The Biden Administration’s Final Rule on Section 1557 Non-Discrimination Regulations Under the ACA
This brief provides an overview of the Biden Administration 2024 final rule implementing Section 1557 of the ACA, which is home to the law’s major nondiscrimination provisions. While Section 1557’s protections took effect when the ACA was enacted in 2010, much of its reach has been determined by implementation guidance issued across different Presidential administrations, often reflecting conflicting views. The final rule reinstates and expands upon many of the 2016 regulations from the Obama Administration and is a reversal from much of the 2020 Trump Administration rule. We provide a brief background on 1557 rulemaking and identify key differences between this rule and the 2020 rule. We also highlight two areas of growing interest impacted by the rule – nondiscrimination protections for pregnancy related decisions, past, present and future, including abortion, and for transgender people. Despite the issuance of the final rule, debates about 1557’s protections, and ensuing litigation, continue and will be particularly dependent on the outcome of the 2024 Presidential election.
Introduction
On April 27, 2024, the Biden Administration’s Department of Health and Human Services (HHS) finalized long-awaited revised regulations implementing Section 1557 of the Affordable Care Act (ACA). Section 1557 prohibits discrimination on the basis of race, color, national origin, age, disability, or sex and applies to health programs and activities receiving federal financial assistance (referred to as covered entities). In broad terms, it prevents covered entities from discriminating against certain protected groups in providing health care services, insurance coverage and program participation. The rule has staggered effective dates starting on July 5, 2024. In broad terms, 1557 provides nondiscrimination health care protections to individuals in protected groups, including prohibiting denial of benefits, coverage, program participation, and otherwise unequal treatment based on these factors
The administration also released a FAQ and press release. Section 1557 houses the law’s major nondiscrimination provisions by incorporating protections from existing civil rights laws. These laws include Title VI of the Civil Rights Act of 1964 (race, color, and national origin), Title IX of the Education Amendments of 1972 (sex), the Age Discrimination Act of 1975, and Section 504 of the Rehabilitation Act of 1973 (disability). Notably, Section 1557 is the first federal civil rights law to prohibit discrimination on the basis of sex in health care.
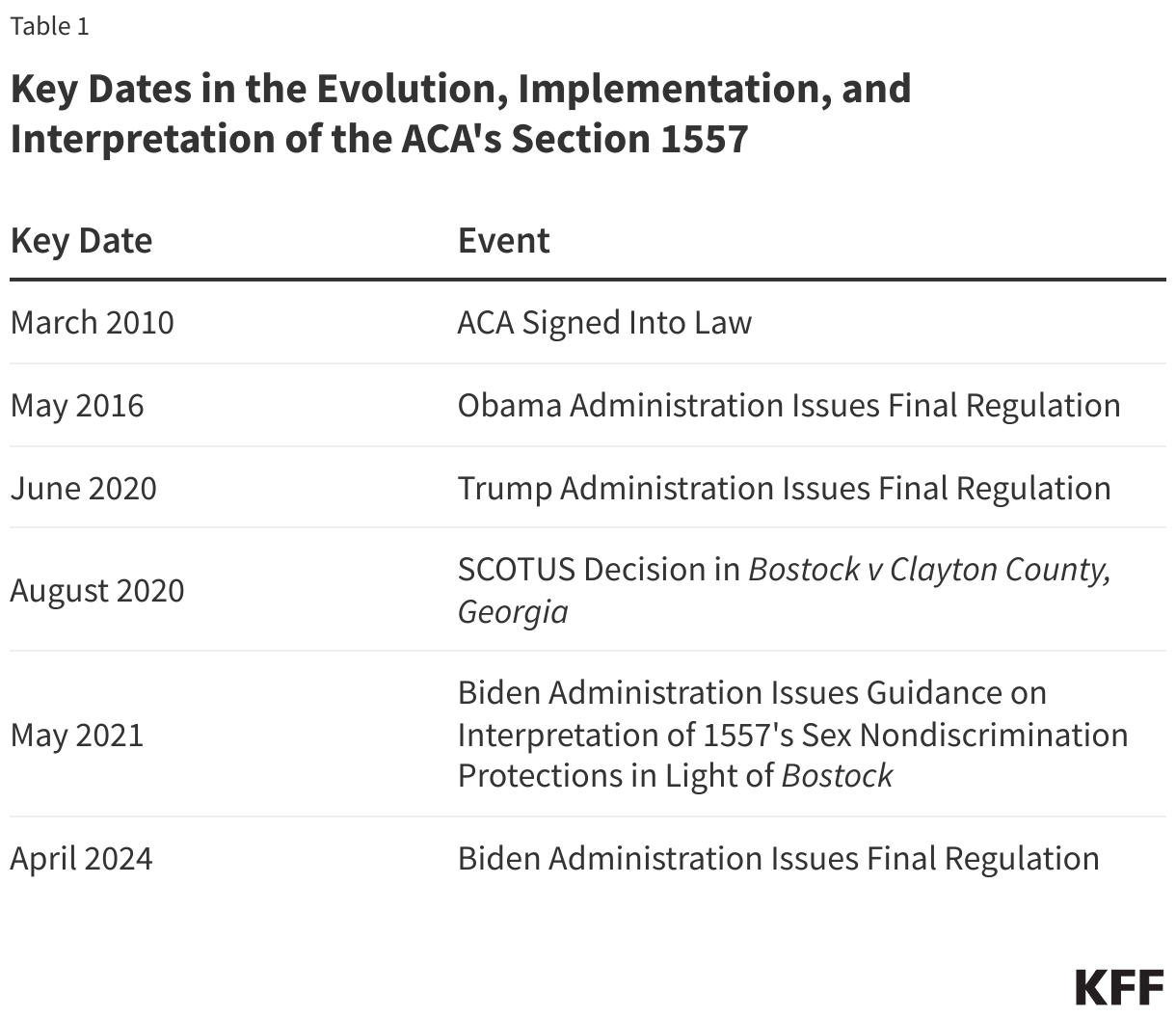
Section 1557’s protections took effect when the ACA was enacted on March 23, 2010, but much of the law’s reach has been determined by implementation guidance issued by different Presidential administrations, reflecting different interpretations and priorities. Across the Obama, Trump, and Biden administrations, the 1557 implementing regulations have volleyed back and forth in their interpretations, particularly related to the scope of entities covered by the law and the law’s ability to provide nondiscrimination protections based on sexual orientation and gender identity and pregnancy related conditions. These debates, and ensuing litigation, are likely to continue, and will be particularly dependent on the outcome of the 2024 Presidential election.
Most of the implementing regulations in the new rule are effective 60 days (July 5, 2024) after publication in the Federal Register (May 6. 2024). Some provisions impacting health insurance plan design won’t become effective until the plan year beginning after January 1, 2025, and other provisions where entities might need additional time to amend current practices also have later effective dates. (The rule and the FAQ provide a table of these dates.)
The FAQ accompanying the rule states it was necessary to issue this guidance “to restore and strengthen civil rights protections for individuals consistent with…the statutory text,” noting that the 2020 Trump Administration rule “covers fewer programs and services and limited nondiscrimination protections for individuals.”
Section 1557 has been subject to a wave of litigation across administrations. Litigation has both centered on rulemaking and on the statue itself. In some cases (e.g. Franciscan Alliance v. Azar), courts have found narrowly in favor of plaintiffs who have asserted that the requirement to cover or provide certain services, such as those related to termination of pregnancy or gender affirming care, violated their sincerely held religious beliefs and thus religious freedom protections. In other cases, courts have found that Section 1557 protects access to these same services, such as by requiring state Medicaid programs to cover gender affirming care (e.g. Flack v. Wisconsin). Courts have also weighed in on the legality of aspects of rulemaking (e.g. Whitman-Walker Clinic v. HHS) and litigation has already been filed in the state of Florida by the attorney general and a Catholic hospital group challenging the new rule (see State of Florida et al v. HHS et al.) In addition, litigation related to other civil rights protections (Bostock v Clayton County, Georgia) has implications for Section 1557 and, in particular, this regulation’s interpretation of nondiscrimination based on sex. (Box 1)
Box 1: Impact of Bostock v Clayton County, Georgia on Section 1557
In June 2020, just three days after the Trump Administration rule was finalized, the Supreme Court ruled in Bostock v Clayton County, Georgia that in the context of employment, discrimination based on sex encompasses sexual orientation and gender identity. The Bostock ruling does not directly apply to 1557 because it was based on interpretation of sex protections under Title VII and the 1557 sex protections are pulled in through Title IX. However, courts have historically looked to Title VII in interpreting Title IX, including in cases where plaintiffs challenged the Trump-era rule. As such, prior to issuing the new regulation, the Biden Administration issued guidance in May 2021 stating it would interpret and enforce 1557’s sex nondiscrimination provisions to include protections on the basis of sexual orientation and gender identity in light of and consistent with Bostock.
Summary of Major Changes
The final rule closely mirrors a proposed rule issued by the Biden administration in July of 2022 and is, in many ways, a reversal of the final rule issued by the Trump Administration in June of 2020, which itself was a significant departure from the Obama Administration regulations issued in 2016. This final rule reinstates and expands upon much of those 2016 regulations. Compared to the previous rules, key changes in the Biden Administration final rule include:
- Section 1557 applies to health programs or activities that receive direct or indirect federal financial assistance from HHS, health programs and activities administered by HHS, and Therefore, covered entities include state Medicaid agencies, Medicare, many health insurance plans, and most hospitals and providers, among others. The new rule expands on the types of entities subject to 1557 compared to the Trump rule, including by determining that 1557 protections apply to products sold by issuers with plans on the marketplaces (not just the marketplace plans themselves) and by considering Medicare Part B as receiving Federal financial assistance for the first time;
- Provides nondiscrimination protections for those who experience discrimination on the basis of multiple protected characteristics. (A new protection compared to both the Obama and Trump rules);
- Explicitly provides for nondiscrimination protections based on gender identity and sexual orientation, sex characteristics (including intersex traits), and pregnancy related conditions including pregnancy termination, as well as related specific health insurance coverage protections, expanding these moderately compared to the Obama rule and completely compared to the Trump rule;
- Provides specific nondiscrimination protections for transgender people’s access to care and coverage, expanding moderately on those in the Obama rule and completely compared to the Trump rule. The rule requires people be treated consistently with their gender identity, prohibits the denial of gender affirming care when provided for other purposes, if the denial is on the basis of sex, and the categorical exclusion of gender affirming care. (See box 3 for additional details related to this provision);
- Protects patients from discrimination on the basis of actual or perceived abortions but states it is not a violation of Section 1557 if providers do not provide abortions unless the provider does not do so based on an individual’s protected status (e.g. race, age, etc.) (See box 2 for additional details related to this provision);
- Removes explicit blanket abortion and religious freedom exemptions which the Trump rule incorporated through Title IX’s religious exemptions, stating instead that robust religious freedom protections exist outside of Section 1557 and that incorporation of Title IX exemptions through the rule is not necessary;
- Adopts a new religious freedom and conscience protections exemptions process;
- The new rule reinstates explicit prohibitions on discrimination based on gender identity and sexual orientation that had existed in ten other federal regulations outside Section 1557. The protections were put in place through Obama Administration regulations and related to coverage, access, and marketing, in Medicaid, private insurance, and the Marketplaces but were eliminated in the Trump Administration’s 1557 rule.;
- Expands protections for those with limited English proficiency (including in telehealth) compared to both prior rules;
- Includes new provisions for services requirements and notices related to language access and access to auxiliary aids and services, and adopts new policies and staffing requirements for 1557 compliance;
- Reaffirms most requirements related to disability discrimination from the 2016 rule, which complement a new rule on web accessibility for public entities under the Americans with Disabilities Act and major updates to regulations implementing Section 504 of the Rehabilitation Act, which were last updated in 1977. Section 504 prohibits recipients of federal funding, including publicly-subsidized health payers and health care providers who accept Medicare or Medicaid, from discriminating against people on the basis of disability. Among other changes, the Section 504 health provisions address discrimination in medical treatment, create enforceable standards for medical equipment, address accessible web content and mobile apps, and codify the Olmstead requirement to serve people with disabilities in the most integrated setting that is appropriate.
- Reflecting emerging technologies, for the first time, addresses and applies Section 1557 nondiscrimination protections to the use of telehealth and patient care decision support tools, including in addressing bias in clinical algorithms and other tools and in the use of AI.
Box 2: Abortion – Protections from Sex Discrimination Includes Pregnancy Termination
The ACA protects providers and programs based on their willingness to provide, pay for, cover, or refer for abortion or to provide or participate in such trainings. The new final Section 1557 rule includes protections for patients on discrimination on the basis of having had actual or perceived abortions. OCR explains that a covered provider’s decision not to provide an abortion is not a violation of Section 1557 unless the provider chooses not to provide abortion for a particular individual based on a protected ground such as race. Some commenters “expressed concern that Dobbs created tension between health providers, and patients, increasing distrust in providers and that it has created chaos in the health care system. They state this has increased the risk that patients will experience discriminatory care and suffer delays in lifesaving treatment as a direct result of legal and medical uncertainty. These commenters said that discrimination in care propagates more distrust, which is a significant barrier for individuals seeking care and is precisely what section 1557 was designed to protect against.” OCR responded to these concerns noting that it is considering revisions to the HIPAA Privacy Rule to strengthen privacy protections for individuals’ protected health information related to reproductive health care.
Box 3: Care and Access for Transgender People – Protections from Sex Discrimination Include Gender Identity
Section 1557’s regulatory treatment of sexual orientation and gender identity has changed considerably over time. The 2016 Obama Administration rule interpreted sex nondiscrimination protections to include gender identity and sex stereotyping (among other identities) but not sexual orientation. At that time, HHS stated it would “evaluate complaints alleging sex discrimination … sexual orientation” on a case-by-case basis and anticipated that case law would evolve as to clarify whether sexual orientation could be covered. The Trump Administration did not define sex in the regulatory text but in the preamble suggested it would interpret sex to mean only biological sex assigned at birth. The Biden Administration interpreted sex to include sexual orientation and gender identity (among other identities), reaffirming its earlier guidance which took the same approach, in light of Bostock (see Box 1). It also extends these protections to include intersex people for the first time.
As noted above, the new rule also reinstates explicit prohibitions on discrimination based on gender identity and sexual orientation in regulations outside of Section 1557 that had been put in by the Obama Administration but eliminated through the Trump Administration’s 1557 rule.
***
In addition, the rule, in text and preamble, spells out specific protections for transgender people and access to gender affirming care including that entities cannot refuse gender affirming care services that would be provided to an individual for other purposes, if the limitation is based on sex or gender and that the categorical exclusions of gender affirming care is prohibited. It does not prohibit nondiscriminatory denial of services with the preamble noting “OCR has a general practice of deferring to a clinician’s judgment about whether a particular service is medically appropriate for an individual, or whether the clinician has the appropriate expertise.” OCR states any investigations will not focus on clinical judgment per se but rather whether that judgment reflects unlawful bias, The rule also does not prevent a covered entity from availing itself of religious freedom and creates new pathways for asserting such protections. (Additional details in Table 1.)
***
Some commenters had specific concerns regarding the rule’s application to “State laws that prohibit access to gender-affirming care…” OCR responded that “some States may have laws…that are contrary to the final rule’s nondiscrimination protections, and…section 1557 preempts those laws.” The conflict between state and federal law in this case is unresolved and the Florida Attorney General, along with a Catholic medical group, has filed suit alleging that the rule requires providers to provide gender affirming care and violates protections.
Table 2 summarizes the major provisions of HHS’s new final rule and provides a side-by-side comparison to the Obama (2016) and Trump (2020) administration rules.
