COVID-19 Presents Significant Risks for American Indian and Alaska Native People
The COVID-19 emergency presents significant risks for the over 5 million individuals who self-identify as American Indian and Alaska Native (AIAN) alone or in combination with another race. AIAN people live across the country, but are concentrated in certain states, with roughly half living in seven states (CA, OK, AZ, TX, NM, WA, and NY). Under treaties and laws, the federal government has a unique responsibility to provide health care services to AIAN people. AIAN people face disproportionate risks from the COVID-19 outbreak given significant underlying disparities in health, social, and economic factors. Addressing their needs as part of COVID-19 response efforts will be key for preventing further widening of these disparities and fulfilling the federal government’s federal trust responsibility.
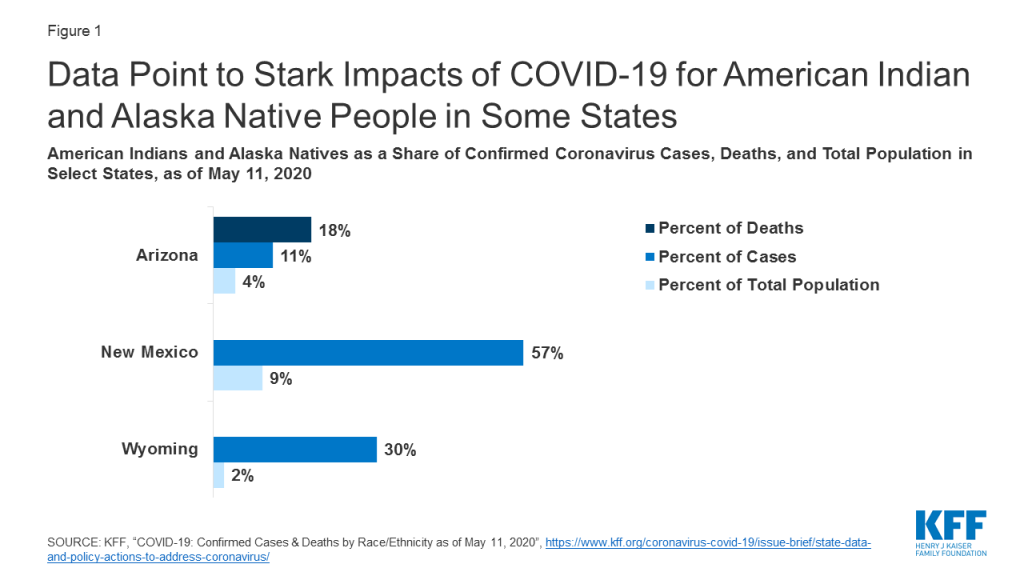
Data point to stark impacts of COVID-19 for AIAN people in some states. For example, as of May 11th, AIAN people made up 18% of deaths and 11% of cases compared to 4% of the total population in Arizona, 57% of cases compared to 9% of the total population in New Mexico, and 30% of cases compared to 2% of the total population in Wyoming, and (Figure 1). As of May 10th, the Indian Health Service (IHS) reported nearly 5,500 positive cases from IHS, Tribal, and urban Indian facilities, including over 3,300 among the Navajo Nation, which spans Arizona, New Mexico, and Utah.
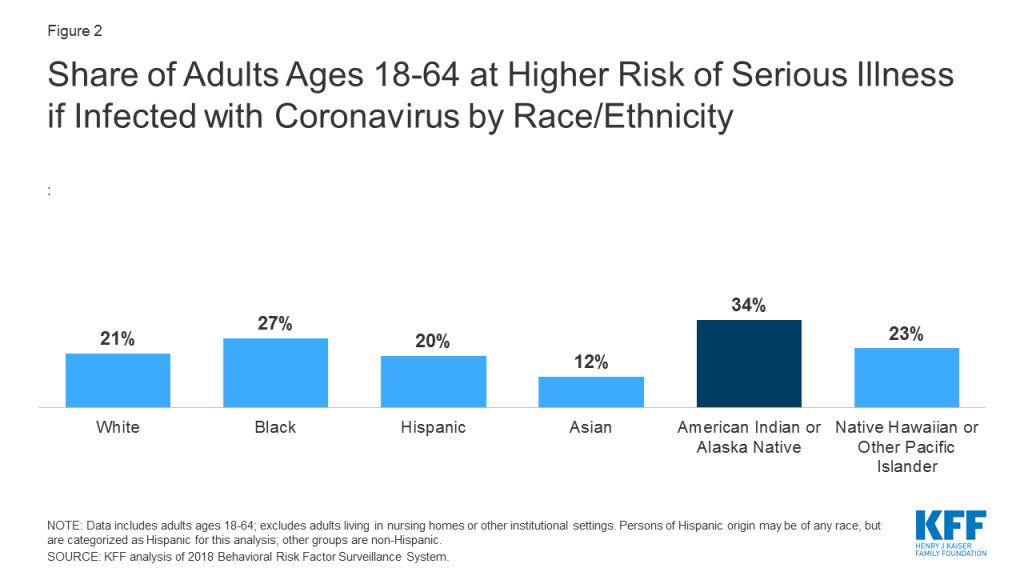
Coronavirus presents significant health risks for AIAN people because they face large underlying health disparities. AIAN people have disproportionately high rates of many health conditions that may put them at higher risk for serious illness if they contract coronavirus, including diabetes, heart disease, asthma, and obesity. Analysis examining how many adults are at higher risk for experiencing serious illness if they are infected with coronavirus based on CDC’s identified health risk factors finds that 34% of AIAN nonelderly adults are at risk of serious illness compared to 21% of White nonelderly adults (Figure 2). Living conditions also put AIAN people at increased risk for exposure to the disease. For example, compared to other groups, AIAN individuals are more likely to lack access to clean water and plumbing and to live in substandard and crowded housing situations, limiting the ability to practice frequent hand washing and social distancing.
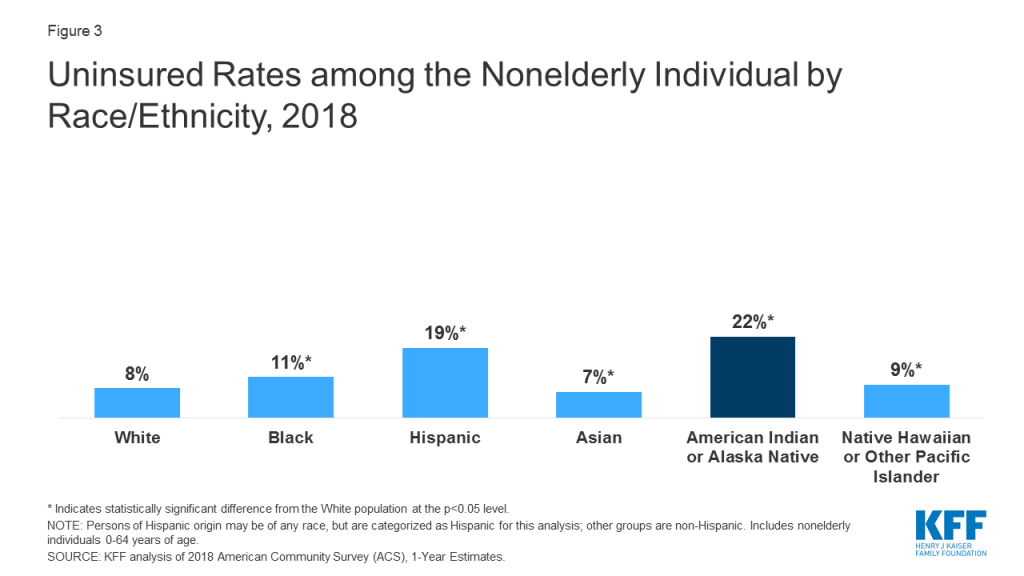
AIAN people face barriers to health care that may make it challenging to obtain coronavirus testing and treatment services. IHS is the primary vehicle through which the federal government fulfills its responsibility to provide health care services to AIAN people. However, IHS historically has been underfunded to meet their health care needs. Moreover, not all individuals who identify as AIAN are able to access services through IHS. IHS services generally are limited to members of or descendants of members of federally recognized Tribes. However, not all individuals who self-identify as AIAN belong to a federally recognized Tribe. Further, while many AIAN people live in rural areas, the majority live outside of Tribal areas, which can make it challenging to access an IHS provider. Give the limitations of IHS, Medicaid and other sources of health insurance remain important for expanding access to care for AIAN people. They also provide revenue that enhances capacity at IHS and Tribal facilities. However, as of 2018, 22% of AIAN nonelderly people were uninsured, the highest of all racial and ethnic groups (Figure 3). Reflecting the limitations of IHS and the high uninsured rate for AIAN people, they face increased challenges accessing care. For example, AIAN nonelderly adults are more likely compared to their White counterparts to have not seen a doctor in the past year due to cost (19% vs. 13%) and to have delayed care for other reasons (36% vs. 19%).
Coronavirus also may lead to disproportionate financial challenges for AIAN people. Over one in four (26%) nonelderly AIAN people have income below poverty, leaving them with limited ability to absorb income decreases that may result from the COVID-19 crisis. In addition, Tribes have lost key sources of revenue to support operations and services due to the halting of businesses and services in response to social distancing policies.
Addressing the needs of AIAN people as part of COVID-19 response efforts will be key to prevent further widening of their already large health and economic disparities and fulfilling the federal trust responsibility provide health care to AIAN people. The federal government has provided relief and support for federally recognized Tribes and Tribal business entities through the Coronavirus Aid Relief and Economic Security Act, including roughly $1 billion in additional IHS funding. Looking ahead, it will be important to assess the extent to which resources are adequate to address the needs of AIAN people and communities, including providing access to testing and treatment, support for health care providers, resources to mitigate risks associated with living conditions, culturally appropriate outreach and education, and financial relief. Moreover, comprehensive data will be key for understanding how the COVID-19 outbreak is affecting AIAN people, directing resources to meet needs, and measuring effects of response and relief efforts.