Contraceptive Experiences, Coverage, and Preferences: Findings from the 2024 KFF Women's Health Survey
Contraceptive care is an important component of overall health care for many people, and most women use contraception at some point in their lifetime. As abortion access has become more limited post-Dobbs there has been an increased attention on the need for and future of contraceptive access.
This brief provides a close examination of women’s experiences with contraception, insurance coverage, contraceptive preferences, and interactions with the health care system. We also explore the influence and reach of contraceptive information on social media. The KFF Women’s Health Survey, a nationally representative survey of women in the United States was fielded in May and June 2024 and includes a sample of 3,901 women of reproductive age (18-49). Women include individuals who identify as such, as well as those with other gender identities that preferred to complete the female set of sexual and reproductive health questions in the survey. See the methodology section for detailed definitions, sampling design, and margins of sampling error.
Key Takeaways
Use of Contraceptives
- Eight in ten (82%) women of reproductive age say they used some form of contraception in the past 12 months.
- Almost half (48%) of contraceptive users used more than one contraceptive method in the past 12 months, with male condoms and oral contraceptives representing the most commonly used methods.
- The majority of women use contraception to prevent pregnancy (85%), but one in seven (14%) use it solely for another reason, such as managing a medical condition or preventing a sexually transmitted infection.
- Nearly seven in ten (69%) women of reproductive age say it is very important for them to avoid becoming pregnant in the next month.
Contraception in Social Media
- Nearly four in ten (39%) of reproductive age women have heard something on social media about birth control in the past 12 months, including half (49%) of women ages 18 to 25.
- Almost four in ten (38%) women of reproductive age who have heard something on social media about birth control (19% of all reproductive age women), have talked to someone in their life about what they saw or heard.
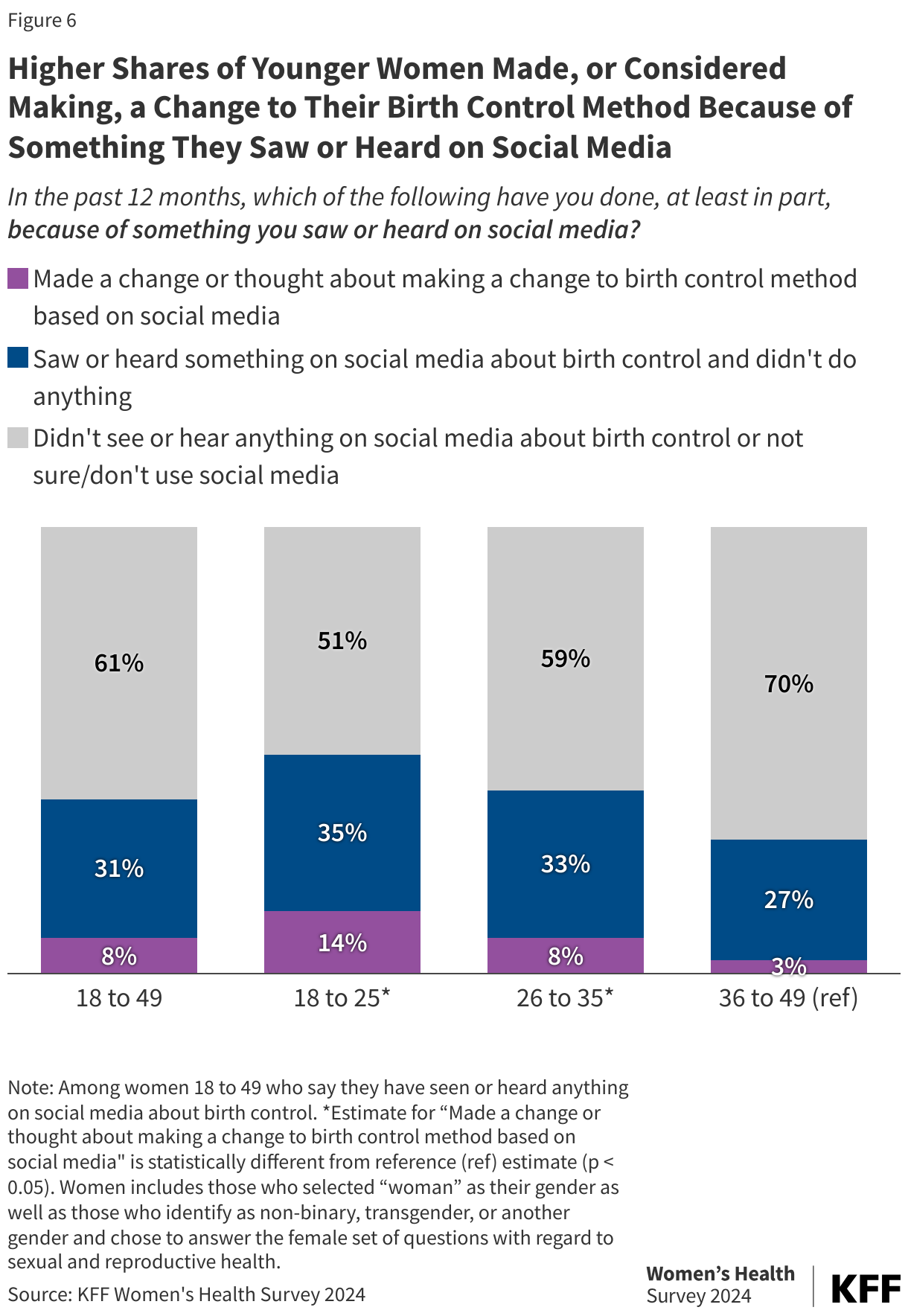
- One in seven women ages 18 to 25 (14%) say they made a change or thought about making a change to their birth control method because of something they saw or heard on social media.
Contraceptive Coverage
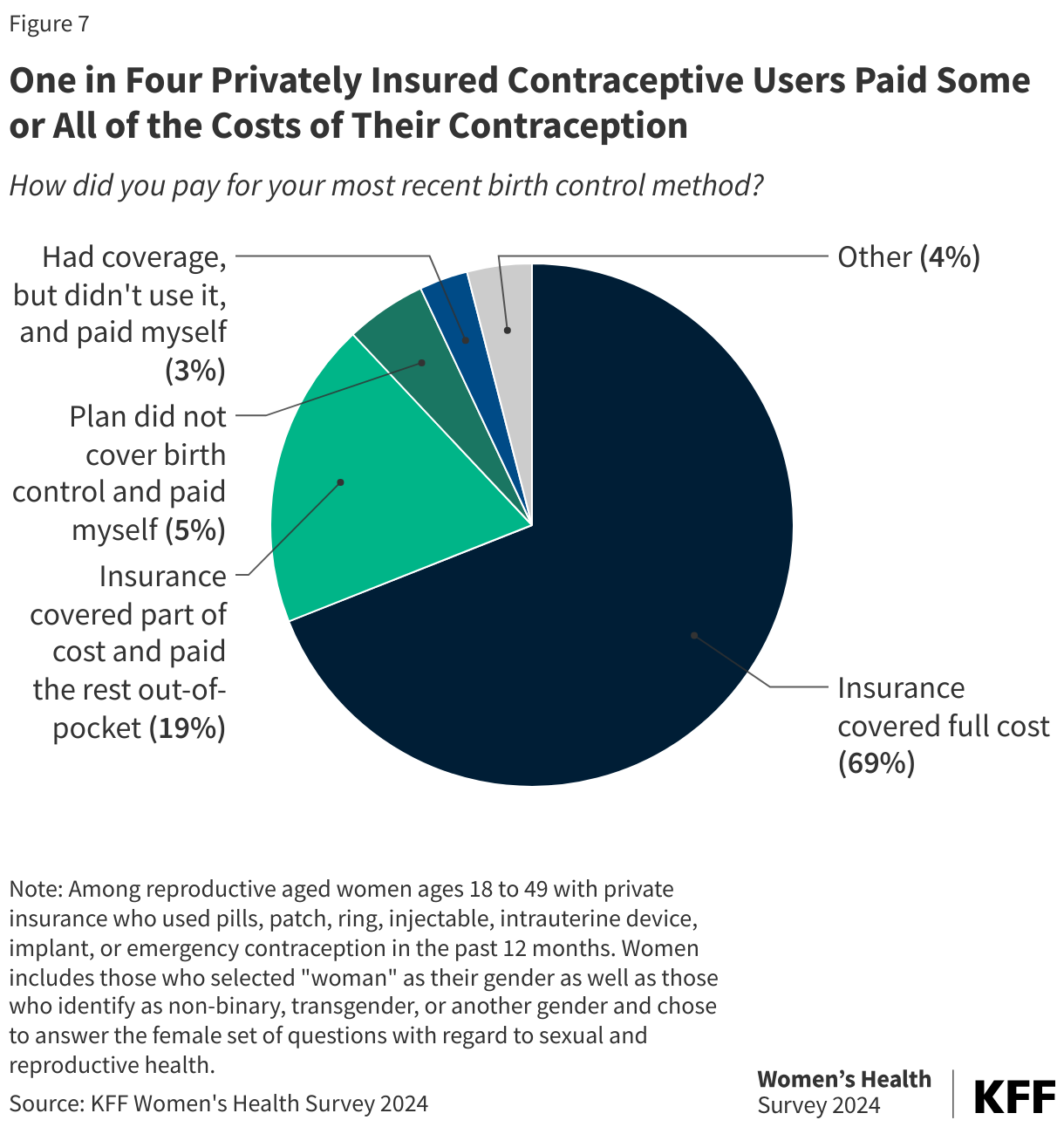
- While insurance paid the full cost of contraception for the majority (69%) of contraceptive users with private insurance, a quarter (24%) report that they paid some or all of the costs out-of-pocket because their plan did not cover the full cost or did not cover birth control at all.
- Despite emergency contraceptive pills being covered by insurance at no cost (with a prescription), few (17%) of those who have used emergency contraception in the past 12 months say they got it with a prescription.
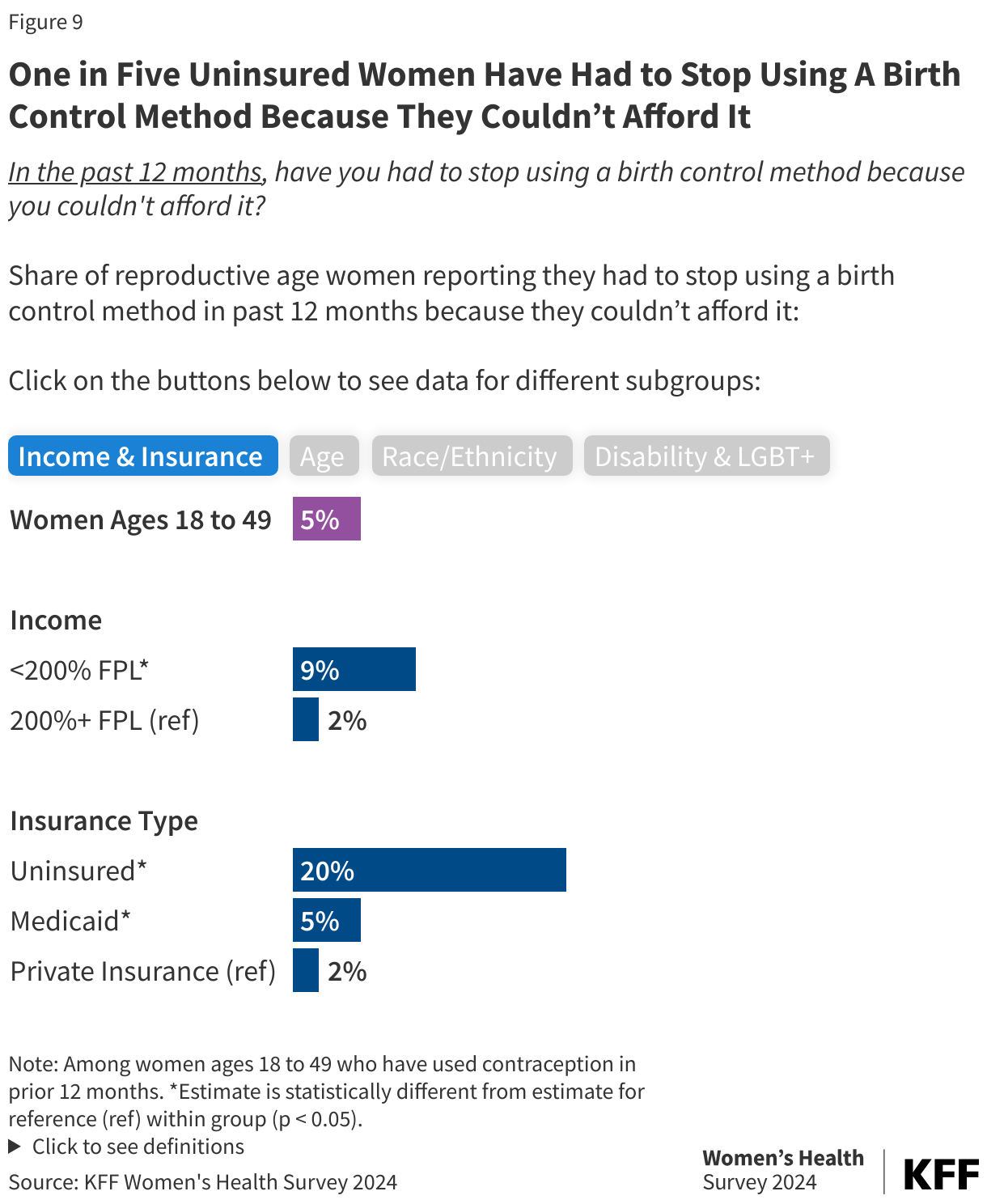
- The costs of contraceptives are still a barrier for some women; one in five (20%) uninsured women had to stop using a birth control method because they couldn’t afford it.
Access and Quality of Care
- Three quarters (78%) of women received their most recent contraceptive care at a doctor’s office, but clinics play an important role for women with low incomes (21%) and women without insurance (28%).
- One in five (20%) reproductive age women say they would not know where to get emergency contraception if they wanted or needed it despite its availability as an over-the-counter method.
- Four in ten (42%) contraceptive users rated their contraceptive counseling as excellent across all measures of care.
- Nearly a quarter (23%) of contraceptive users say if they could use any type of birth control method available, they would use a different method than the one they are currently using. Of this group, nearly one in four (23%) say they prefer their partner get a vasectomy.
Use of Contraceptives
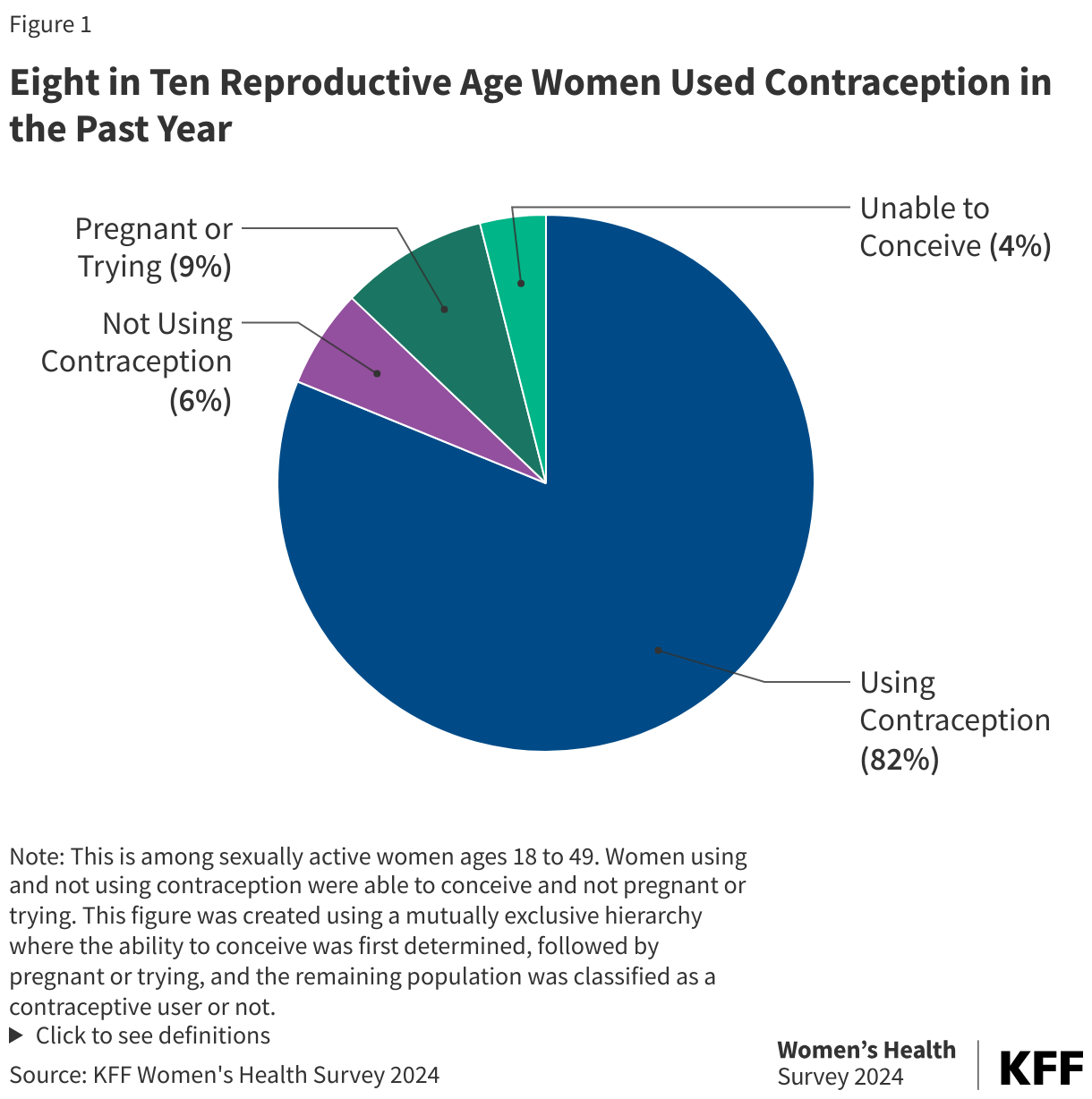
The majority of reproductive age women use contraception. Eight in ten (82%) women ages 18 to 49 say they used some form of contraception in the past 12 months (Figure 1). Methods used include a sterilization procedure that they or their partner have had, pills, injectables, patch, ring, intrauterine device, contraceptive implant, male condoms, emergency contraception, fertility awareness-based methods, and withdrawal. Nearly one in ten (9%) reproductive age women say they are either pregnant or trying to conceive, 4% say they are unable to conceive, and 6% did not use contraception in the past 12 months.
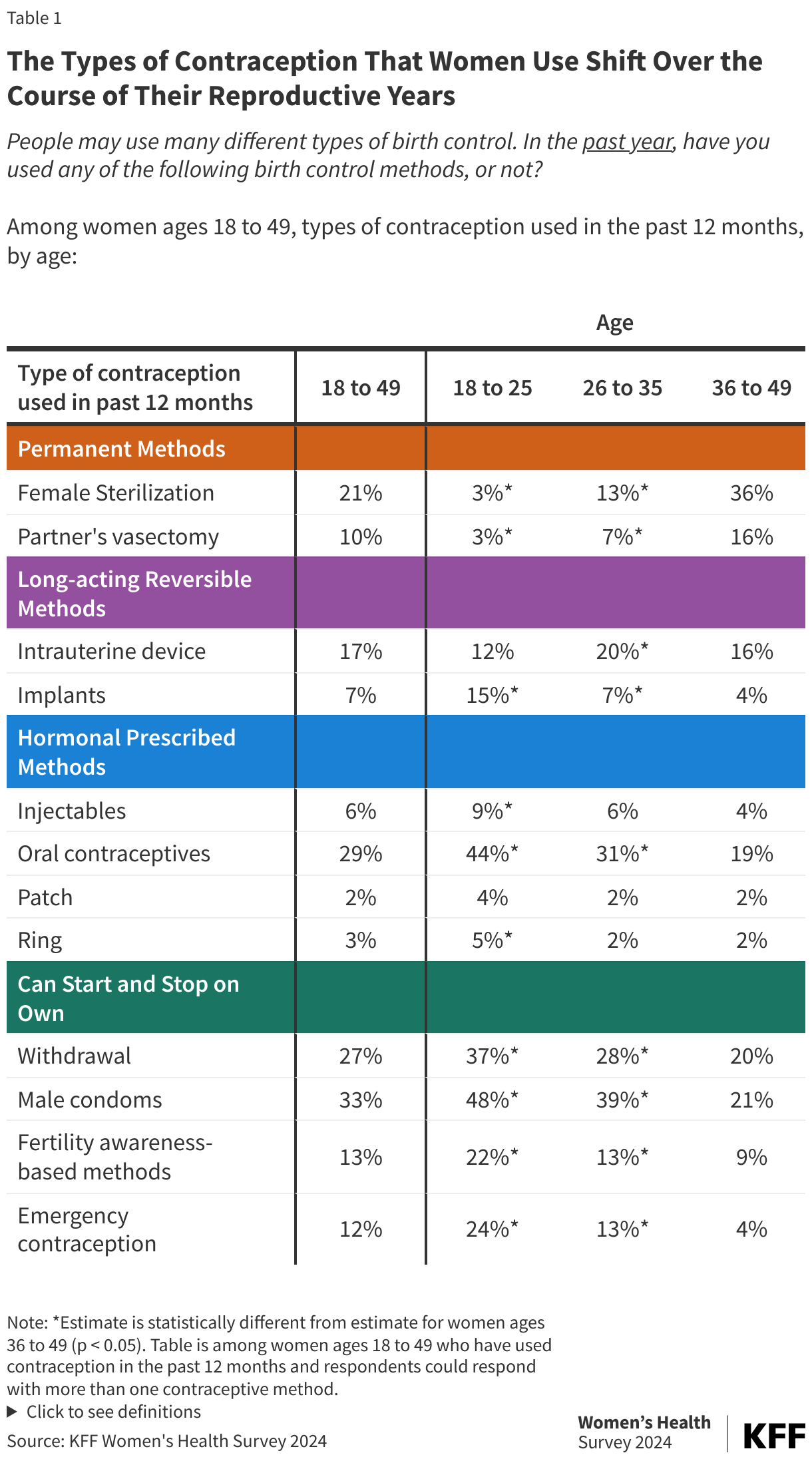
Nearly half (48%) of contraceptive users report using more than one kind of contraceptive method in the past 12 months, and the methods used shift as they age (Table 1). Among all reproductive age women, three in ten (31%) rely on a permanent method, such as female sterilization (21%) or a partner’s vasectomy (10%). The share of women who report relying on permanent methods increases to over half (52%) of women ages 36 to 49. Almost a quarter (24%) of women used a long-acting reversible method in the past year, such as an intrauterine device (IUD) or contraceptive implant, with highest shares of women ages 26 to 35 using IUDs and larger shares of women ages 18 to 25 using contraceptive implants. Four in ten women used a shorter acting hormonal prescribed method in the past 12 months, with oral contraceptive pills accounting for the largest share among all age groups.
Sizable shares of women use contraceptive methods that they can easily start and stop on their own without a prescription, with condoms and withdrawal representing two of the most widely used methods among women of all age groups. Almost one in four (22%) younger women ages 18 to 25 report using fertility awareness-based methods, which could reflect a growing interest in non-hormonal methods, discussed extensively on social media outlets targeting young people. One in four (24%) younger women also report using emergency contraception in the past 12 months compared to just 4% of women ages 36 to 49.
Women also use contraception for reasons other than preventing pregnancy. Two-thirds (65%) of women say they use contraception only to prevent pregnancy (Figure 2), one in seven (14%) use contraception solely for a reason outside of preventing pregnancy, such as to manage a medical condition or prevent a sexually transmitted infection in the case of condoms, and one in five (20%) use it to prevent pregnancy and another reason. Among women who identify as a disabled person or a person with a disability, one in four (26%) use contraception solely for a reason outside of preventing pregnancy, such as managing a medical condition, making access to contraception particularly important for this population (data not shown in figure).
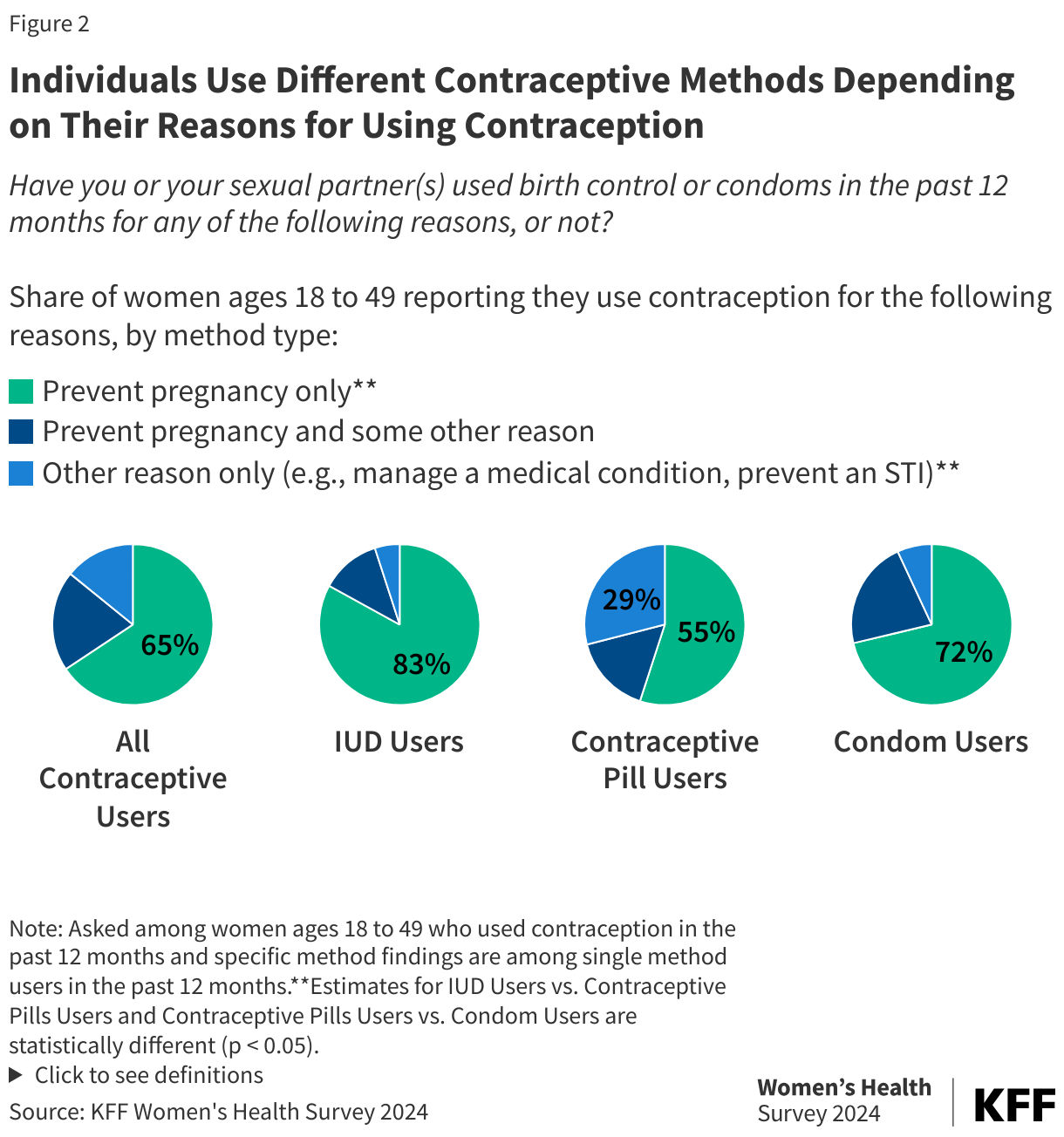
The type of method selected may depend on their reason for use. For those who only used an IUD in the past 12 months, eight in ten (81%) report using contraception for the sole reason of preventing pregnancy. A much larger share of contraceptive pill users, compared to users of other forms of contraception, report using contraception for only reasons outside of pregnancy prevention, as many hormonal methods are used to manage menstrual irregularities, treat acne, alleviate menstrual migraines, and manage symptoms of conditions like polycystic ovary syndrome (PCOS). Nearly one in five condom only users use contraception to prevent both prevent pregnancy and some other reason, likely to prevent STIs.
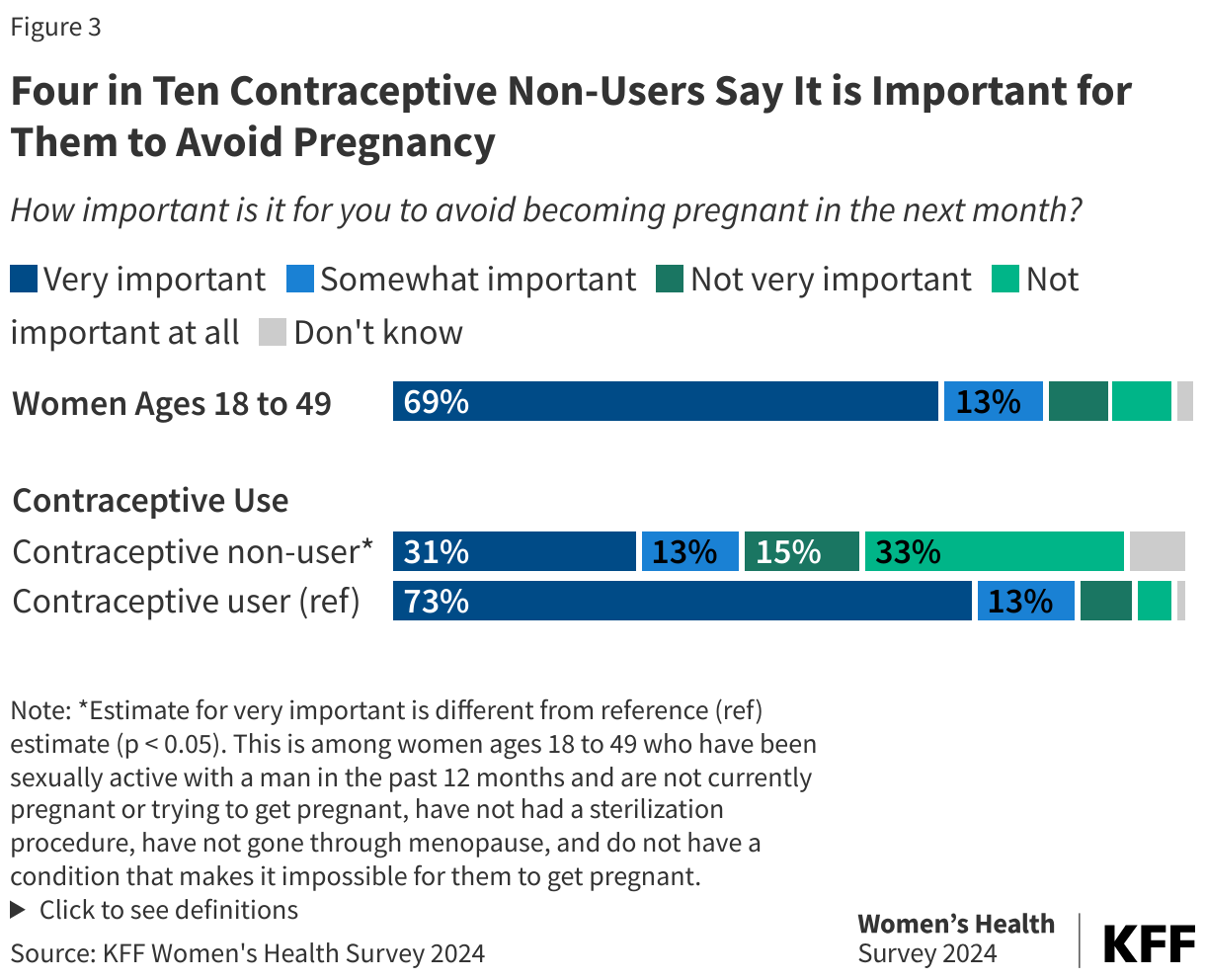
Nearly seven in ten (69%) women of reproductive age say that avoiding pregnancy in the next month is very important to them (Figure 3). Pregnancy prevention is very important to nearly three in four (74%) women ages 18 to 25. While smaller shares of contraceptive non-users say it is very important for them to avoid pregnancy compared to contraceptive users (31% vs. 73%), four in ten (44%) still say it is important for them to avoid becoming pregnant in the next month. There are not significant differences between women of certain demographics including race/ethnicity, income, disability, and abortion status in state of residence.
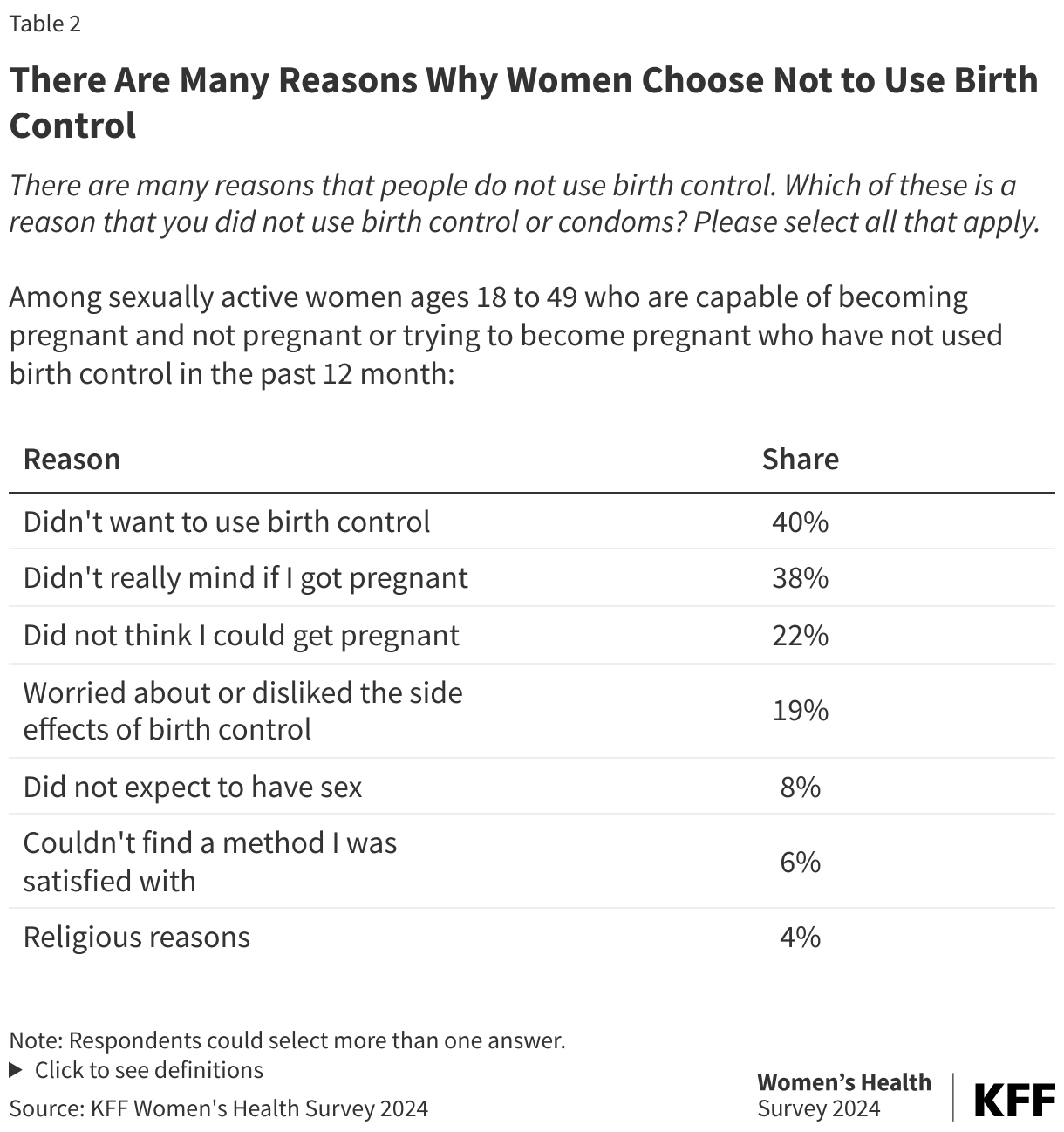
There are many reasons why someone may choose not to use contraception. Among sexually active women capable of becoming pregnant who do not use contraception, four in ten (40%) say they did not want to use birth control, another nearly four in ten (38%) say they didn’t really mind if they got pregnant, and almost one in four (22%) say they did not think they could get pregnant (even though they or their partner were not sterilized etc.) (Table 2). One in five (19%) do not use birth control because they were worried about or disliked the side effects of birth control. Another 7% say they did not expect to have sex, 6% couldn’t find a method they were satisfied with, and 4% do not use contraception for religious reasons.
Contraception in Social Media
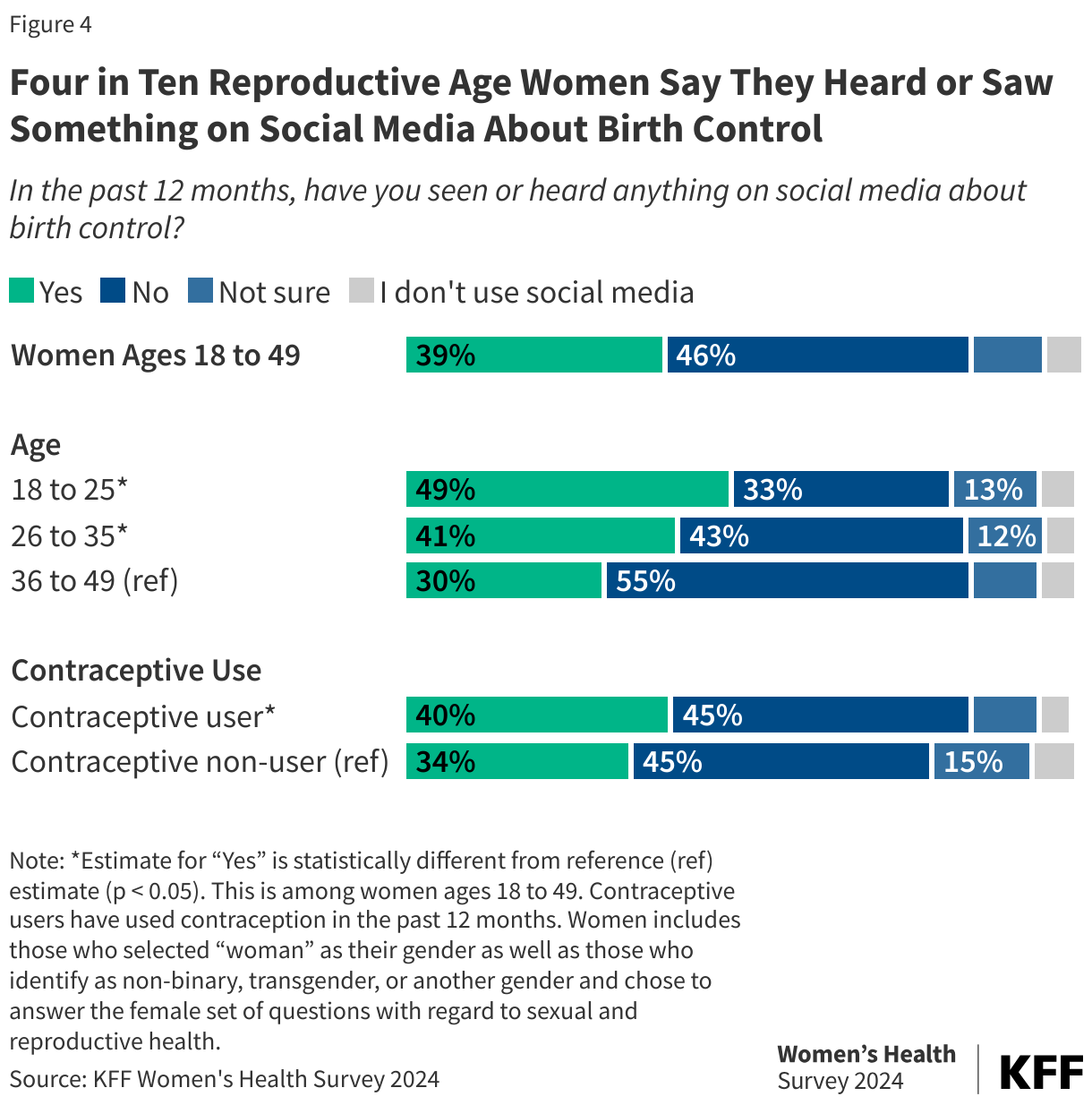
Contraceptive information is pervasive on social media. Nearly four in ten (39%) women of reproductive age say they have seen or heard something on social media about birth control in the past 12 months (Figure 4). This includes half of women ages 18 to 25 (49%) and four in 10 women ages 26 to 35 (41%) who report seeing or hearing information about birth control via social media. Exposure to social media that talks about birth control was higher among women who use contraception than those who do not.
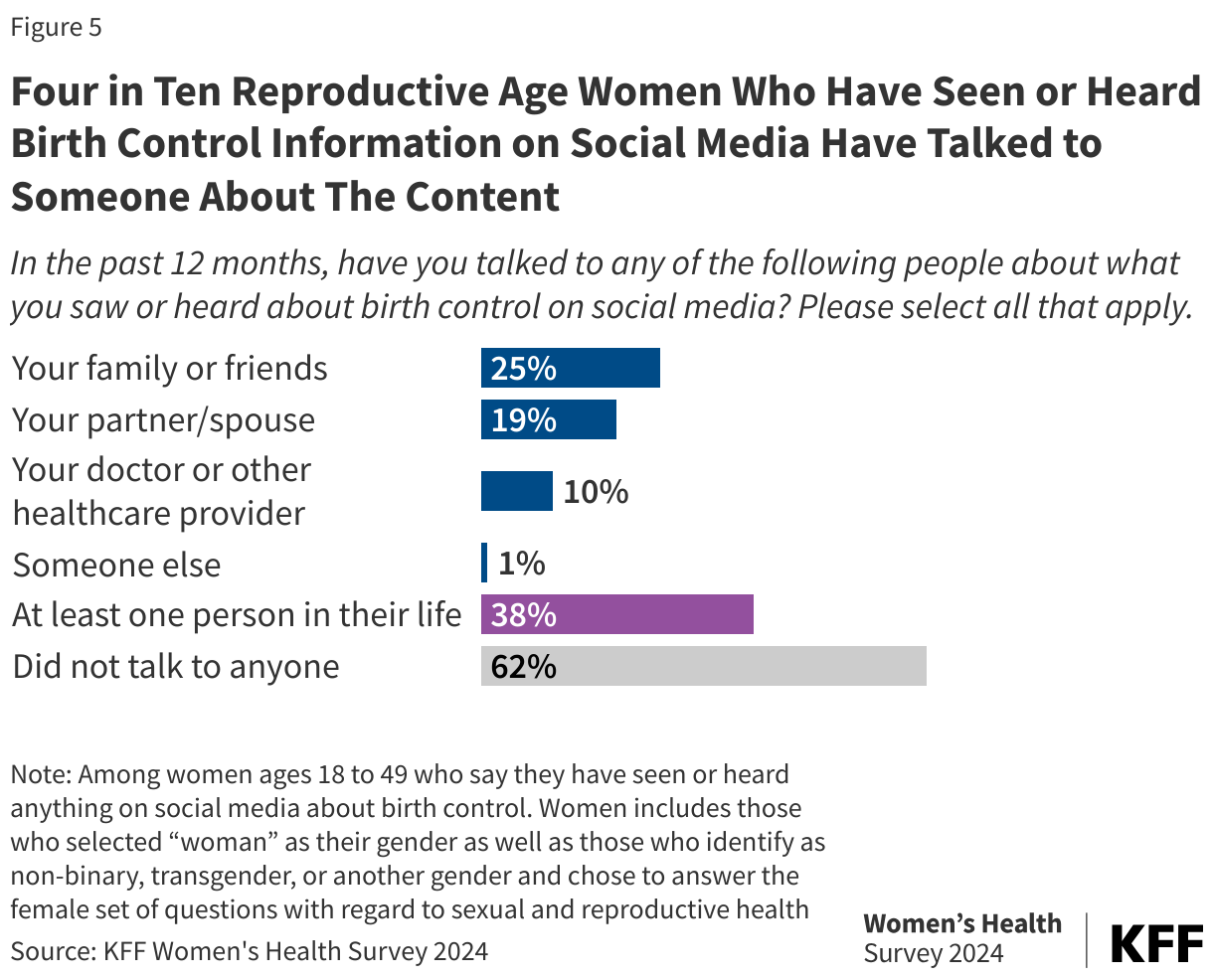
Almost four in ten (38%) reproductive age women who have seen or heard something on social media about contraception report they have talked to at least one person in their lives about the content (Figure 5). Among those who have seen or heard anything on social media about birth control (39% of women ages 18 to 49), a quarter (25%) say they talked to their family or friends about the birth control content. One in five (19%) say they talked to their partner or spouse, and one in ten (10%) say they talked to their doctor or healthcare provider. Most women who have seen or heard anything on social media about birth control did not talk to anyone about the content (62%).
While social media can be a tool to spread reliable and trustworthy health-related information, it can be and has been used to spread mis- and dis-information. A growing number of social media influencers have tapped into their social networks to share their negative experiences with certain birth control methods such as oral contraceptive pills or intrauterine devices (IUDs), often making false claims about the safety and efficacy of hormonal contraception. While previous KFF research found that only a small share of women use social media as their main source of information about birth control side effects, there have been anecdotal reports about women stopping contraception use after consuming misleading or factually incorrect social media.
Few women say they made a change or thought about making a change to their method of birth control because of something they saw on social media, but younger women seem to be more receptive to change based on social media messaging (Figure 6). Compared to older reproductive age women (ages 36 to 49; 3%), larger shares of women ages 18 to 25 (14%) and 26 to 35 (8%) made a change or thought about making a change to their birth control method based on something they saw or heard on social media. Across all age groups, most reproductive age women say they did not change their birth control method because of something they saw or heard on social media.
Contraceptive Coverage
The ACA requires that plans cover out-of-pocket contraception costs for most individuals with private insurance, yet a sizable share of women are still paying some of the cost. A quarter (24%) of contraceptive users with private insurance say they paid out-of-pocket some or all of the costs of their contraception because their plan did not cover the full cost or did not cover birth control at all (Figure 7).
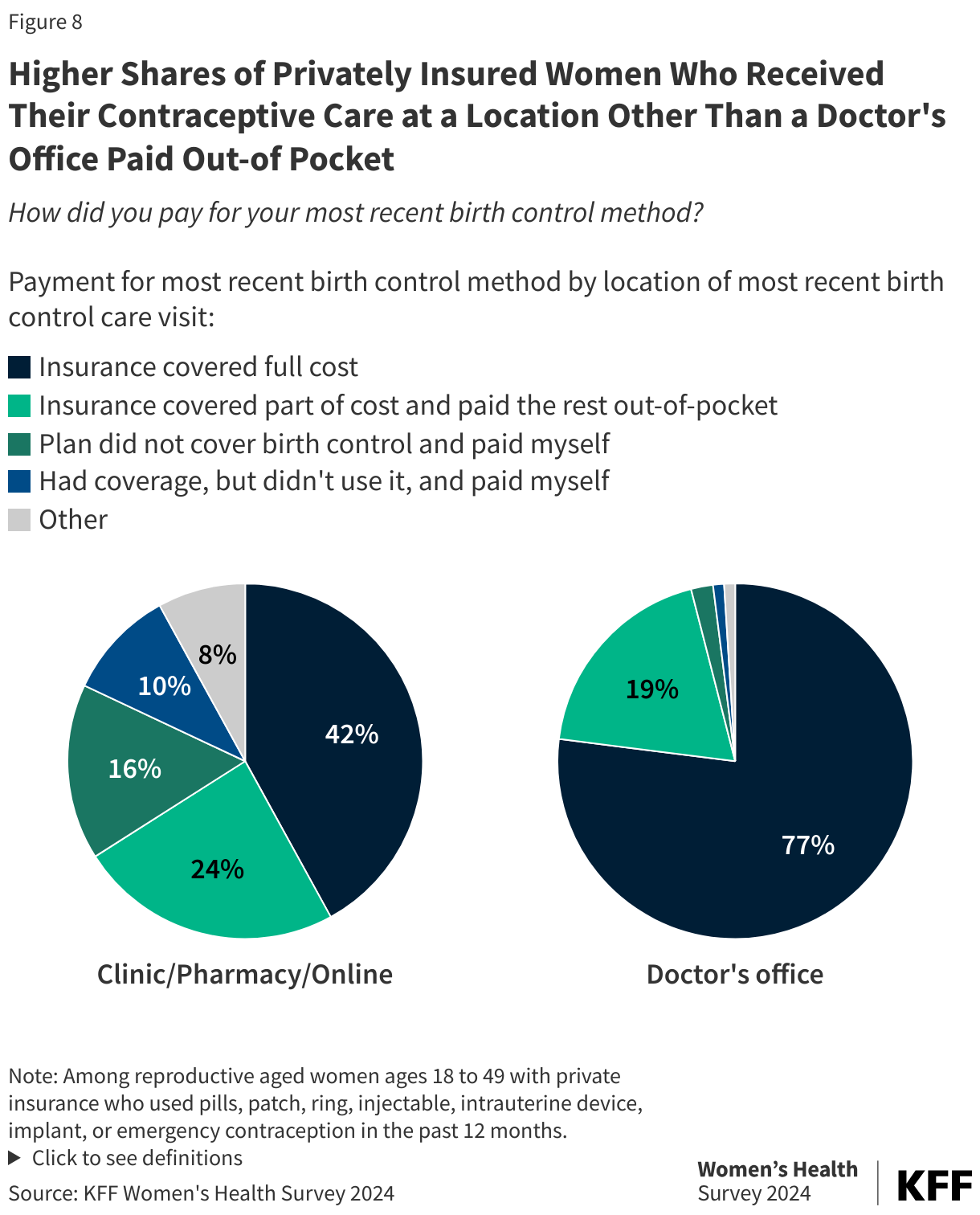
The share of individuals paying out-of-pocket for contraception dropped dramatically shortly after the ACA’s contraceptive coverage requirements were adopted, however, there have been several reports about people continuing to pay out-of-pocket. Reasons could be enrollment in a grandfathered health plan that does not have to adhere to the contraceptive coverage requirements, working for an employer that has religious or moral objections to covering contraception, or going to an out-of-network provider. Some face out-of-pocket costs for using a brand name method that has a generic alternative. A higher share of privately insured women who received their contraceptive care at a location other than a doctor’s office say they paid out-of-pocket for their care (40% vs. 20%) (Figure 8).
This could include individuals using telecontraception apps, which do not always accept insurance or charge a membership or subscriber fee. It could also include individuals purchasing emergency contraception without a prescription, which health plans have not been required to cover. New proposed regulations issued by the Biden administration, if finalized would require health plans to cover all OTC methods, including Opill, spermicide, and male condoms when obtained through an in-network pharmacy. While a type of emergency contraceptive pills (Plan B and its generic alternatives) is available over the counter, most insurers require a prescription before they will cover the costs. Among those who used EC pills in the past 12 months (12% of reproductive age women), less than one in five (17%) got it with a prescription. The majority (83%) of reproductive age women who used EC pills in the past years obtained over-the-counter emergency contraception without a prescription and most likely pay the full cost, which can be up to $50.
Overall, 5% of reproductive age women and 20% of those who are uninsured, say they have had to stop using a contraceptive method because they could not afford it (Figure 9). Discontinuation of a method due to costs was reported by nearly one in ten (9%) women with low incomes and one in five (20%) women who are uninsured. Title X clinics and federally qualified health centers are designed to provide free or low-cost contraception to people with low incomes and those without insurance. However, people may not be aware of these free or low-cost services, or they may reside in a community that does not have a clinic site nearby.
Access to and Quality of Contraceptive Care
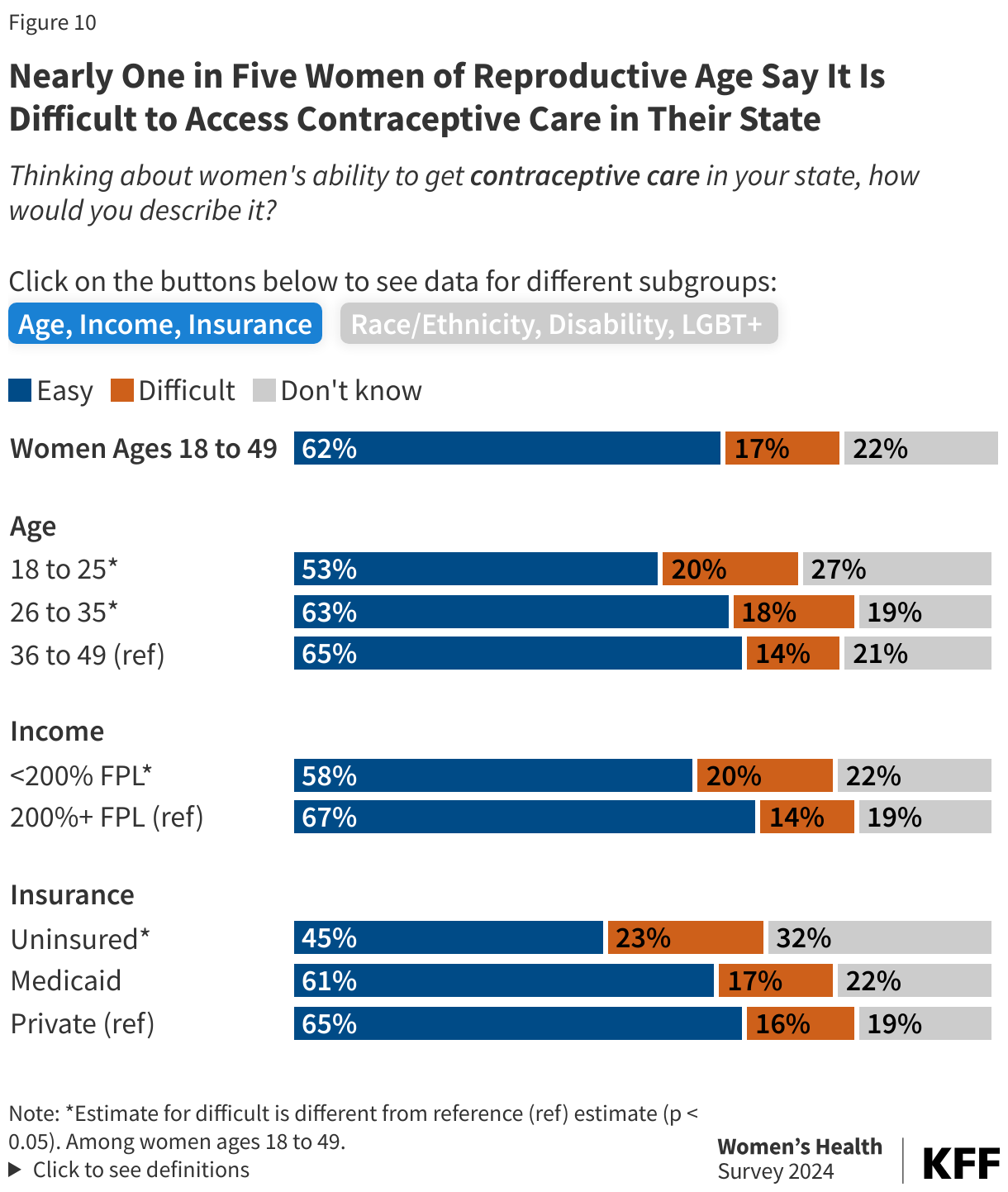
There has been an increased attention to the importance of contraceptive access, especially post-Dobbs where access to abortion is now banned or severely restricted in many states. Nationally, nearly one in five women of reproductive age say it is “difficult” to access contraceptive care in their state and this rises to nearly one in four (23%) among those who are uninsured women (Figure 10). Larger shares of younger women and women with lower incomes also describe contraceptive care as difficult to access compared to those who are older or with higher incomes.
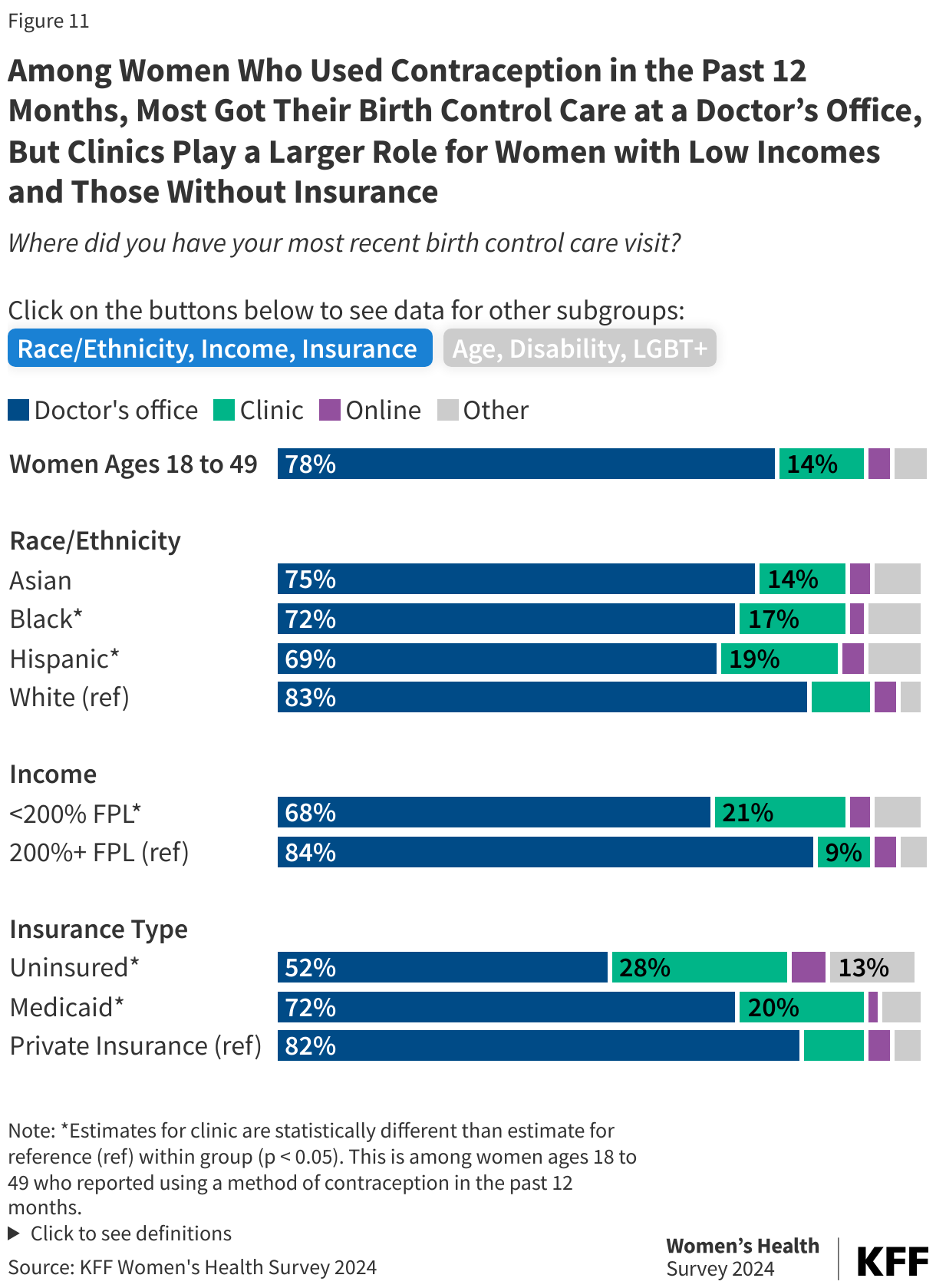
The avenues through which people can access contraception has been expanding, but most (77%) women still obtain their contraceptive care through a doctor’s office (Figure 11). Clinics also play an important role for many, with higher shares of Black (16%) and Hispanic (19%) women compared to White women (10%) receiving their contraceptive care at a clinic-based setting, such as a community health center, Planned Parenthood or other family planning clinic, or a school-based or walk-in clinic. Among contraceptive users, one in five (21%) women with low incomes and those who have Medicaid coverage (20%) obtain their contraceptive care at a clinic and this rises to 28% of women who are uninsured. Nearly one in ten (9%) women using contraception access their birth control care outside of a clinic setting, such as online through a website or app or through a pharmacy, drug store, or some other place.
Over-the-counter (OTC) options from pharmacies, drug stores, and online websites can be appealing avenue for contraceptive access especially for people without a clinician’s prescription for hormonal methods. Until recently, over-the-counter options for contraceptives intended for regular use were limited to non-hormonal methods such as condoms and spermicides. After FDA-approval in 2023, the first ever daily oral contraceptive pill became available in stores and online in early 2024, making Opill the most effective form of contraception available over the counter. However, awareness of the new Opill is generally low, with a quarter (26%) of women 18 to 49 saying they have heard of the new daily oral contraceptive pill. Among those who have heard of it, just 4% have purchased it and an even smaller share (3%) have used or taken Opill since it became available in stores and online earlier in 2024.
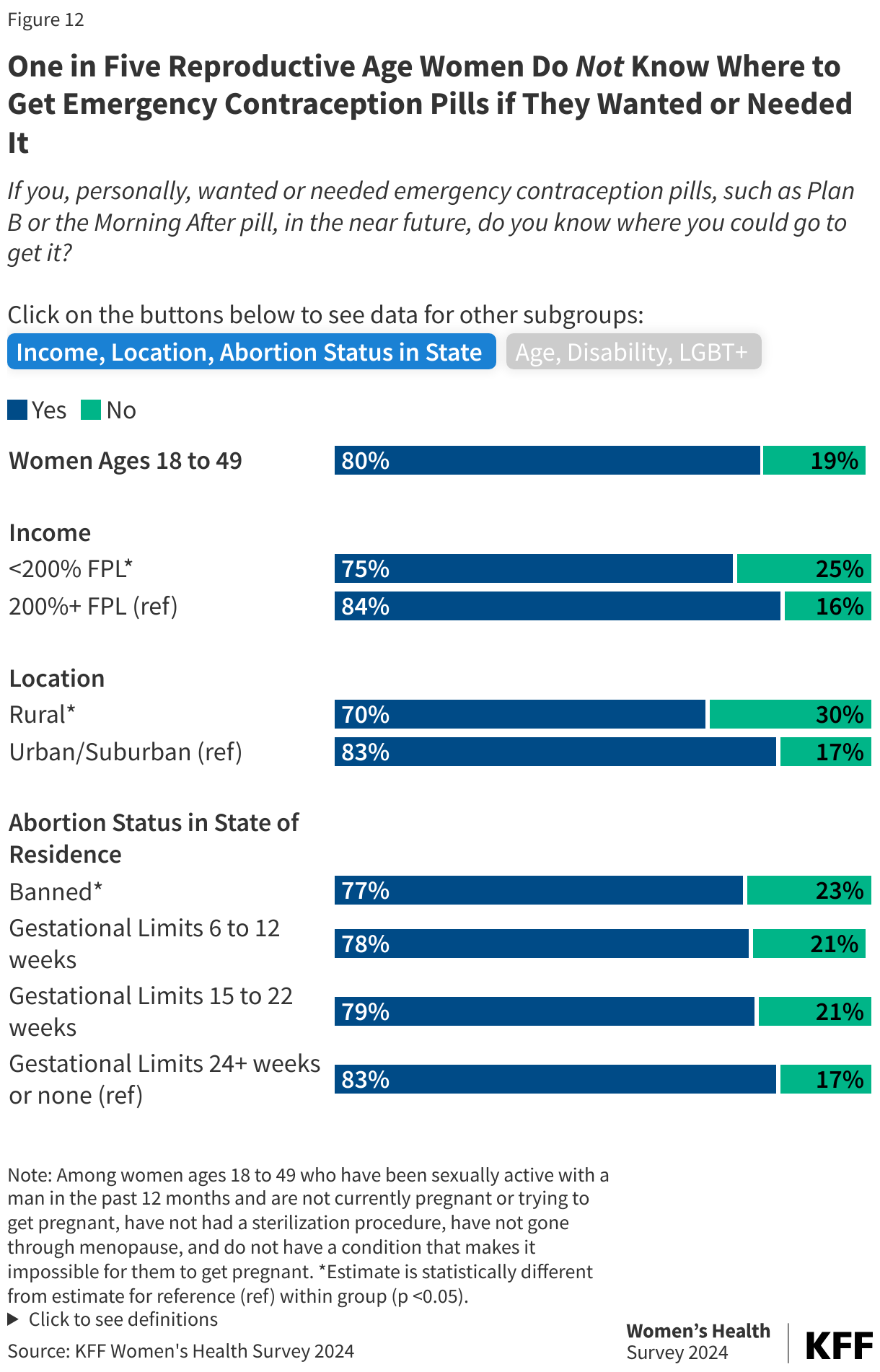
Emergency contraceptive pills have been available OTC since 2006, as well as through many doctors’ offices and clinics, however, one in five (19%) reproductive age women would not know where to get emergency contraception pills if they wanted or needed them in the near future (Figure 12). Higher shares of women with lower incomes compared to higher incomes (25% vs. 16%) and women living in rural areas compared to those living in urban or suburban areas (30% vs. 17%) say they would not know where to get emergency contraception pills if they wanted or needed them in near future. A higher share of women living in states where abortion is banned say they would not know where they could go to get emergency contraception compared to women living in states where abortion is generally available (23% vs. 17%).
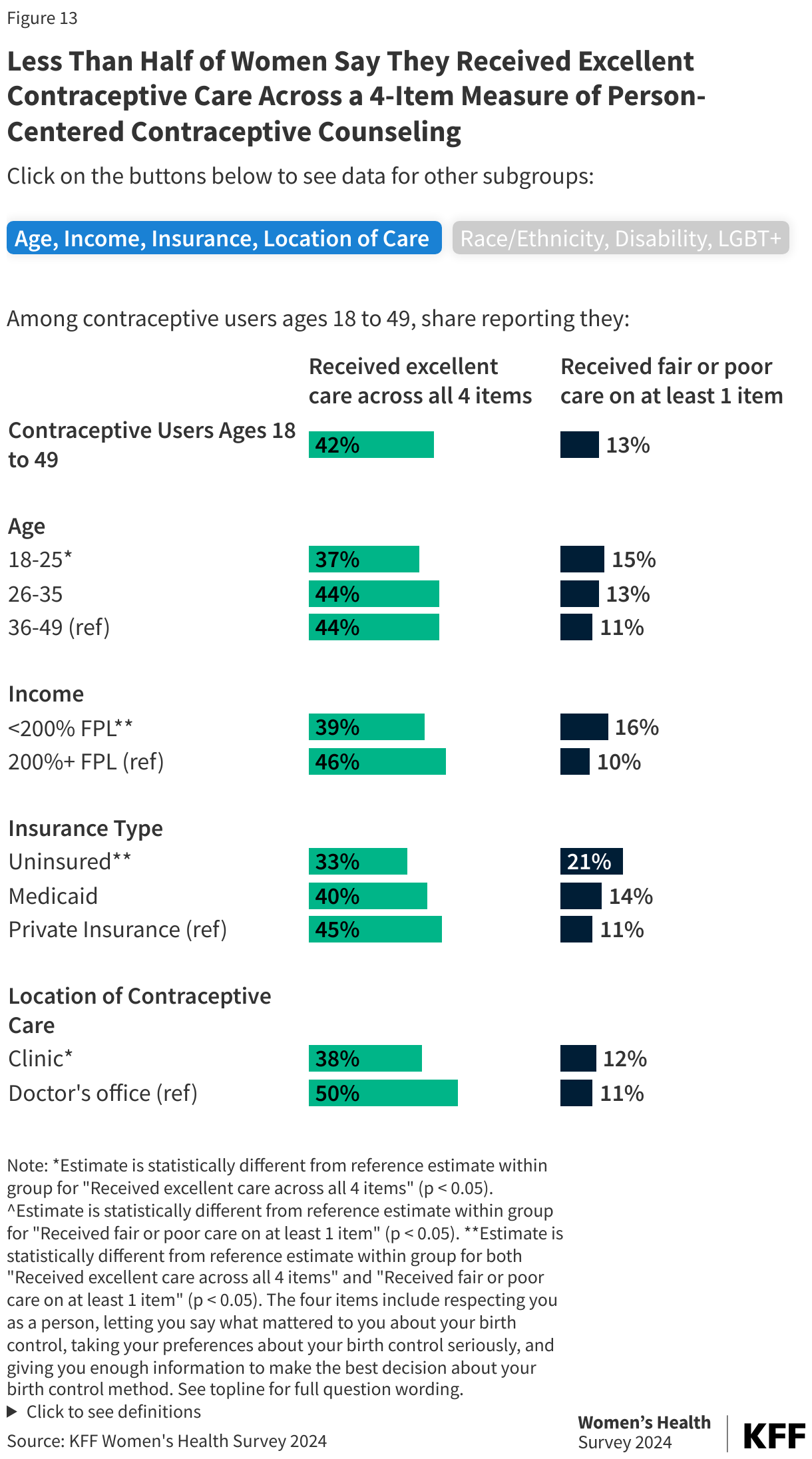
An important part of a contraceptive care visit is contraceptive counseling that is focused on a patient’s own needs, values, and preferences with regard to their contraceptive decision-making., referred to as person-centered contraceptive counseling. The quality of this counseling can be measured using a four-item survey that uses a 5-point scale and asks patients to rate the extent to which their provider respected them as a person, let them say what mattered to them about their birth control method, took their preferences about their birth control seriously, and gave them enough information to make the best decision about their birth control method. Using this measure, four in ten (42%) contraceptive users report receiving excellent person-centered contraceptive counseling across all dimensions (Figure 13). Smaller shares of women with low incomes compared to women with higher incomes rate their contraceptive counseling as excellent across all four items (39% vs. 49%). Only a third (33%) of women without insurance rate their contraceptive counseling as excellent compared to 45% of women with private insurance. Smaller shares of women receiving their contraceptive care at a clinic rate their contraceptive counseling as excellent compared to those getting care in a doctor’s office (38% vs. 49%) which disproportionately reflects the experiences of women who are low income or uninsured. Just over 10% of contraceptive users rated their provider as fair or poor on at least one of the four items of patient-centered contraceptive counseling. Higher shares of women with low incomes (16%) and uninsured women (21%), as well as one in five women with disabilities say they received fair or poor contraceptive counseling on at least one item.
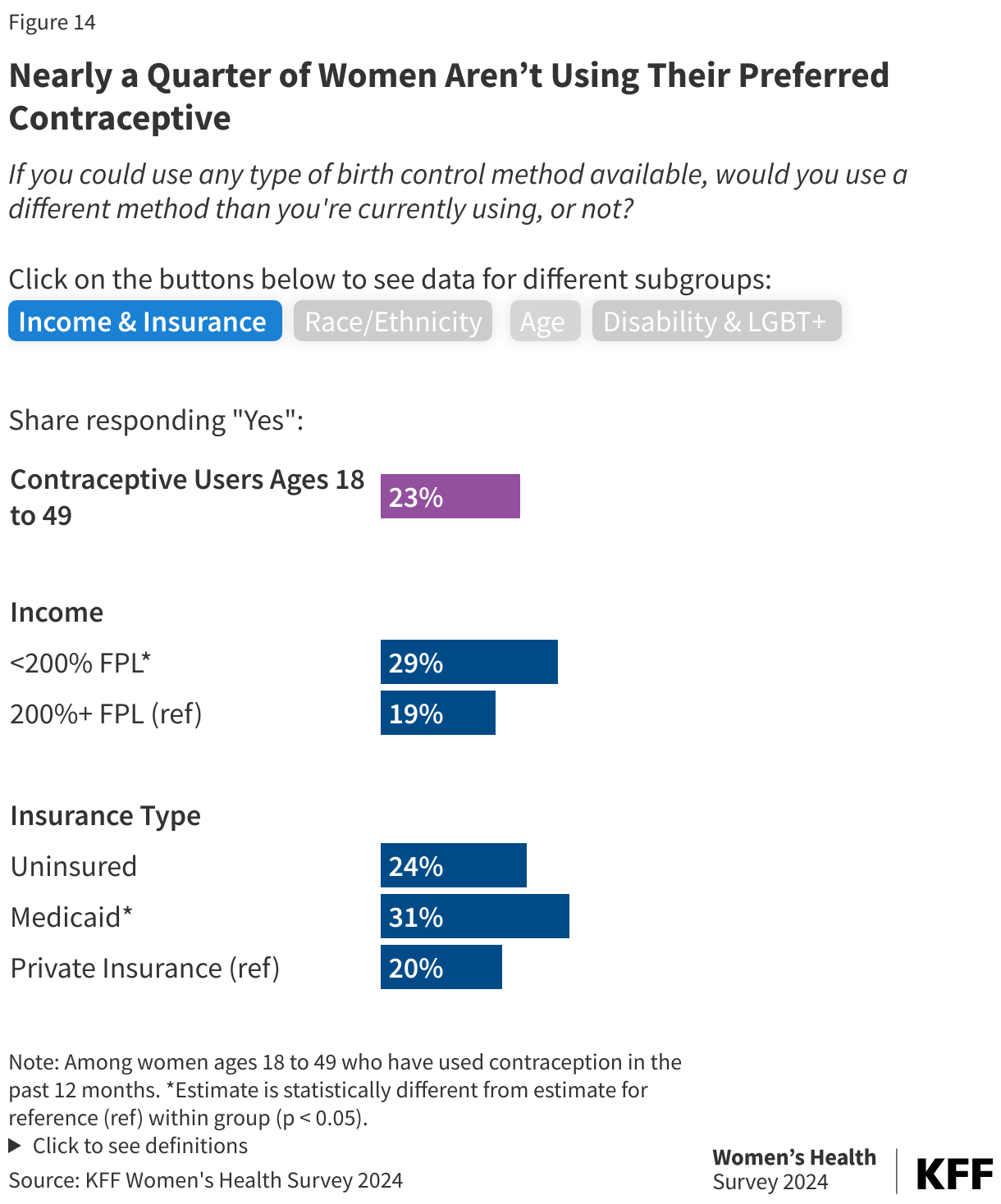
Part of person-centered contraceptive counseling is letting patients say what matters to them about their birth control method and taking their preferences about their birth control seriously. However, nearly a quarter (23%) of contraceptive users say if they could use any type of birth control method available, they would use a different method than the method they are currently using (Figure 14). This is similar across age groups and race/ethnicity. Larger shares of women with low incomes say that if they could use any type of birth control method available, they would use a different method than they are currently using compared to women with higher incomes (29% vs. 19%). Over three in ten (31%) women with Medicaid coverage say they would use a different method than the one they are currently using if they could use any method compared to one in five (20%) women with private insurance.
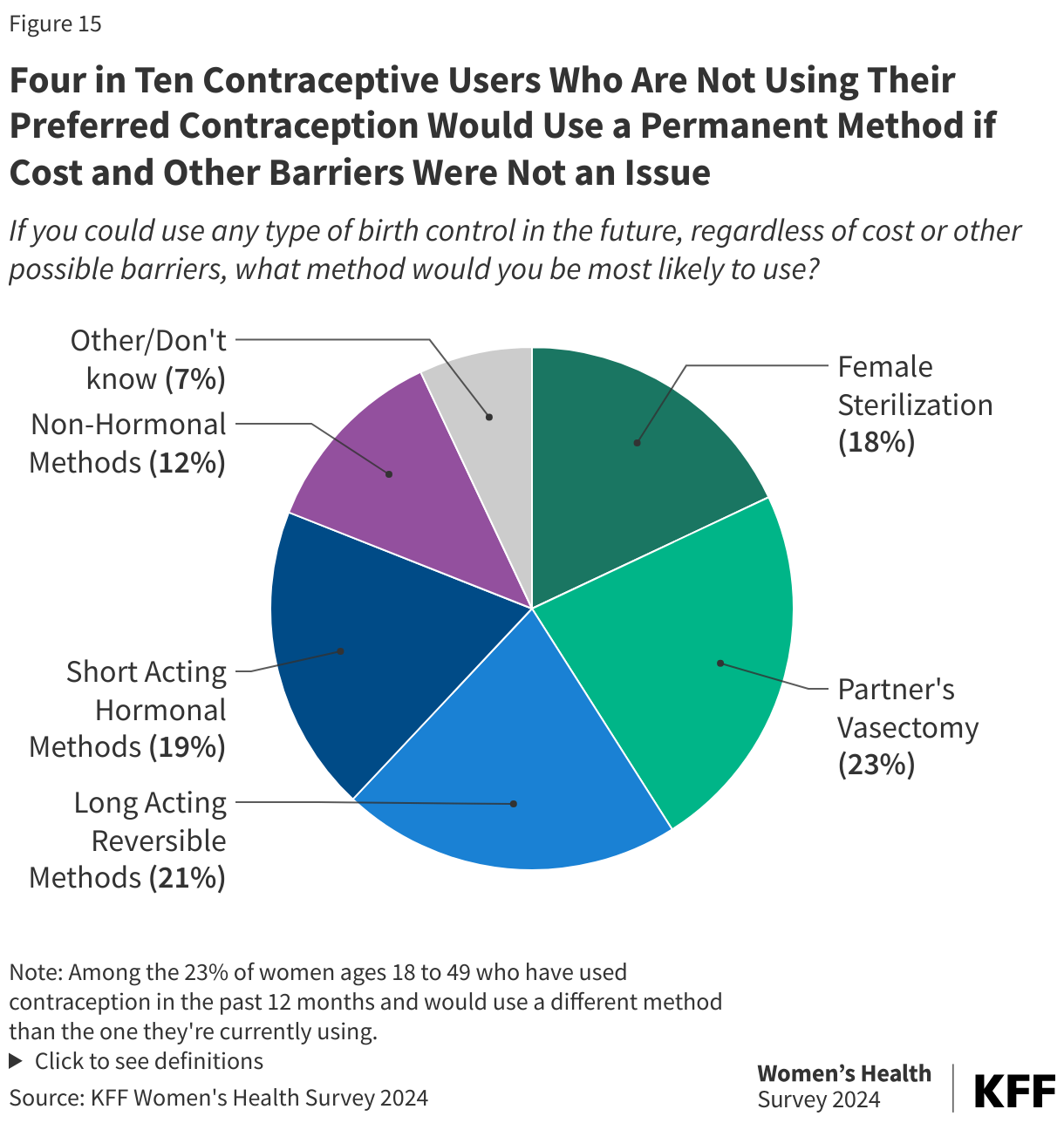
Among women who aren’t using their preferred method, nearly one in four (23%) say they would use a partner’s vasectomy if they could use any type of birth control, regardless of cost or other possible barriers (Figure 15). Contraceptive use is commonly the responsibility of women due to the extremely limited contraceptive methods available to men. For women or those who can get pregnant, avoiding pregnancy involves undergoing a procedure, or remembering to take a pill every day, or tracking one’s cycle and for many, living with side effects. Having the ability to rely on a partner’s vasectomy can take some of the burden off those who are capable of becoming pregnant. Nearly one in five (18%) women who aren’t using their preferred method (23% of contraceptive users) say they would choose to be sterilized, while 21% would use a long-acting reversible method, such as an IUD (14%) or implant (7%). These long-acting methods can be appealing because they can be used for three to ten years and don’t rely on regularly remembering to take a daily pill or get a periodic injection in the case of short acting hormonal methods. Among those who are not using their preferred method one in five (19%) women would use a short acting hormonal method, such as pills (8%), injectables (5%), patch (2%), ring (2%), and emergency contraception (2%). While one in ten (12%) would choose a non-hormonal method, including male condoms (6%), withdrawal (3%), and fertility awareness-based methods (3%).
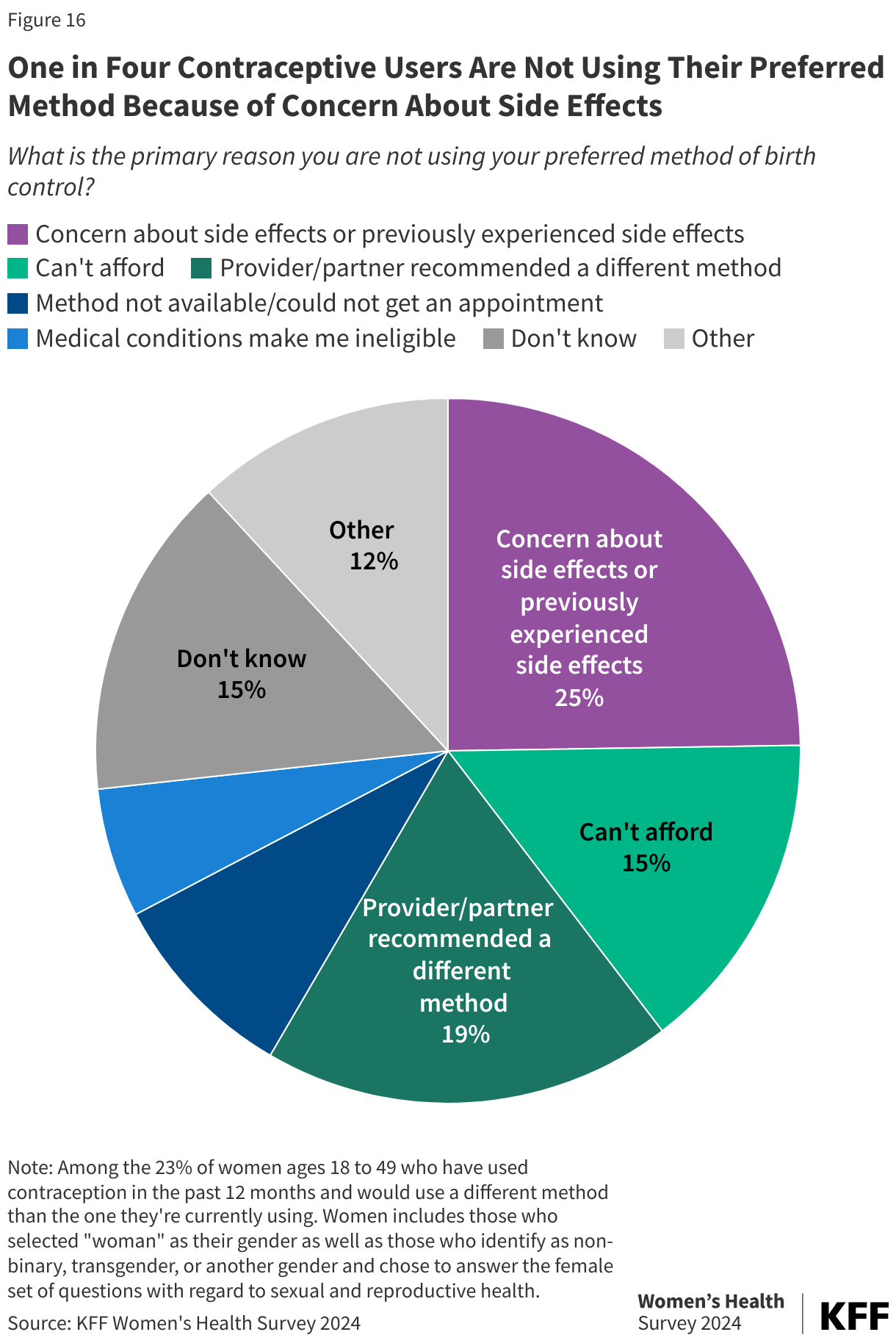
Concern about side effects or previously experienced side effects are leading reasons women are not using their preferred method of birth control, with a quarter (25%) of women who are not using their preferred method citing this as the reason (Figure 16). Over four in ten (44%) Black women who are not using their preferred method say concern about side effects is the primary reason compared to 18% of White women. Some of the other top reasons women are not using their preferred method include inability to afford their preferred method (15%), their provider recommending a different method (10%), or their partner not wanting them to use their preferred method (8%).
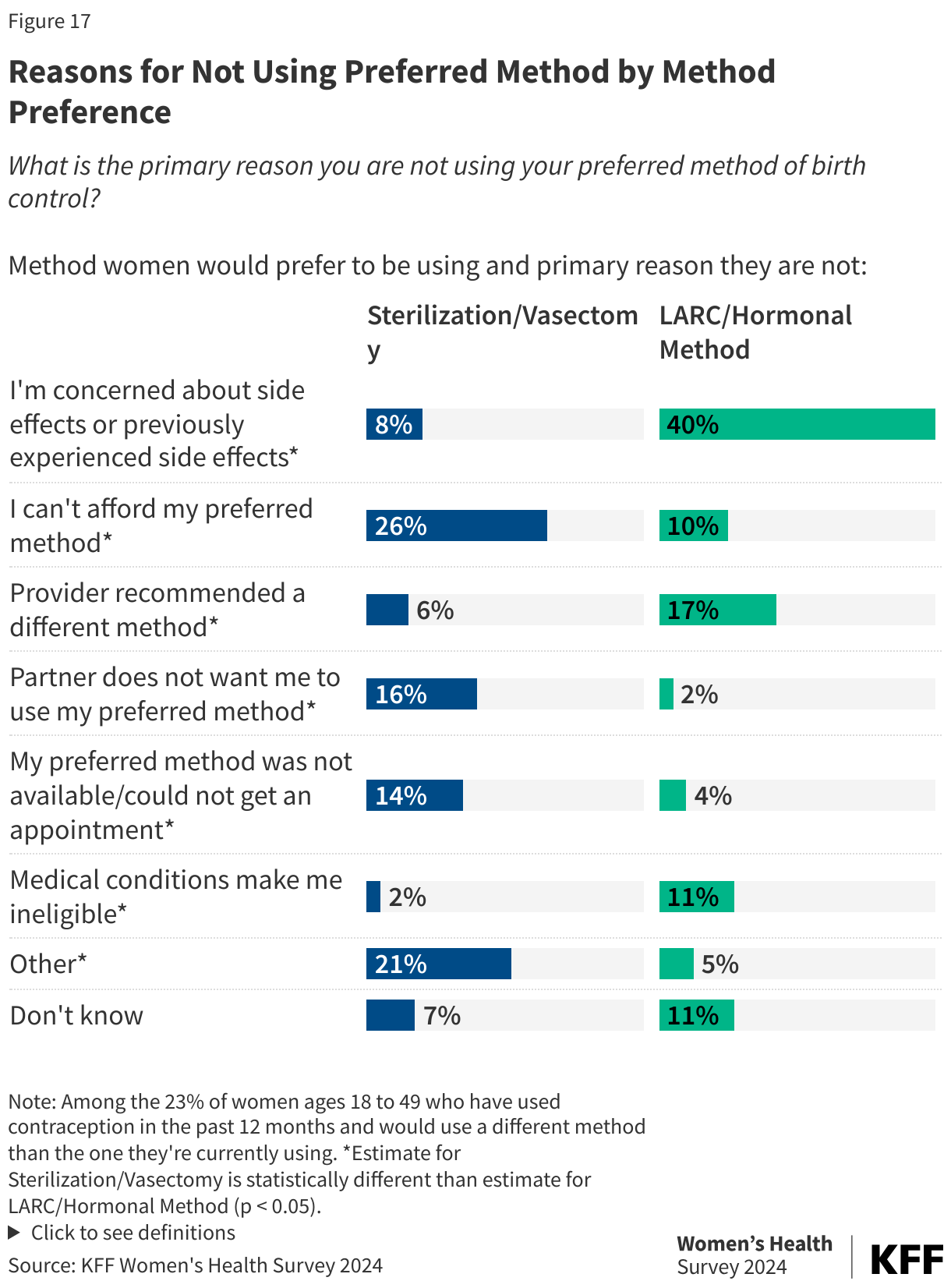
The primary reasons for not using their preferred method of birth control depends on the method they prefer to be using. For those who prefer to be using a permanent method, such as female sterilization or a partner’s vasectomy, the top reasons they are not using these methods is affordability (26%) and their partner does not want them to use this method (16%) (Figure 17). Among those who prefer to be using a long-acting contraceptive or hormonal method, four in ten (40%) cite concern about side effects, 17% say their provider recommended a different method, 11% say medical conditions make them ineligible, and 10% can’t afford their preferred method.