they can choose to switch into a different plan during the annual open enrollment period.
Despite the reduction in PDP availability for 2022, beneficiaries in each state will have a choice of multiple stand-alone PDPs, ranging from 19 PDPs in New York to 27 PDPs in Arizona, plus multiple MA-PDs offered at the local level (Figure 3, Table 1).
The number of firms sponsoring stand-alone drug plans has declined steadily over time, from more than 40 firms in 2010 and earlier years, dropping below 25 firms beginning in 2015, and at 16 firms in 2022, is lower than in any other year since Part D started. PDP enrollment is expected to be concentrated in a small number of firms in 2022, as it has been every year. Based on August 2021 enrollment, 8 out of 10 PDP enrollees (80%) in 2022 are projected to be in PDPs operated by just four firms: CVS Health, Centene, UnitedHealth, and Humana. All four firms offer PDPs in all 34 PDP regions in 2022.
Availability of Insulin Demonstration Plans
In 2022, beneficiaries in each state will have the option to enroll in a Part D plan participating in an Innovation Center model in which enhanced drug plans cover insulin products for non-LIS enrollees at a monthly copayment of $35 in the deductible, initial coverage, and coverage gap phases of the Part D benefit. In 2022, a total of 2,159 Part D plans will participate in this model (a 32% increase over 2021, including 258 PDPs (33% of all PDPs) and 1,901 MA-PDs (38% of MA-PDs, including segmented plans). Between 7 and 10 PDPs in each region are participating in the model, in addition to multiple MA-PDs (Table 1). Based on August 2021 enrollment, 45% of non-LIS enrollees are in PDPs that will participate in the insulin model in 2022.
Part D Premiums
Average Monthly Premiums for the 16 National PDPs Are Projected to Range from $7 to $99 in 2022
The estimated national average monthly PDP premium for 2022 is projected to be $43, a 15% increase from $38 in 2021, weighted by August 2021 enrollment (Table 2). It is likely that the actual average weighted premium for 2022, after accounting for enrollment choices by new enrollees and plan changes by current enrollees, will be lower than this estimated average. CMS reported that the average premium for basic Part D coverage offered by PDPs and MA-PDs will be an estimated $33 in 2022. Our premium estimate is higher because it is based on PDPs only (excluding MA-PDs) and includes PDPs offering both basic and enhanced coverage (enhanced plans, which account for 60% of all PDPs in 2022, have higher premiums than basic plans, on average).
PDP premiums will vary widely across plans in 2022, as in previous years. Among the 16 PDPs available nationwide, average premiums will range from a low of $7 per month (or $85 annually) for SilverScript SmartRx to a high of $99 per month (or nearly $1,200 annually) for AARP MedicareRx Preferred (Figure 4, Table 2). In other words, among the 16 national PDPs, there is an $1,100 difference in annual premiums between the highest-premium PDP and the lowest-premium PDP.
Changes to premiums from 2021 to 2022, averaged across regions and weighted by 2021 enrollment, also vary widely across PDPs, as do the absolute amounts of monthly premiums for 2022. Among the 16 national PDPs, average monthly premiums are increasing for 12 PDPs, including 5 PDPs with increases exceeding $10: Wellcare Medicare Rx Value Plus (+$23, a 52% increase), Cigna Extra Rx (+$21, a 54% increase), Cigna Essential Rx (+$12, a 49% increase), Humana Premier Rx Plan (+$12, an 18% increase), and AARP Medicare Rx Preferred (+$11, a 12% increase).
Monthly premiums are increasing in 2 of the top 3 PDPs by enrollment:
- The 1.6 million non-LIS enrollees in the largest PDP, CVS Health’s SilverScript Choice (which has a total of 3.4 million enrollees in 2021, including those receiving low-income subsidies) will see a $3 increase (+9%) in their average monthly premium, from $28 in 2021 to $31 in 2022.
- The 1.6 million non-LIS enrollees in the second largest PDP, AARP MedicareRx Preferred, will see an $11 increase (+12%) in their average monthly premium between 2021 and 2022 from $89 to $99. This is the highest average monthly premium among the national PDPs in 2022. Part D enrollees who have been enrolled in AARP MedicareRx Preferred since 2016 and stay enrolled in 2022 will be paying nearly $40 more than in 2016, when the average monthly premium for this PDP was $61.
- The 1.6 million non-LIS enrollees in the third largest PDP, Wellcare Value Script, will see a $4 decrease (-25%) in their monthly premium, from $16 in 2021 to $12 in 2022.
Average Monthly Premiums Are Higher for PDPs Offering Enhanced Benefits, Including Insulin at a $35 Monthly Copay, and Lower or No Deductibles
Most Part D stand-alone drug plans in 2022 (60% of PDPs) will offer enhanced benefits for a higher average monthly premium, and most non-LIS PDP enrollees (72%) are enrolled in enhanced plans, based on August 2021 enrollment. Enhanced benefits can include a lower (or no) deductible, reduced cost sharing, or a higher initial coverage limit than under the basic benefit design. The average premium in 2022 for enhanced benefit PDPs is $51, which is 44% higher than the monthly premium for PDPs offering the basic benefit ($35). For the subset of enhanced PDPs participating in the $35 copay insulin model, the average monthly premium ($63) is nearly twice as high as the monthly premium for PDPs that are not participating in the model ($34) (Figure 5).
In 2022, most PDPs (82%) will charge a deductible, including 7 in 10 PDPs (71%) charging the standard (maximum) amount of $480 in 2022. Across all PDPs, the average deductible in 2022 will be $384. The average monthly premium in 2022 for PDPs that charge no deductible is $90, nearly three times the monthly premium for PDPs that charge the standard deductible ($33) and twice as much as the monthly premium for PDPs charging a partial deductible ($45).
Nearly Three-Fourths of Part D Stand-alone Drug Plan Enrollees Without Low-income Subsidies Will Pay Higher Premiums in 2022 If They Stay in Their Current Plan
Most Part D stand-alone plan enrollees – nearly 10 million of the 13.3 million Part D PDP enrollees who are responsible for paying the entire premium (which excludes Low-Income Subsidy (LIS) recipients) (73%) – will see their monthly premium increase in 2022 if they stay in their same plan, while 3.5 million (27%) will see a premium reduction if they stay in their same plan (Figure 6).
While the average weighted monthly PDP premium is increasing by $5 between 2021 and 2022 (from $38 to $43), nearly 4 million non-LIS enrollees (28%) will see a premium increase of $10 or more per month. Substantially fewer non-LIS enrollees (0.2 million, or 2%) will see a premium reduction of the same magnitude. More than one-third (35%) of non-LIS enrollees (4.7 million) are projected to pay monthly premiums of at least $60 if they stay in their current plans, including 1.3 million (9% of non-LIS enrollees) projected to pay monthly premiums of at least $100. This group includes enrollees in the AARP MedicareRx Preferred PDP in several regions, along with enrollees in several Blue Cross/Blue Shield PDPs and other PDPs that are offered in selected regions but not nationwide.
Part D Cost Sharing
Part D Enrollees Pay Much Higher Cost Sharing for Brands and Non-preferred Drugs Than for Generic-Tier Drugs, and a Mix of Copays and Coinsurance for Different Formulary Tiers
In 2022, as in prior years, Part D enrollees will face much higher cost-sharing amounts for brands and non-preferred drugs (which can include both brands and generics) than for drugs on a generic tier, and a mix of copayments and coinsurance for different formulary tiers. The typical five-tier formulary design in Part D includes tiers for preferred generics, generics, preferred brands, non-preferred drugs, and specialty drugs.
Among all PDPs, median standard cost sharing in 2022 is $0 for preferred generics and $5 for generics, $42 for preferred brands (an increase from $40 in 2021), 40% coinsurance for non-preferred drugs (the same as in 2021; the maximum allowed is 50%), and 25% coinsurance for specialty drugs (the same as in 2021; the maximum allowed is 33%) (Figure 7, Table 3).
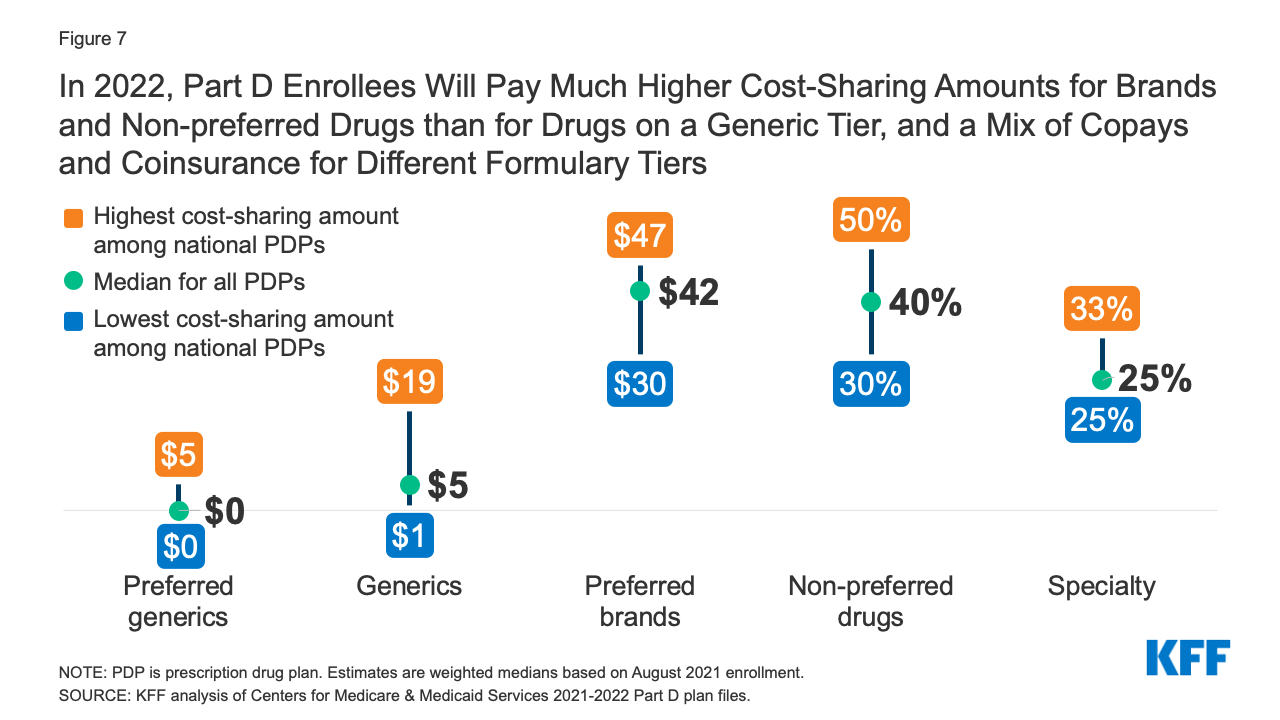
Figure 7: In 2022, Part D Enrollees Will Pay Much Higher Cost-Sharing Amounts for Brands and Non-preferred Drugs than for Drugs on a Generic Tier, and a Mix of Copays and Coinsurance for Different Formulary Tiers
Plans are implementing a mix of cost-sharing changes for 2022, with both increases and decreases in cost-sharing amounts on various formulary tiers. Of note, however, are cost-sharing increases for non-preferred drugs in 6 of the 16 national PDPs (while decreasing in only 2 of the 16). In 12 of the 16 national PDPs, coinsurance amounts for non-preferred drugs will range from 40% to 50% (the maximum allowed for this tier) in 2022. In addition, enrollees in the top PDP by enrollment, SilverScript Choice, will see their cost sharing for preferred brands shift from a $35 flat copayment to a 17% coinsurance rate, which could mean higher out-of-pocket costs for drugs priced over $206 per 30-day supply, since 17% of this amount or more would exceed the flat $35 copayment. And paying coinsurance rather than flat copayments makes it more difficult to know in advance what actual out-of-pocket costs will be, since that depends on the underlying list price of the drug.
Low-Income Subsidy Plan Availability
In 2022, a Smaller Number of Part D Stand-Alone Drug Plans Will Be Premium-Free to Enrollees Receiving the Low-Income Subsidy (Benchmark Plans) Than in Any Other Year
Through the Part D LIS program, enrollees with low incomes and modest assets are eligible for assistance with Part D plan premiums and cost sharing. As of March 2021, approximately 13 million Part D enrollees are receiving LIS, including 6.8 million (53%) in MA-PDs and 6.0 million (47%) in PDPs.
In 2022, a smaller number of PDPs will be premium-free benchmark plans – that is, PDPs available for no monthly premium to Medicare Part D enrollees receiving the Low-Income Subsidy (LIS) – than in any year since Part D started in 2006, with 198 premium-free benchmark plans, or roughly a quarter of all PDPs in 2022 (Figure 8). The reduction in benchmark plan availability between 2021 and 2022 is the result of plan consolidations by Cigna and Centene; one of Cigna’s Express Scripts PDPs and one of Centene’s Wellcare PDPs that will not be offered in 2022 were benchmark PDPs in all regions in 2021.
On average (weighted by Medicare enrollment), LIS beneficiaries have six benchmark plans available to them for 2022, which is about one-fourth the average number of PDP choices available overall and the lowest average number of benchmark plan options in any year since Part D started. All LIS enrollees can select any plan offered in their area, but if they enroll in a non-benchmark plan, they must pay some portion of their chosen plan’s monthly premium. In 2022, 13% of all LIS PDP enrollees who are eligible for premium-free Part D coverage (0.8 million LIS enrollees) will pay Part D premiums averaging $27 per month unless they switch or are reassigned by CMS to premium-free plans.
The number of benchmark plans available in 2022 will vary by region, from four to nine (Table 1). In 2022, 91% of the 6.0 million LIS PDP enrollees are projected to be in PDPs operated by five firms: CVS Health, Centene, Humana, UnitedHealth, and Cigna (based on August 2021 enrollment).
Discussion
Our analysis of the Medicare Part D stand-alone drug plan landscape for 2022 shows that millions of Part D enrollees without low-income subsidies will face premium and other cost increases in 2022 if they stay in their current stand-alone drug plan. There are somewhat fewer stand-alone PDP options available nationwide in 2022, but still dozens of drug plan choices available to beneficiaries in each area during this year’s open enrollment period, including both PDPs (23 plans, on average) and Medicare Advantage drug plans (31 MA-PD plans, on average). There are also fewer benchmark plan options for Part D enrollees receiving Low-Income Subsidies. A narrower set of benchmark plan options could make it more difficult for some LIS enrollees to find a premium-free plan that covers all their prescription medications.
Some Part D stand-alone drug plan enrollees who choose to stay in their current plans may see lower premiums and other costs for their drug coverage, but nearly three-fourths of non-LIS PDP enrollees will face higher premiums if they remain in their current plan, and many will also face higher deductibles and cost sharing for covered drugs. Most Part D PDP enrollees who remain in the same plan in 2022 will be in a plan with the standard (maximum) $480 deductible and will face much higher cost sharing for brands than for generic drugs, including as much as 50% coinsurance for non-preferred drugs. Some beneficiaries could see overall cost savings, including the monthly premium, deductible, and cost sharing, if they switched to a lower-premium plan, while for other beneficiaries, a higher-premium plan might better meet their needs at a lower overall total cost.
Despite these year-to-year changes in plan coverage and costs, as well as changes in beneficiaries’ health needs, other KFF analysis finds that most Medicare beneficiaries did not compare plans during a recent open enrollment period, and most Part D enrollees did not compare the coverage offered by their drug plan to other drug plans. Comparing and choosing among the wide array of Part D plans can be difficult, given that plans differ from each other in multiple ways beyond premiums, including cost sharing, deductibles, covered drugs, and pharmacy networks. Comparing Medicare Advantage drug plans may be made more difficult by the fact that not only drug coverage varies but also other features, including cost sharing for medical benefits, provider networks, and coverage and costs for supplemental benefits. Because Part D plans differ in several ways that can have a significant effect on an enrollee’s access to medications and out-of-pocket drug spending, all Part D enrollees could benefit from the opportunity to compare plans during open enrollment.
| Methods |
| This analysis focuses on the Medicare Part D stand-alone prescription drug plan marketplace in 2022 and trends over time. The analysis focuses on the 19.5 million enrollees in stand-alone PDPs, as of March 2021. The analysis excludes 21.3 million MA-PD enrollees (non-employer), and another 4.4 million enrollees in employer-group only PDPs and 2.8 million in employer-group only MA-PDs for whom plan premium and benefits data are unavailable.
Data on Part D plan availability, enrollment, and premiums were collected from a set of data files released by the Centers for Medicare & Medicaid Services (CMS):
In this analysis, premium and deductible estimates are weighted by August enrollment unless otherwise noted. Percentage increases are calculated based on non-rounded estimates and in some cases differ from percentages calculated based on rounded estimates presented in the text. |