Health Insurer Financial Performance in 2023
The largest private health insurance companies often offer plans in multiple markets, including the Medicare Advantage, Medicaid managed care, individual (non-group), and fully insured group (employer) health insurance markets. Each market has unique features, including eligibility, payment, and coverage rules, which affect insurers’ overhead and potential profit. In recent years, private insurers are playing a growing role in public insurance programs, with more than half of eligible Medicare beneficiaries enrolled in a private Medicare Advantage plan and nearly three-quarters of Medicaid enrollees obtaining coverage through a managed care plan (typically a private insurer).
This brief examines two measures of financial performance – gross margins and medical loss ratios – in the Medicare Advantage, Medicaid managed care, individual, and fully insured group health insurance markets using data reported by insurance companies to the National Association of Insurance Commissioners (NAIC) and compiled by Mark Farrah Associates, through the end 2023 (the most recent year of annual data).
In 2023, per enrollee gross margins were highest in the Medicare Advantage market, and medical loss ratios were lowest in the individual insurance market. While both gross margins and medical loss ratios are indicators of financial performance, higher margins and lower loss ratios do not necessarily translate into greater profitability since they do not account for administrative expenses or tax liabilities. Additionally, the increasingly complex structure of insurance companies, including the rise in consolidation and vertical integration, and role of subsidiaries, make it difficult to isolate the revenues and expenses associated with a particular insurance market. (A detailed description of each market is included in the Appendix).
Measures of Financial Performance in 2023
Gross margins
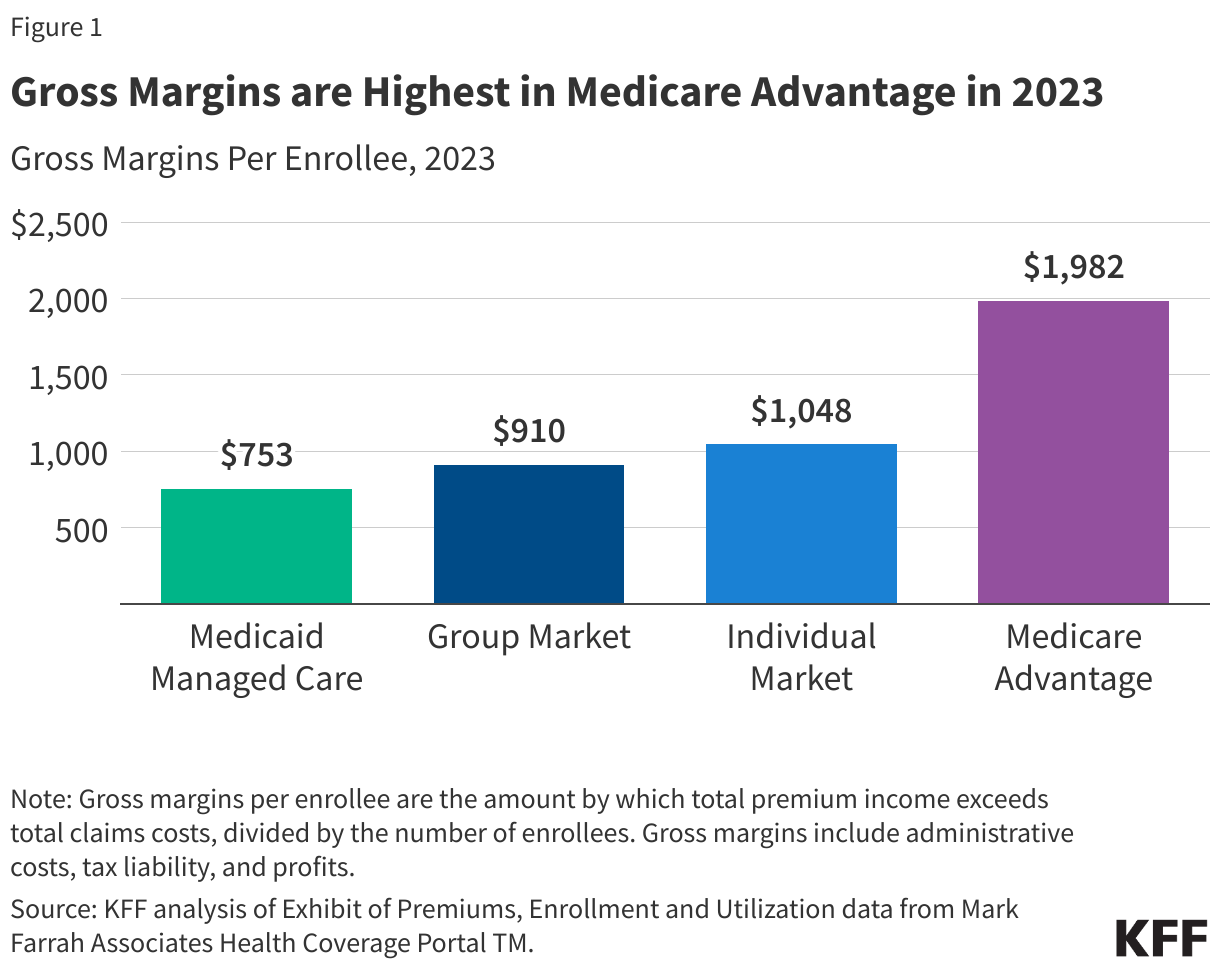
The gross margin per enrollee is the amount by which total premium income exceeds total claims costs per person over a specified time period (i.e., per year).
At the end of 2023, gross margins per enrollee ranged from $753 in the Medicaid managed care market to $1,982 in the Medicare Advantage market. Gross margins per enrollee in the group and individual markets were $910 and $1,048, respectively, roughly half the level observed among Medicare Advantage plans on average. The level of margins reflect, in part, the overall health needs and spending in a market segment. A similar margin in percentage terms will translate to a higher margin in dollars per enrollee when average health expenses are higher.
Medical loss ratios
Another way to assess insurer financial performance is to look at medical loss ratios (MLRs), or the percent of premium income that insurers pay out in the form of medical claims. Generally, lower MLRs mean that insurers have a higher share of income remaining after paying medical costs to use for administrative costs or keep as profits. Each health insurance market has different administrative needs and costs, so a lower MLR in one market does not necessarily mean that market is more profitable than another market.
MLRs are used in state and federal insurance regulation in a variety of ways. In the commercial insurance (individual and group) markets, insurers must issue rebates to individuals and businesses if their MLRs fail to reach minimum standards set by the ACA. Medicare Advantage insurers are required to report MLRs at the contract level (which typically combines multiple plans) and are required to issue rebates to the federal government if their MLRs fall short of required levels and are subject to additional penalties if they fail to meet MLR requirements for multiple consecutive years. For Medicaid managed care organizations (MCOs), CMS requires states to develop capitation rates for Medicaid to achieve an MLR of at least 85%. There is no federal requirement for Medicaid plans to pay remittances if they fail to meet their MLR threshold, but a majority of states that contract with MCOs require remittances in at least some cases. The 2024 Consolidated Appropriations Act includes a financial incentive to encourage certain states to collect remittances from Medicaid MCOs that do not meet minimum MLR requirements.
The MLRs shown in this issue brief are simple loss ratios (claims as a share of premium income) and differ from the definition of MLR in the ACA and in Medicaid managed care, which makes some adjustments for quality improvement and taxes, and do not account for reinsurance, risk corridors, or risk adjustment payments.
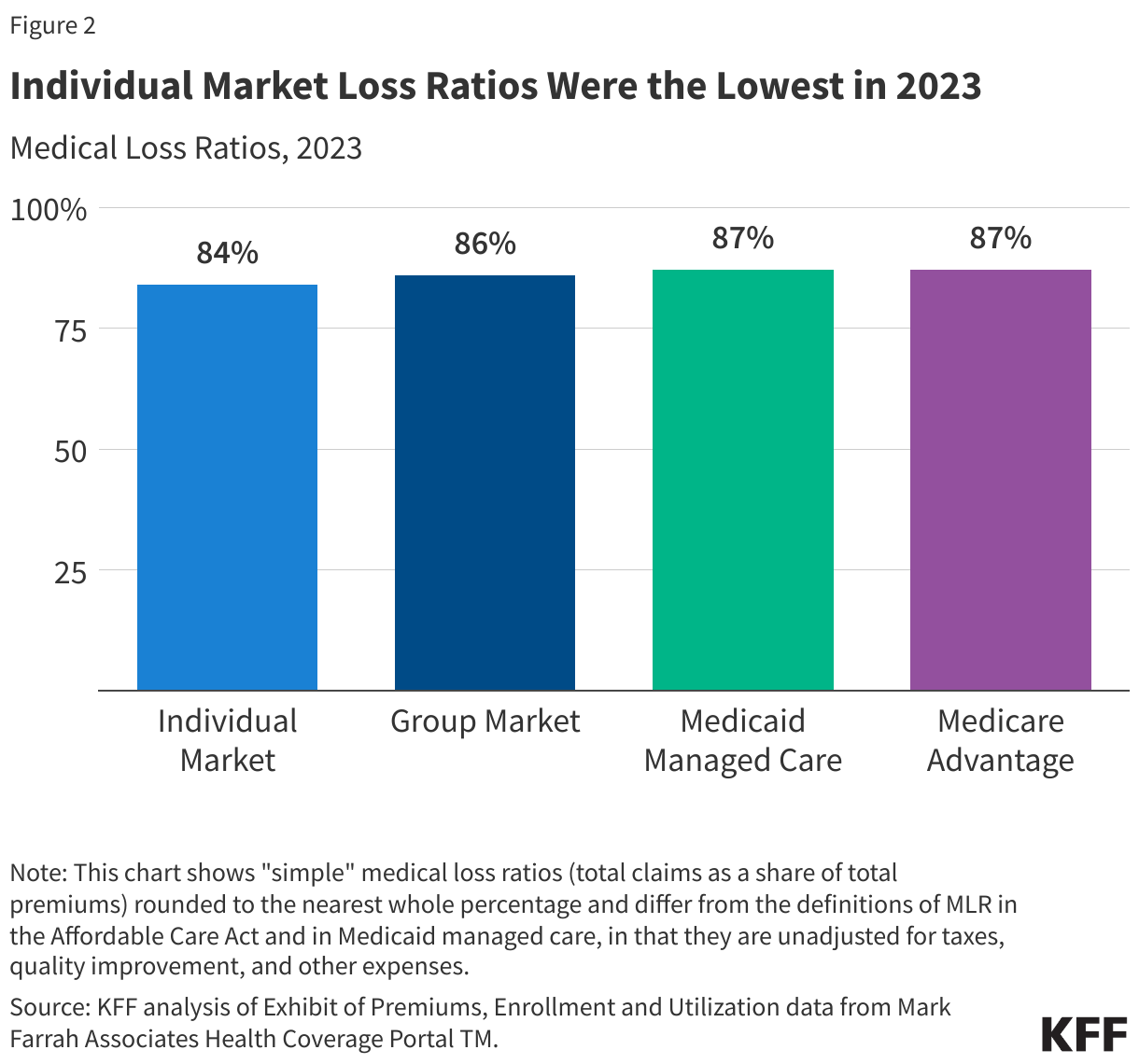
In 2023, MLRs were similar across the group, Medicare Advantage, and Medicaid managed care markets and somewhat lower in the individual market. Simple loss ratios were around 84% in individual market, 86% in the fully insured (group) market, and 87% in the Medicaid managed care and Medicare Advantage markets.
Trends in Gross Margins
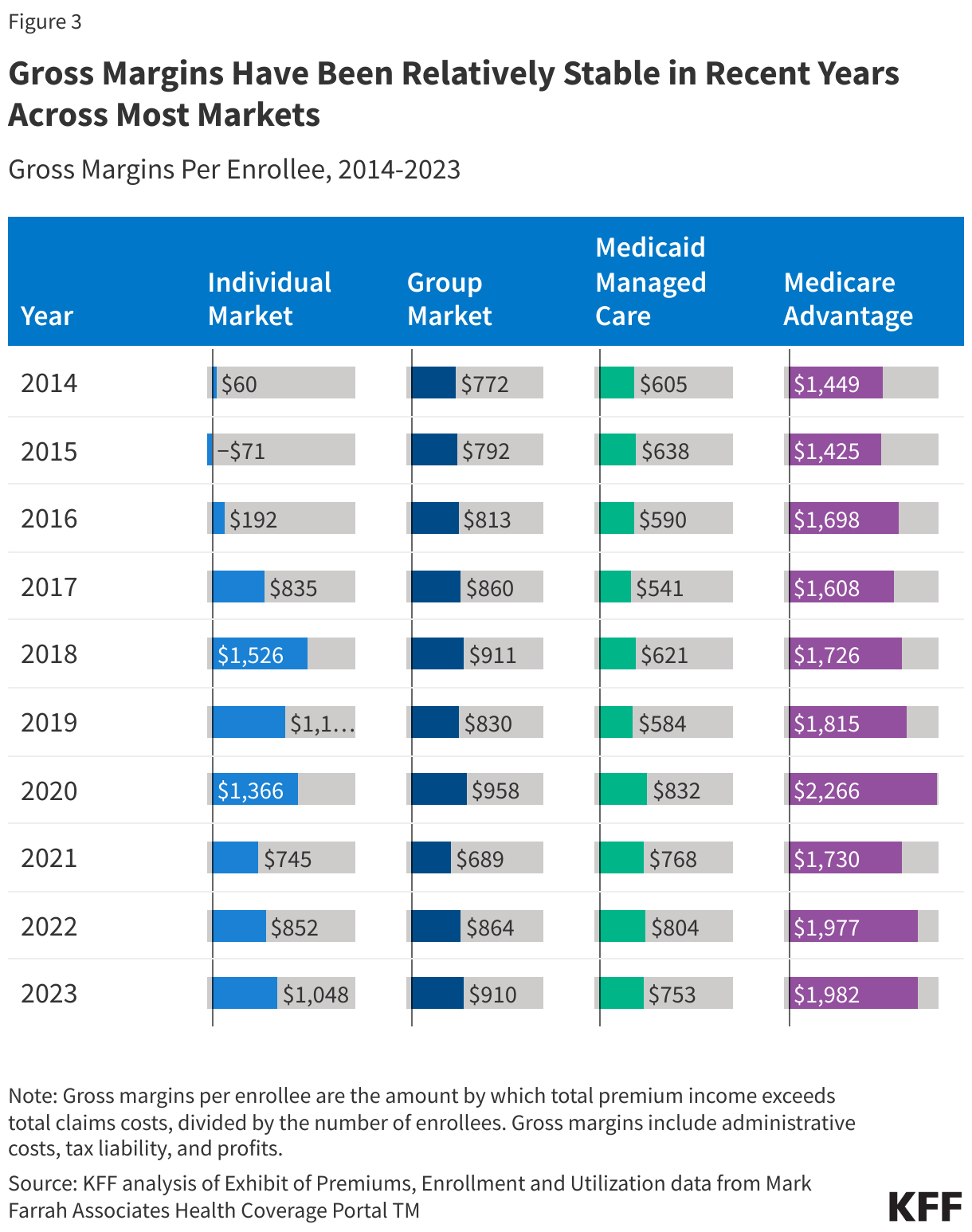
While gross margins are not equivalent to profitability, changes in gross margins can be indicative of changes in profitability (assuming administrative costs and tax liability are stable). Across most markets, gross margins have been relatively stable in recent years, though they have declined somewhat from spikes that occurred in 2020 during the initial phase of the COVID-19 pandemic.
Medicare Advantage: Through the end of 2023, gross margins in the Medicare Advantage market averaged $1,982 per enrollee, which was similar to 2022 ($1,977), despite reports by the largest Medicare Advantage insurers of higher-than-expected utilization at the end of 2023. Potentially spurred by the prospect of strong financial returns, the Medicare Advantage market has grown substantially in the last decade, with more than 50% of eligible beneficiaries enrolled in a Medicare Advantage plan in 2023.
Group Market: Gross margins for fully insured group plans declined significantly from 2020 to 2021 (the lowest in the past decade) but have been increasing in subsequent years. In 2023, per enrollee gross margins in the group market were nearly the same as those in 2018.
Individual Market: Individual market gross margins were about 31% and 10% lower in 2023 than in 2018 and 2019, respectively. In 2018, following efforts to repeal the ACA and defunding of Cost Sharing Reduction subsidies, insurers raised individual market premiums substantially. These premium increases resulted in significantly higher margins than in earlier years (Figure 3).
Medicaid Managed Care: Per enrollee gross margins in the Medicaid managed care market decreased by 6% from 2022 to 2023 but remained higher than pre-pandemic levels. Starting in April 2023, pandemic-era policies that allowed for “continuous enrollment” in Medicaid ended and states began reviewing eligibility and disenrolling individuals who were no longer eligible or who did not complete the renewal process. National data show total Medicaid/CHIP enrollment declined by more than 9% (about 9 million people) from March 2023 to December 2023. Medicaid managed care plans expected the overall risk profile (or “acuity”) of its members to worsen during unwinding, as they anticipated “stayers” would be sicker than “leavers,” which may have contributed to the decrease in per enrollee gross margins seen from 2022 to 2023. States may use a variety of risk mitigation strategies to provide financial protection and limits on financial risk for states and plans that may not be accounted for in the data used in this analysis. Many states implemented COVID-19 related risk corridors (where states and health plans agree to share profit or losses) allowing for the recoupment of payments made for 2020, 2021, and 2022. Gross margins reported may not reflect recoupments of funds that may occur after the reporting period.
Trends in Medical Loss Ratios
Each health insurance market has different administrative needs and costs, so similar MLRs do not imply that the markets are similar to each other in profitability. Additionally, simple MLRs examined in this brief do not incorporate the effects of changes in tax law, such as the health insurer tax, which has been permanently repealed starting in 2021, was in effect in 2018 and 2020, but was not in 2019. While MLRs alone cannot convey whether a market is profitable in a particular year, if administrative costs hold mostly constant from one year to the next, a change in the MLR could imply a change in profitability.
Individual Market: The average individual market MLR in 2023 was lower than in 2021 and 2022 but higher than those seen in the years leading up to the pandemic. As mentioned earlier, 2018 and 2019 were exceptionally lucrative years for the individual market. Many plans fell short of the ACA’s MLR requirements and were therefore required to issue large rebates to consumers based on their 2018 and 2019 experience.
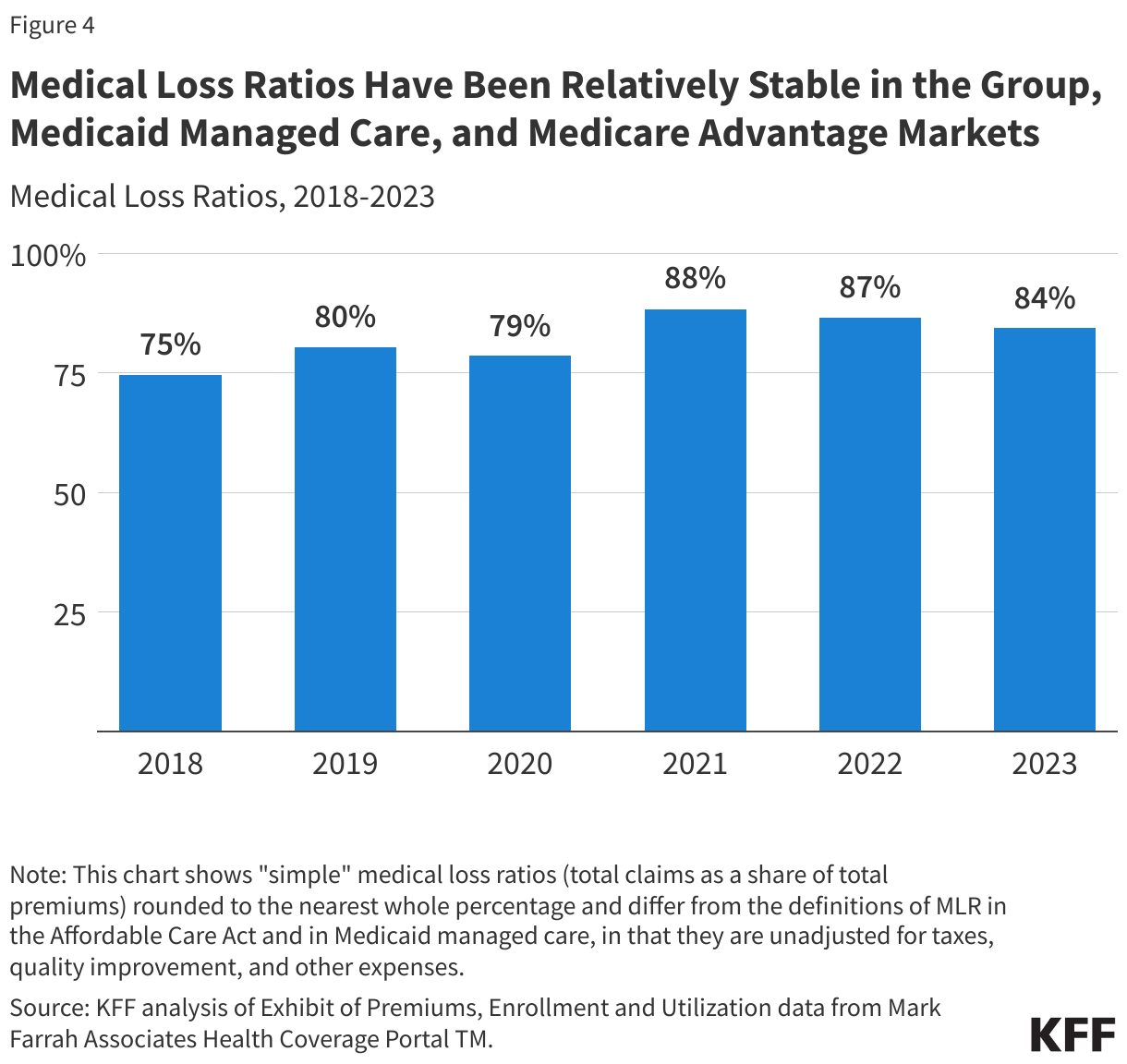
Group Market: The average MLR for group plans was stable between 2022 and 2023 at 86%, and slightly below the average of 88% in 2021. These are all higher than previous years, when MLRs ranged from 83% in 2018 and 2020 to 85% in 2019.
Medicaid Managed Care: Relative to 2022, the average MLR in 2023 for the Medicaid managed care market increased slightly from 86% to 87% (implying a potential decrease in profitability) but remained lower than in 2018 and 2019. State Medicaid programs and managed care plans continue to be in a period of heightened uncertainty as unwinding continues. States and plans will be closely monitoring disenrollments and “churn” (off and on the program) as well as new utilization and acuity trends.
Medicare Advantage: Average MLRs in the Medicare Advantage market have been relatively stable over the last few years, averaging 87% in 2021 and 2023 and 86% in 2022. That is somewhat higher than before and during the onset of the COVID-19 pandemic. The slight increase of the MLR in the Medicare Advantage market could imply decreased profitability. It is also possible that some Medicare Advantage insurers opted to offer new or more generous extra benefits, such as over-the-counter allowances, meals following hospital stays, or transportation, in addition to gym memberships, dental, vision and hearing benefits that are offered nearly universally to help retain and attract new enrollees, while also ensuring that those at risk of falling below the required thresholds would have sufficient costs to avoid triggering any rebates to the federal government. At the same time, it may be difficult to interpret changes in MLRs with increasing consolidation, driven in part by insurers purchasing related businesses, such as pharmacy benefit managers, physician groups, and post-acute care providers, because it is not entirely clear how insurers allocate expenses across different lines of business.
Medicare Advantage plans have both higher average costs and higher premiums (largely paid by the federal government), because Medicare covers an older, sicker population. So, while Medicare Advantage insurers spend a similar share of their premiums on benefits as other insurers in other markets, the gross margins described above—which include profits and administrative costs—tend to be higher in Medicare Advantage plans.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
We analyzed insurer-reported financial data from Health Coverage PortalTM, a market database maintained by Mark Farrah Associates, which includes information from the National Association of Insurance Commissioners (NAIC). We used the “Exhibit of Premiums, Enrollment, and Utilization” report (accessed May 28, 2024) for this analysis. The dataset analyzed in this report does not include California HMOs regulated by California’s Department of Managed Health Care. Additionally, for Medicaid, there are five states (Arizona, California, Delaware, New York, and Oregon) that have different reporting practices and therefore consistently only have partial or no NAIC data available.
We excluded plans that were not present in the NAIC demographics file, filed negative values in any of the segments of interest, or have negative or zero dollars in premiums or claims. We also excluded plans reporting at least 1,000 hospital patient days incurred per 1,000 member months. We only included plans that were categorized as having a “medical” focus in our analysis and exclude “specialty” plans which are categorized as “ancillary or supplemental benefit plans.” We also excluded any plans from the U.S. territories. We corrected for plans that did not file “member months” or filed a zero “member month” value in the annual statement but did file current year membership by imputing these values. If, after imputing, plans still did not have “member months,” they were excluded.
The group market in this analysis only includes fully insured plans. NAIC defines “Medicaid” as “business where the reporting entity charges a premium and agrees to cover the full medical costs of Medicaid subscribers.” This explicitly excludes Administrative Services Only (ASO) plans. We only use “medical” focused plans to help exclude any specialty plans; however, prepaid ambulatory health plans (PAHPs), prepaid inpatient health plans (PIHPs), or Programs of All-Inclusive Care for the Elderly (PACE) plans may be included in the analysis due to NAIC’s definition of Medicaid.
Gross margins per enrollee were calculated by subtracting the sum of total incurred claims from the sum of unadjusted health premiums earned and dividing by the total number of members.
Premiums for Medicare Advantage plans primarily consist of federal payments made to plans and any additional amounts plans may choose to charge their enrollees. Premiums for Medicare Advantage plans do not include payments for Medicare Part D benefits. Premiums for Medicaid do not reflect contractual adjustments related to risk corridors or other risk-sharing adjustments.
To calculate medical loss ratios, we divided the market-wide sum of total incurred claims by the sum of all unadjusted health premiums earned. MLRs in this analysis are simple loss ratios and do not adjust for quality improvement expenses, taxes, or risk program payments. It should be noted that other organizations and agencies use claims and premiums reported in the “Statement of Revenues & Expenses” for their medical loss ratio calculations.
Appendix
Individual Market:The individual market, which accounted for about 18 million people in the first quarter of 2023, includes coverage purchased by individuals and families through the Affordable Care Act’s exchanges (Marketplaces) as well as coverage purchased directly off-exchange, which includes both plans complying with the ACA’s rules and non-compliant coverage (e.g., grandfathered policies purchased before the ACA went into effect and some short-term plans). The federal government provides subsidies for low and middle-income people in the Marketplace and includes measures, such as risk adjustment, to help limit the financial liability of insurers. Insurers in the individual market receive premium payments from enrollees, plus any federal subsidies for people in the Marketplaces.
Some plans submitting data on the Exhibit of Premiums Enrollment and Utilization appear to be including some Children’s Health Insurance Program (CHIP) data in their Individual market filings. In a previous version of this analysis, we used the Supplemental Health Care Exhibit to address this. However, in this analysis, we opted to use the EPEU to ensure comparability.
Group Market:The fully insured group market serves employers, their employees and dependents who are enrolled in fully insured health plans. This market includes both small and large group plans but excludes employer-sponsored insurance plans that are self-funded, which account for 65% of workers with employer-sponsored insurance in 2023. Roughly 30 million people were enrolled in fully insured group market plans in 2023. Plans typically receive premium payments from both employers and their employees.
Medicaid Managed Care:The Medicaid managed care market includes managed care organizations (MCOs) that contract with state Medicaid programs to deliver comprehensive acute care (i.e., most physician and hospital services) to enrollees. As of July 2021, about three-fourths (just over 66 million people) of all Medicaid beneficiaries nationally received most or all of their care from comprehensive risk-based MCOs. There is significant variation across states with respect to services that are covered by MCOs.
In this analysis, the NAIC data we use defines “Medicaid” as “business where the reporting entity charges a premium and agrees to cover the full medical costs of Medicaid subscribers” and only explicitly excludes Administrative Services Only (ASO) plans from their reporting. While we only use “medically” focused plans to help exclude any specialty plans, PAHPs, PIHPs and PACE plans may not be excluded due to NAIC’s definition of Medicaid. Additionally, for Medicaid, there are five states (Arizona, California, Delaware, New York, and Oregon) that have different reporting practices and therefore consistently only have partial or no NAIC data available. In other work, KFF defines comprehensive MCOs as managed care plans that provide comprehensive Medicaid acute care services and, in some cases, long-term services and supports as well. This excludes “limited benefit plans” including prepaid ambulatory health plans (PAHPs), prepaid inpatient health plans (PIHPs), and Programs of All-Inclusive Care for the Elderly (PACE) that may be included in this analysis.
Mark Farrah Associates Health Coverage PortalTM includes data from fully capitated risk-based MCOs as well as non-comprehensive Primary Care Case Management (PCCM) plans and some specialty plans. PCCM plans have lower capitated payments than comprehensive MCO agreements because a primary care physician is paid a smaller flat fee for case management and care coordination responsibilities, but the remainder of services an enrollee receives are delivered on a Fee-For-Service agreement.
Medicare Advantage:The Medicare Advantage market provides Medicare-covered benefits through private plans to more than 30 million Medicare beneficiaries in 2023, which is just over half of all Medicare beneficiaries in 2023. The federal government makes risk-adjusted payments (higher payments for sicker enrollees and lower payments for healthier enrollees) to plans (averaging nearly $14,380 per enrollee in 2023) to cover the cost of benefits covered under Medicare Parts A and B and supplemental benefits, such as dental, vision, hearing, and others, with additional payments for costs associated with prescription drug coverage. Some plans charge enrollees an additional premium.