How Much Does Medicare Spend on Insulin?
The rising cost of prescription drugs is currently a major focus for policymakers. One medication that has come under increasing scrutiny over its price increases is insulin, used by people with both Type 1 and Type 2 diabetes to control blood glucose levels. Among people with Medicare, one third (33%) had diabetes in 2016, up from 18% in 2000. The rate of diabetes is higher among certain groups, including more than 40% of black and Hispanic beneficiaries. Although not all people with diabetes take insulin, for many it is a life-saving medication and essential to maintaining good health. Three companies—Eli Lilly, Novo Nordisk, and Sanofi—manufacture most insulin products, and there are no generic insulin products currently available, despite the fact that insulin was discovered in the 1920s. Committees in both the House and the Senate recently convened hearings on prescription drug costs that focused on rising insulin prices and affordability concerns for patients, and congressional investigations are underway.
This data note examines spending on insulin by Medicare and beneficiaries enrolled in private Part D drug plans, based on data from the Centers for Medicare & Medicaid Services (see Data and Methods). Because drug-specific rebate data for Medicare are proprietary, the analysis examines Medicare spending without rebates, but also uses average Part D rebates reported by Medicare’s actuaries to illustrate the potential effects on total Part D insulin spending. While rebates may help to lower Part D premiums, they do not lower enrollees’ out-of-pocket drug costs, which are based on list prices.
Key Findings
- Total Medicare Part D spending on insulin increased by 840% between 2007 and 2017, from $1.4 billion to $13.3 billion (Figure 1)—including what Medicare, plans, and beneficiaries paid.
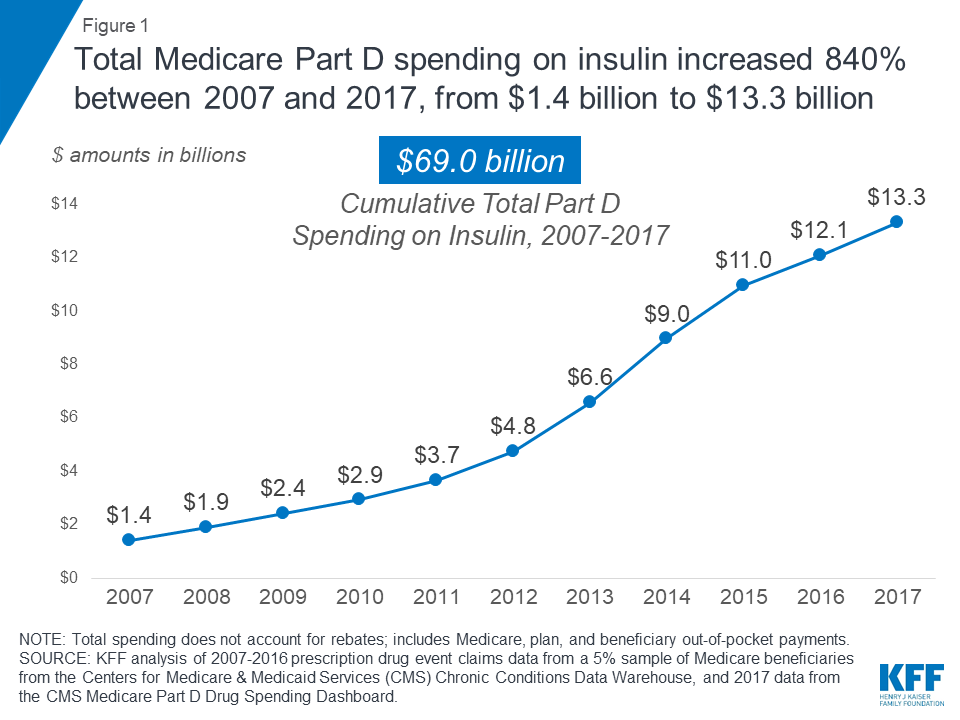
Figure 1: Total Medicare Part D spending on insulin increased 840% between 2007 and 2017, from $1.4 billion to $13.3 billion
- With rising prices and the introduction of more costly insulin products over time, average total Medicare Part D spending per user on insulin products increased by 358% between 2007 and 2016, from $862 to $3,949.
- Aggregate out-of-pocket spending by Part D enrollees on insulin quadrupled between 2007 and 2016, from $236 million to $968 million, reflecting both an increase in the number of users and price increases for insulin. Among enrollees without low-income subsidies, average per capita out-of-pocket spending on insulin nearly doubled between 2007 and 2016 (from $324 to $588; an increase of 81%).
- Among all insulin products, Lantus Solostar, a long-acting insulin manufactured by Sanofi, accounted for the largest share of both total Part D spending and out-of-pocket spending by enrollees who used insulin. Spending on Lantus Solostar, which was used by 1.1 million Part D enrollees in 2017, accounted for 20% of total Part D spending on insulin therapies in 2017 and 25% of out-of-pocket spending on insulin by non-low income subsidy enrollees in 2016.
Total Medicare Part D Spending on Insulin
According to our analysis, total Medicare Part D spending on insulin increased by 840% between 2007 and 2017, from $1.4 billion to $13.3 billion—including what Medicare, plans, and beneficiaries paid. In light of rising prices for existing insulin products and the introduction of more costly insulin therapies over time, average annual total Part D spending on insulin products per user increased by 358% between 2007 and 2016—from $862 to $3,949—while average total Medicare Part D spending per insulin prescription increased by 280% over these years—from $96 to $363 (Figure 2).
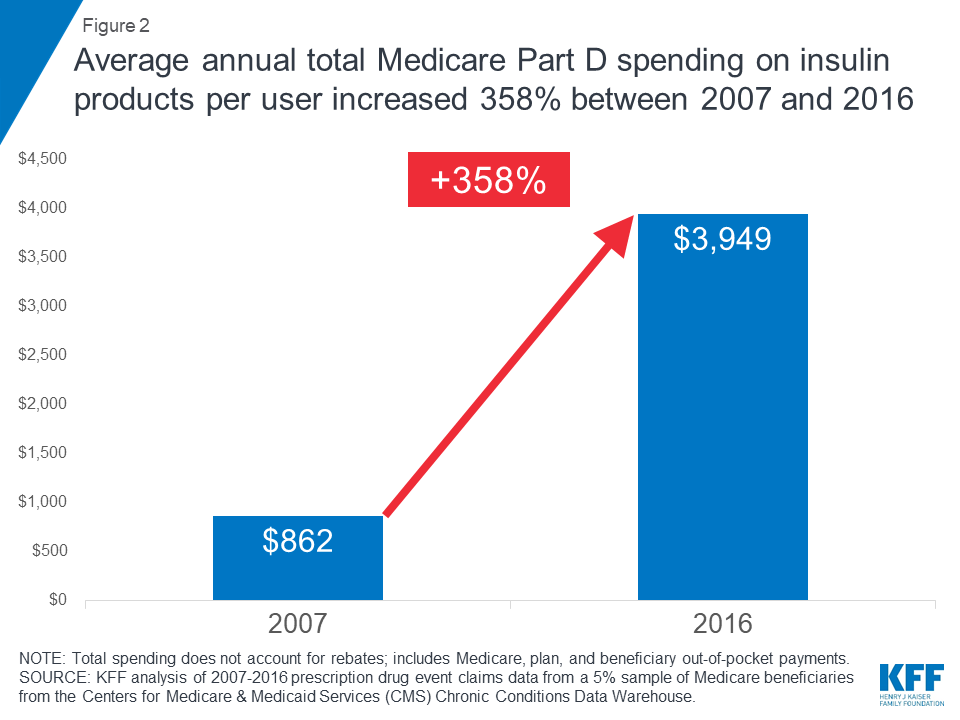
Figure 2: Average annual total Medicare Part D spending on insulin products per user increased 358% between 2007 and 2016
The total number of Part D enrollees using any insulin therapy nearly doubled between 2007 and 2016, from 1.6 million enrollees to 3.1 million—a much smaller increase in percentage terms (86%) than the percent increase in total Part D spending on insulin over the 2007-2016 period (753%) (Table 1). The total number of insulin prescriptions covered by Part D also increased over these years (from 14.8 million in 2007 to 33.3 million in 2016), but the percentage increase (125%) was also substantially lower than the percent increase in total insulin spending.
Total Part D spending on top insulin therapies. In 2017, the top five insulin therapies covered under Part D accounted for 62% of total Part D spending on insulin, or $8.2 billion out of the $13.3 billion total spending on insulin (Figure 3). Among all insulin products, Part D spending was highest for Lantus Solostar, a long-acting insulin manufactured by Sanofi, with $2.6 billion in Part D spending in 2017. This one drug alone, used by 1.1 million Part D enrollees in 2017, accounted for 20% of total Part D spending on insulin that year. Lantus Solostar was also among the top five drugs overall in terms of total Part D spending in 2017.
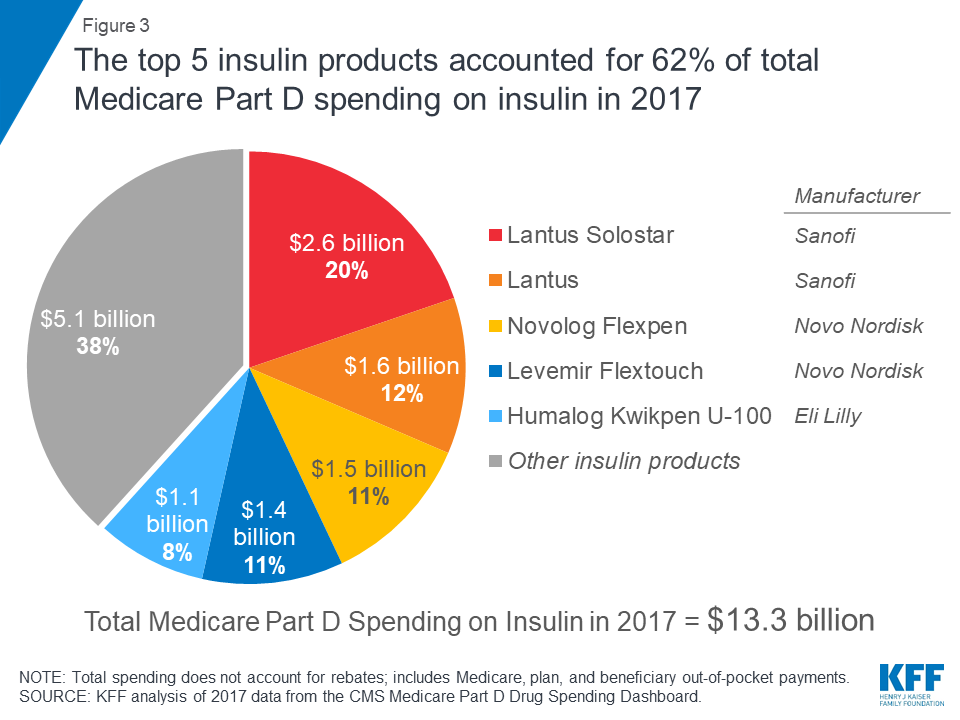
Figure 3: The top 5 insulin products accounted for 62% of total Medicare Part D spending on insulin in 2017
Average total Part D per capita costs for insulin therapy in 2017 ranged from $693 for Humulin R, a short-acting regular insulin manufactured by Eli Lilly—used by 102,000 Part D enrollees in 2017—to $10,014 for Humulin R U-500, a concentrated regular insulin for people who need large doses of insulin, also manufactured by Eli Lilly—used by 14,500 beneficiaries in 2017.
Total Part D spending by insulin manufacturer. In 2017, total Part D spending on all of the different insulin products from the three main manufacturers was $5.5 billion for Novo Nordisk, $4.8 billion for Sanofi, and $3.0 billion for Eli Lilly (Figure 4). Between 2007 and 2017, spending on insulin therapies from all three manufacturers increased dramatically. Over this time period, cumulative total Part D spending was $27.0 billion for insulin products from Novo Nordisk, another $27.0 billion for Sanofi, and $15.0 billion for Eli Lilly.
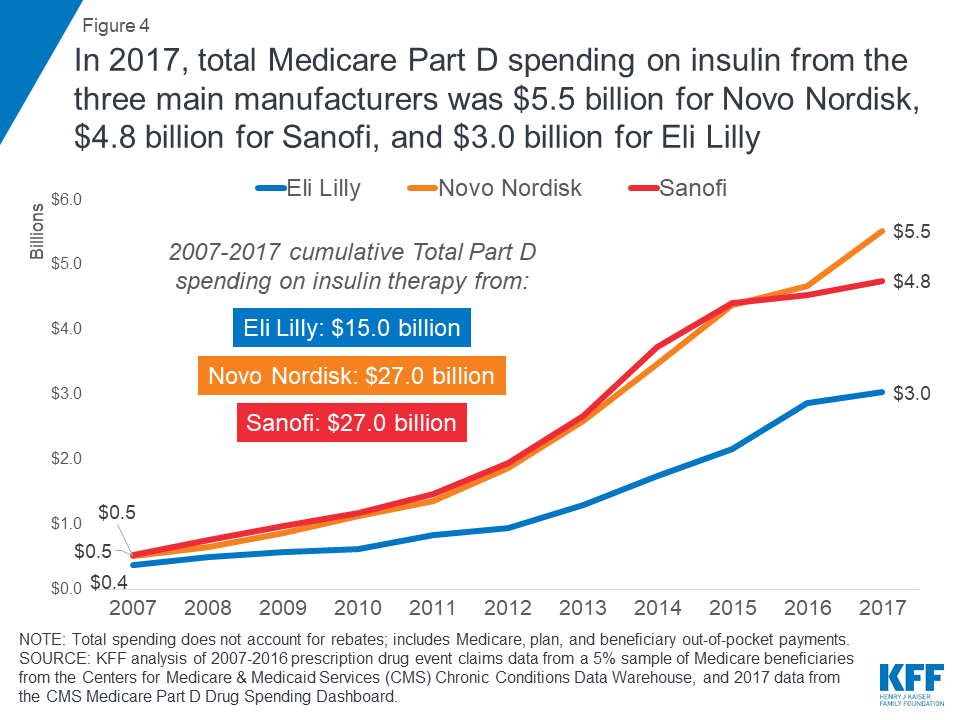
Figure 4: In 2017, total Medicare Part D spending on insulin from the three main manufacturers was $5.5 billion for Novo Nordisk, $4.8 billion for Sanofi, and $3.0 billion for Eli Lilly
Trends in insulin spending per dosage unit. Of the 22 insulin therapies listed in the CMS Part D drug spending dashboard in both 2013 (the first year of dashboard data) and 2017 (the most recent year), 19 products had increases of more than 10% in annual Part D spending per dosage unit between 2013 and 2017, according to CMS estimates (Table 2). Six insulin products had increases of more than 10% in average spending per dosage unit between 2016 and 2017 alone (Figure 5).
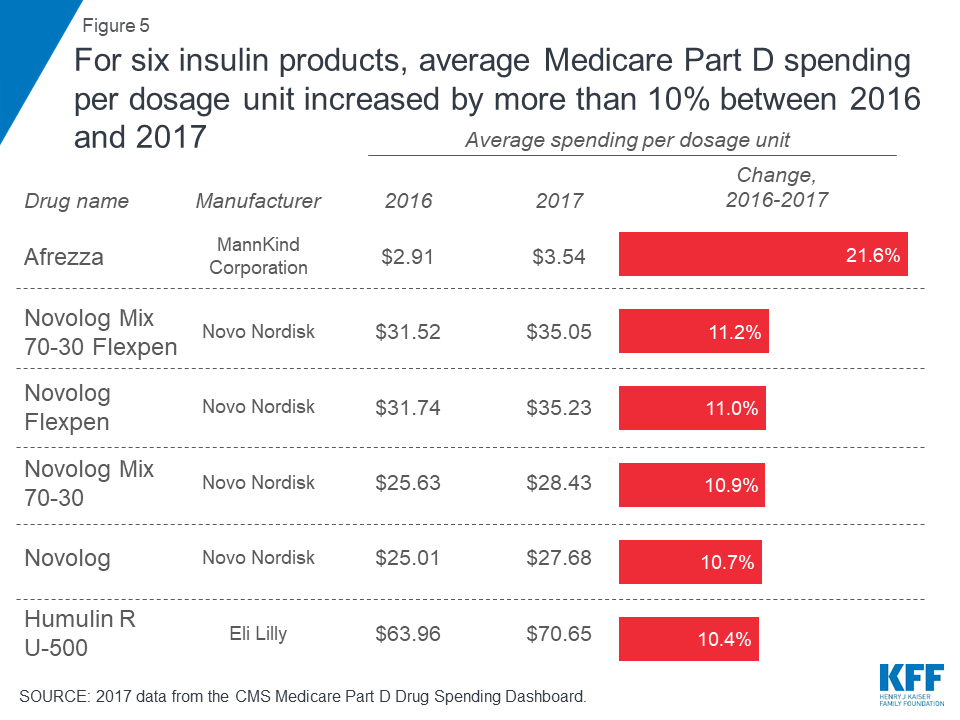
Figure 5: For six insulin products, average Medicare Part D spending per dosage unit increased by more than 10% between 2016 and 2017
These percentage increases in average spending per dosage unit for insulin products represent price increases that can translate to large increases in total spending per claim over time—even if the change in average spending per dosage unit measured in dollars may be relatively low—since there are typically multiple dosage units associated with each claim. For example, while Afrezza has the lowest average spending per dosage unit in 2017 of all the insulin products in the CMS dashboard data ($3.54), the 2016-2017 change of 21.6% was the largest in percent terms—and it translates into a large difference in spending per claim for Afrezza between 2016 and 2017—from $566 per claim in 2016 to $690 per claim in 2017, a $124 increase (Table 2).
Out-of-Pocket Spending on Insulin by Medicare Part D Enrollees
Part D enrollees’ total annual out-of-pocket costs for insulin. Since Medicare Part D plans cover a portion of enrollees’ total drug costs, enrollees pay less than the retail price of drugs covered by their plan, and those who receive Part D low-income subsidies (LIS) face relatively low out-of-pocket costs. Still, in the aggregate, out-of-pocket spending among all Part D enrollees on insulin quadrupled between 2007 and 2016, from $236 million to $968 million, reflecting both an increase in the number of users and price increases for insulin (Figure 6). Between 2007 and 2016, Part D enrollees spent a combined $5.5 billion out of pocket on insulin therapy.
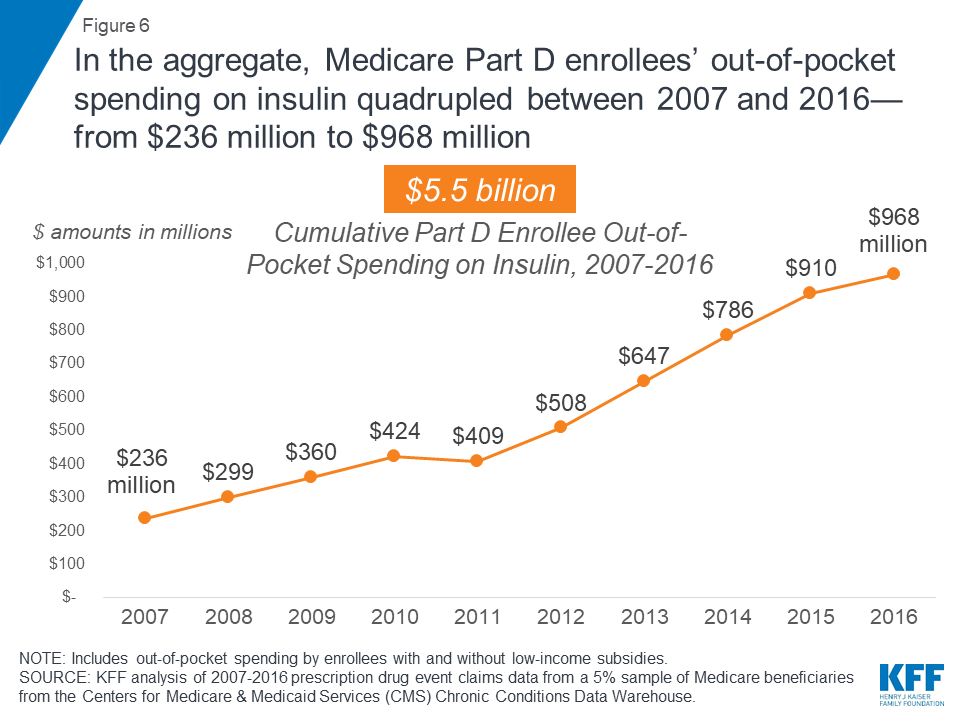
Figure 6: In the aggregate, Medicare Part D enrollees’ out-of-pocket spending on insulin quadrupled between 2007 and 2016—from $236 million to $968 million
Part D enrollees’ average per capita out-of-pocket costs for insulin. Among Part D enrollees who did not receive LIS, average per capita out-of-pocket spending for insulin alone was $588 in 2016, but including costs for all other prescriptions, total per capita out-of-pocket spending among those who used insulin was $1,334. Non-LIS enrollees’ average per capita out-of-pocket spending on insulin in 2016 was nearly double the amount in 2007 ($324; an increase of 81%).
For several insulin products, average per capita out-of-pocket spending by non-LIS enrollees increased by more than 100% between 2007 and 2016; for example, average per capita out-of-pocket spending on Lantus Solostar increased by 291% from $106 to $413 (Figure 7).
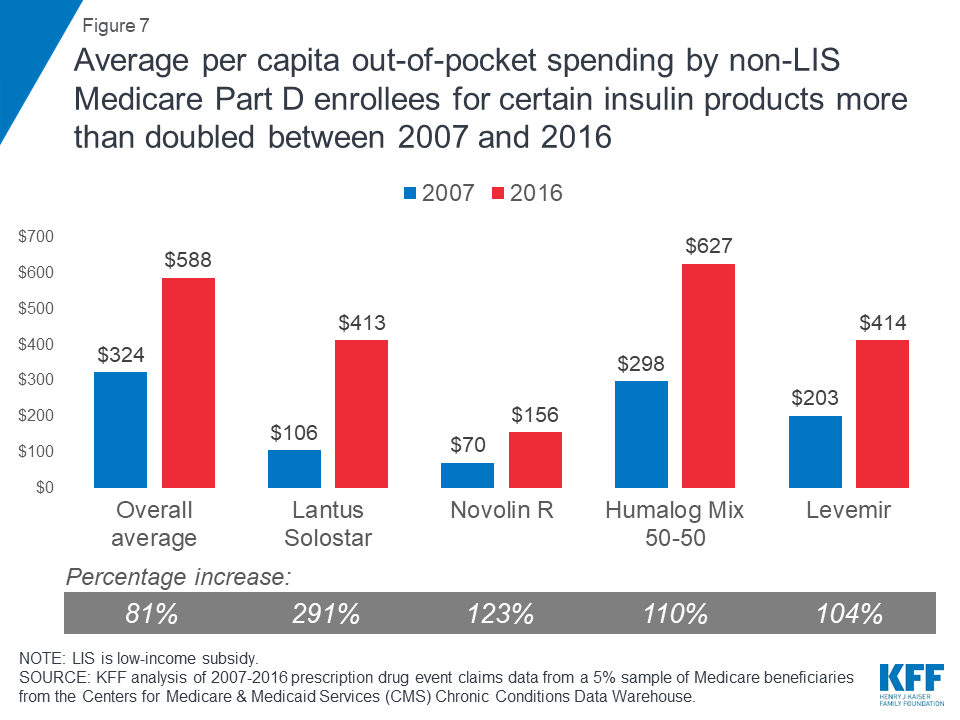
Figure 7: Average per capita out-of-pocket spending by non-LIS Medicare Part D enrollees for certain insulin products more than doubled between 2007 and 2016
In 2016, average annual per capita out-of-pocket spending by non-LIS enrollees who used insulin therapies ranged from $110 for Levemir Flexpen, a long-acting insulin manufactured by Novo Nordisk, to $822 for Humulin R U-500 (Table 3).
Part D enrollees’ out-of-pocket spending on top insulin therapies. In 2016, the top five insulin therapies accounted for 67% of aggregate out-of-pocket spending on insulin by non-LIS enrollees that year, or $0.6 billion out of the $0.9 billion in out-of-pocket spending on insulin by non-LIS enrollees (Figure 8). Aggregate out-of-pocket spending was highest for Lantus Solostar, accounting for 25% ($230 million) of non-LIS enrollees’ total out-of-pocket spending on insulin therapy in 2016.
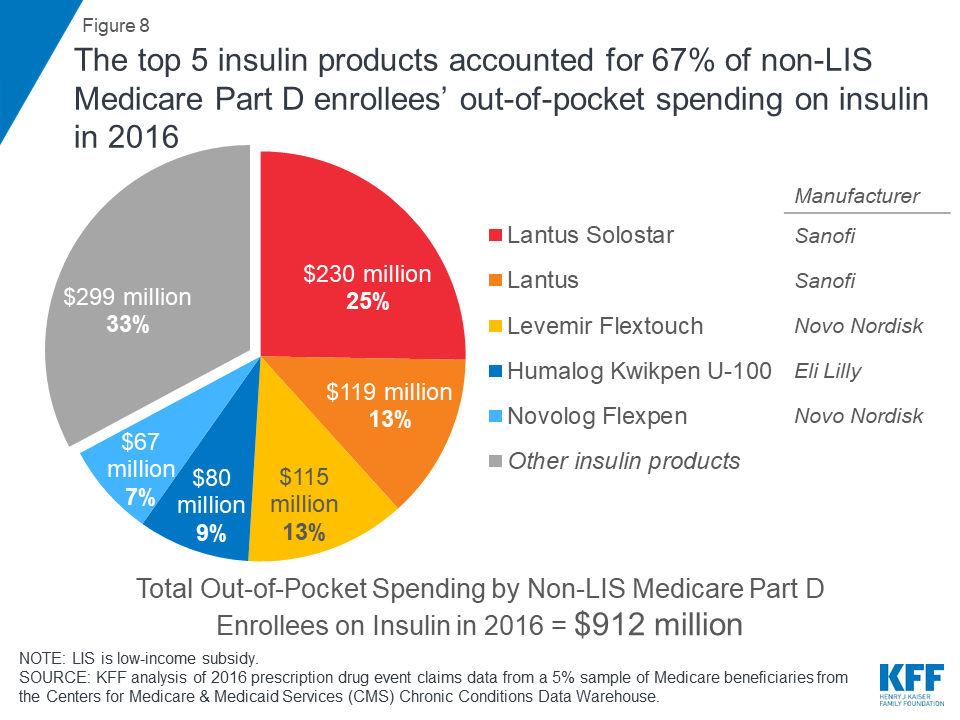
Figure 8: The top 5 insulin products accounted for 67% of non-LIS Medicare Part D enrollees’ out-of-pocket spending on insulin in 2016
Illustrating the Potential Effect of Rebates on Total Insulin Spending
Our analysis is based on retail claims data and aggregated spending data that do not take into account manufacturer rebates and discounts to plans, which are considered proprietary and therefore not publicly available. There is data suggesting that insulin manufacturers have provided large rebates and discounts to payers that have produced net prices that are significantly lower than the high list prices that have attracted public scrutiny. Regardless of the magnitude of rebates for insulin products, however, rebates do not help to lower enrollees’ out-of-pocket costs for insulin. This is because the amount that enrollees pay out of pocket is either a flat dollar copayment (depending on their plan’s cost-sharing design) or, if they are paying full cost in the deductible phase or a coinsurance amount, their cost is based on pre-rebate list prices rather than post-rebate net prices.
Because CMS does not disclose drug-specific rebates, we are unable to know exactly the degree to which our estimates of total Part D spending on insulin therapy might overstate actual costs to Medicare and plans. We can approximate the potential effect of rebates on total Part D spending by assuming that all Part D plans had received for all insulin products the average rebate reported by Medicare’s actuaries each year between 2007 and 2017. Based on this assumption, insulin spending would have increased from $1.3 billion in 2007 (applying the 9.6% average rebate in 2007) to $10.3 billion in 2017 (applying the 22.8% estimated average rebate in 2017). This amounts to a 702% increase in total Part D spending on insulin between 2007 and 2017, compared to an 840% increase based on the pre-rebate total spending amounts ($1.4 billion and $13.3 billion, respectively). If actual rebates for insulin products were larger than these averages, total spending would be lower than these estimates.
Implications
Rising prices for insulin have attracted increasing scrutiny from policymakers in recent months. Our analysis demonstrates that rising insulin prices since 2007 have translated into significantly higher out-of-pocket spending for beneficiaries in Medicare Part D plans and higher spending for the program overall (not taking into account rebates). The number of people Medicare covers for insulin therapy has increased as the number of Medicare beneficiaries with diabetes has risen. Average annual total Part D spending per insulin user increased by 358% between 2007 and 2016, while average out-of-pocket costs for insulin by non-low income subsidy Part D enrollees nearly doubled.
Members of Congress and the Trump Administration have introduced several proposals that could help to address concerns about rising prices for insulin products and affordability concerns for patients, including banning rebates from drug manufacturers unless they are shared directly with patients at the point of sale, taking steps to increase the availability of generic products, allowing Medicare to negotiate drug prices, and allowing patients to import drugs from other countries. Rising prices for insulin therapy in recent years and the resulting increases in Medicare Part D and beneficiary out-of-pocket spending illustrate why the cost of prescription drugs is an ongoing concern for patients and public and private payers, and a pressing issue for policymakers.
Juliette Cubanski, Tricia Neuman, and Sarah True are with the Kaiser Family Foundation. Anthony Damico is an independent consultant.
Supported in part by Arnold Ventures.
KFF retains complete control over all of its policy analysis content.
| Data and Methods |
| We analyze total and out-of-pocket spending on insulin therapies covered by Medicare Part D, in the aggregate and average per insulin user and by manufacturer, based on 2007-2016 prescription drug event claims data from a 5% sample of Medicare beneficiaries from the Centers for Medicare & Medicaid Services (CMS) Chronic Conditions Data Warehouse, and 2013-2017 data from the CMS Medicare Part D Drug Spending Dashboard (March 2019 update). The ‘Manufacturer Summary’ tab in the Drug Spending Dashboard was used to identify the manufacturers of the insulin products in this analysis.
Estimates of total Part D spending on insulin include costs paid by Medicare, plans, and beneficiary out-of-pocket payments. These estimates are based on retail claims data that do not take into account drug-specific manufacturer rebates and discounts to plans, which are considered proprietary and therefore not publicly available. To illustrate the effect of rebates, we used average Part D rebates for 2007 to 2017 as reported in 2017 and 2018 Annual Reports of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. The Part D drug spending dashboard does not include out-of-pocket spending data or aggregated data across all insulin therapies, so for those measures we focus on 2007-2016 data. Estimates of the share of Medicare beneficiaries with diabetes is based on our analysis of 2000 and 2016 data from the CMS Medicare Current Beneficiary Survey. |