Immigrants Have Lower Health Care Expenditures Than Their U.S.-Born Counterparts
Introduction
As of 2022, there were 45.5 million immigrants residing in the U.S., including 21.2 noncitizen immigrants and 24.2 million naturalized citizens, who together account for about 15% of the total population.1 While there has been increasing focus among some policymakers on the health care expenses incurred by immigrants, research suggests that they not only have lower health care costs than U.S.-born people but also help subsidize health care for U.S.-born people by paying more into the system through health insurance premiums and taxes than they utilize. This data note provides further insight into health care expenditures for immigrants by analyzing their average per capita health care expenditures and comparing them to expenditures for U.S.-born people overall and by health care services and payment sources using data from the 2021 Medical Expenditures Panel Survey.
This analysis finds that, on average, annual per capita health care expenditures for immigrants, including naturalized citizens and noncitizens, are about two-thirds of those for U.S.-born citizens overall ($4,875 vs. $7,277). This reflects lower spending for most types of health care, including office-based visits, prescription drugs, inpatient care, outpatient care, and dental care. Among average per capita expenditures, the relative amount paid by most payment sources is lower for immigrants compared to U.S.-born people, including private coverage, Medicare, and out-of-pocket spending. There is no significant difference in average emergency room and Medicaid expenditures between U.S.-born citizens and immigrants.
These patterns suggest that immigrants use less health care than U.S.-born people and often rely on the emergency room when they do seek care. Lower use of health care among immigrants likely reflects a combination of them being younger and healthier than their U.S.-born counterparts as well as them facing increased barriers to care, including lower rates of coverage due to more limited access to private coverage and Medicaid eligibility restrictions for immigrants. In general, lawfully present immigrants must have a “qualified” immigration status to be eligible for Medicaid or the Children’s Health Insurance Program (CHIP), and many must wait five years after obtaining qualified status before they may enroll. Undocumented immigrants are not eligible to enroll. Immigrants also face language access challenges and confusion and fears. Increasing coverage and reducing other barriers to care for immigrants could increase the use of preventive and primary care, which could prevent the worsening of conditions and reliance on emergency room care.
Findings
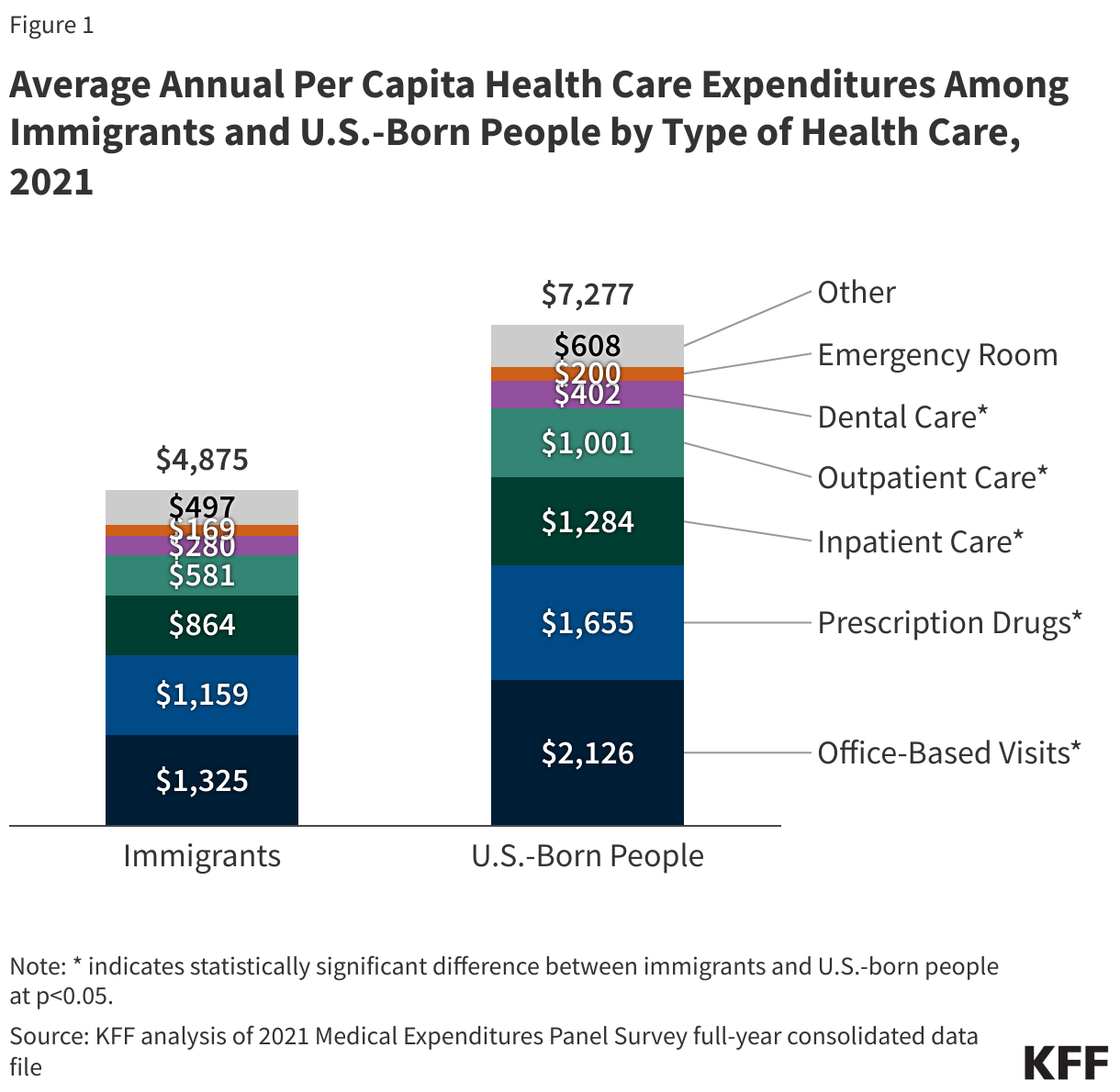
In 2021, annual average overall per capita health care expenditures for immigrants were $4,875 compared to $7,277 for U.S.-born citizens. Annual average per capita spending for immigrants was lower than for U.S.-born citizens on office-based visits ($1,325 vs. $2,126), prescription drugs ($1,159 vs. $1,655) inpatient care ($864 vs. $1,284), outpatient care ($581 vs. $1,001), and dental care ($280 vs. $402) (Figure 1). Average per capita spending on emergency room care was not statistically significantly different between immigrants ($169) and U.S.-born citizens ($200).
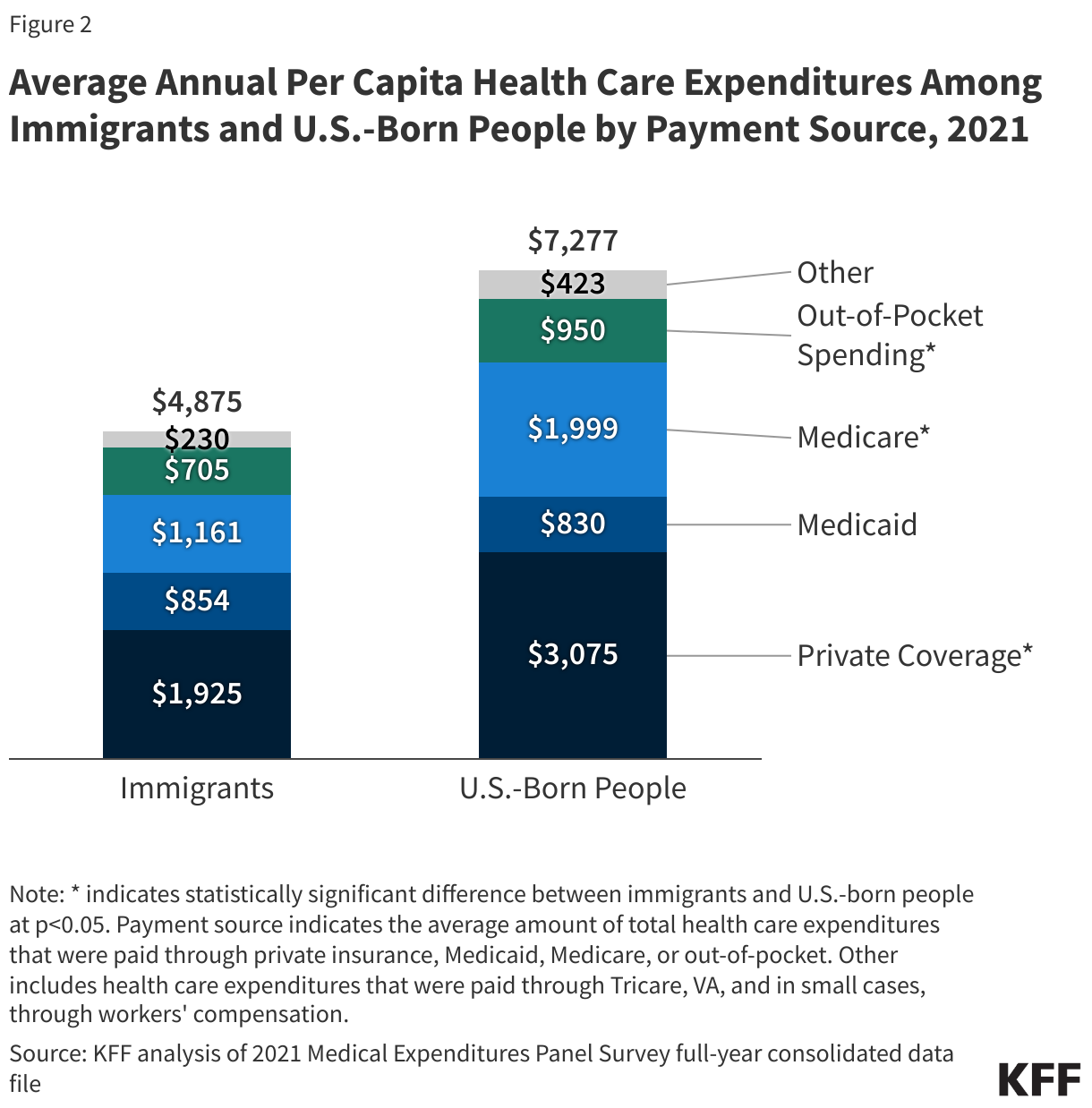
Among average annual total per capita expenditures, the relative amount paid for by private coverage ($1,925 vs. $3,075), Medicare ($1,161 vs. $1,999), and out-of-pocket spending ($705 vs. $950) was lower for immigrants compared to U.S.-born people (Figure 2). There was no statistically significant difference in the average amount paid by Medicaid for immigrants ($854) and U.S.-born people ($830). Medicaid eligibility is limited for immigrants. In general, lawfully present immigrants must have a “qualified” immigration status to be eligible for Medicaid or CHIP, and many must wait five years after obtaining qualified status before they may enroll. For children and pregnant people, states can eliminate the five-year wait and extend coverage to lawfully present immigrants without a qualified status. States can also extend pregnancy-related coverage to immigrants regardless of status through the CHIP From-Conception-to-End-of-Pregnancy option. Undocumented immigrants are not eligible to enroll in Medicaid. Medicaid payments for emergency services may be made for individuals who are otherwise eligible except for immigration status to help cover the costs incurred for providing this care. Given these limits, it is likely that a greater share of Medicaid spending for immigrants goes toward pregnancy-related care and emergency care, which tend to be costly. In contrast, U.S.-born enrollees include a high share of children, who typically utilize lower-cost preventive and primary care, resulting in lower spending.
Methods |
| The data in this brief are based on KFF analysis of the 2021 Medical Expenditures Panel Survey (MEPS) full-year consolidated data file. The data presented in this brief include the average annual per capita health care expenditures for immigrants (individuals born outside the U.S. or its territories) and U.S.-born citizens both overall and for major types of health care including office-based visits, prescription drugs, inpatient care (including facility and doctor charges), outpatient care (including facility and doctor charges), dental care, and emergency room care (including facility and doctor charges). Health care expenditures are also examined by payment source, that is, the amount of total average per capita expenditures that are paid through private coverage, Medicare, Medicaid, and out-of-pocket spending. A limitation of federal surveys, including MEPS, is the likely underrepresentation of immigrants, particularly recent and undocumented immigrants, and potential undercounting of emergency Medicaid spending. |
Endnotes
KFF analysis of 2022 American Community Survey 1-year Public Use Microdata Sample