From Ballot Initiative to Waivers: What is the Status of Medicaid Expansion in Utah?
Since Utah voters approved a November 2018 ballot measure to adopt the Affordable Care Act (ACA) Medicaid expansion up to 138% of the federal poverty level (FPL), the state legislature has taken steps to roll back the full expansion. The state enacted a law in February 2019 that amended the voter-approved ballot measure, requiring the state to submit a series of Section 1115 waiver requests. This brief provides additional detail about the ballot measure, the state legislation, the status of the required waiver submissions, and the broader implications of Utah’s waivers for other states.
- Bridge Plan. The first waiver, the “Bridge Plan,” was approved in March 2019, and allowed the state to implement a coverage expansion to 100% FPL beginning April 1, 2019, at the state’s regular matching rate. The approved waiver also included an enrollment cap and a work requirement.
- Per Capita Cap. On July 31, 2019, Utah submitted to the Centers for Medicare and Medicaid Services (CMS) its “Per Capita Cap” proposal for a new waiver that would continue a number of provisions already approved as well as a request for the enhanced match for partial expansion to 100% FPL and a limit on enhanced federal funding. CMS issued a general statement in late July and a letter to the state in mid-August confirming that they would not approve the enhanced matching rate for an expansion that does not go to 138% FPL or that includes an enrollment cap.1 Given CMS guidance about partial expansion, it seems clear that some provisions of the Per Capita Cap waiver will not be approved, but CMS says it is reviewing the other provisions.
- Fallback Plan. The state legislation requires the submission of a “Fallback Plan” waiver should CMS not approve the Per Capita Cap waiver. On November 4, 2019, Utah submitted to CMS its Fallback Plan waiver that would expand Medicaid to 138% FPL and would continue some other provisions in the earlier waivers, including an enrollment cap. In its submission letter, Utah says that CMS rejected its PCC waiver request, although the waiver is still listed as pending on CMS’ website as of November 14, 2019.
- Ballot Approved Expansion. If CMS does not approve the Fallback Plan by July 1, 2020, Utah must adopt the full Medicaid expansion without restrictions as required by the ballot initiative.
Utah Ballot Initiative and Subsequent Legislation
As in Idaho and Nebraska, Utah voters supported a November 2018 ballot measure to adopt the full Medicaid expansion as set out in the ACA. Utah voters approved a full ACA expansion to cover nearly all adults with income up to 138% of the federal poverty level (FPL, $17,236/year for an individual in 2019), an April 1, 2019, implementation date, and a state sales tax increase as the funding mechanism for the state’s share of expansion costs. By implementing a full ACA expansion, Utah would qualify for the substantially enhanced (93% in 2019 and 90% in 2020 and thereafter) federal matching funds. The expansion population in Utah includes childless adults ages 19-64 with income from 0% to 138% FPL and parent/caretakers ages 19-64 with income from 60% to 138% FPL.2 The fiscal note from the ballot initiative estimated that approximately 150,000 newly eligible individuals would enroll in Medicaid in fiscal year 2020.
However, the Utah legislature significantly changed and limited the coverage expansion that the voters adopted. Utah is one of 11 states (out of the 21 states that allow state laws to be adopted via a ballot initiative) that have no restrictions on how soon or with what majority state legislators can repeal or amend voter-initiated statutes. Utah Governor Gary Herbert signed Senate Bill 96 into law on February 11, 2019. The state released an implementation toolkit that follows the legislation in calling for multiple steps to implement an expansion of Medicaid coverage to adults in ways that differ from a full ACA expansion (Figure 1).
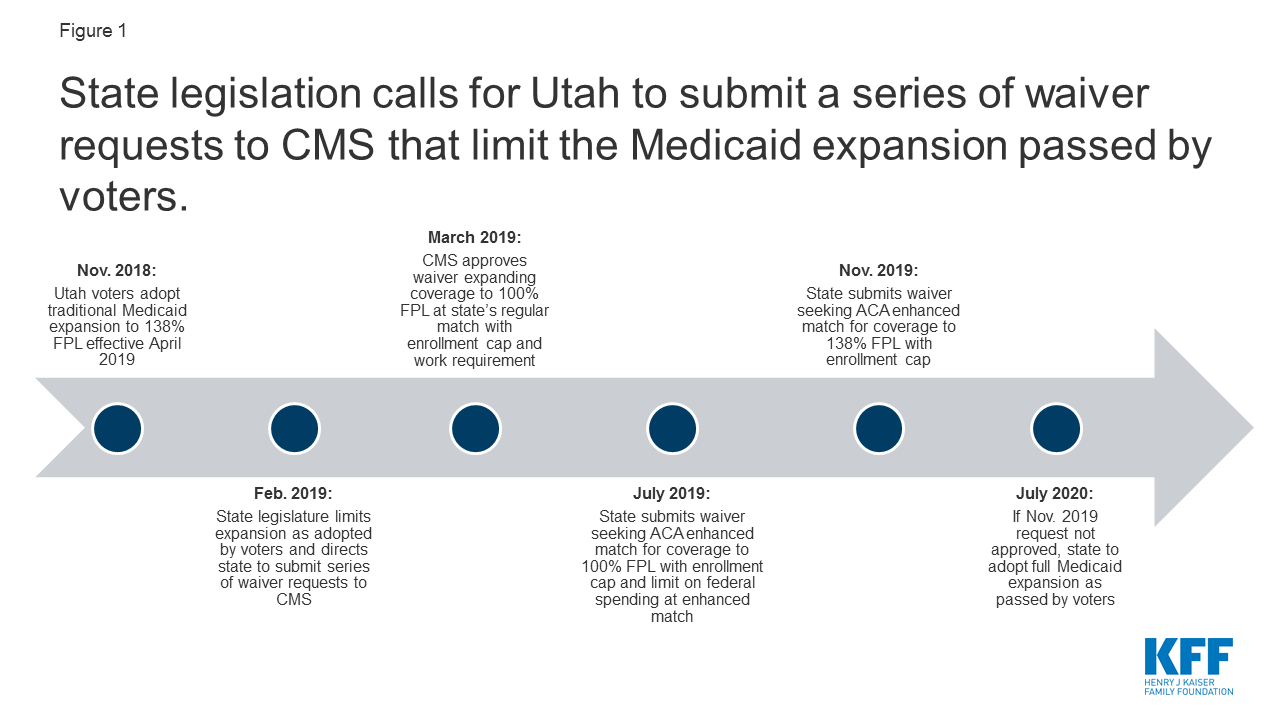
Figure 1: State legislation calls for Utah to submit a series of waiver requests to CMS that limit the Medicaid expansion passed by voters.
Utah’s Amended Waiver Approved March 2019
On March 29, 2019, CMS approved an amendment to Utah’s existing Section 1115 demonstration waiver to expand Medicaid to a capped number of adults with income up to 100% FPL beginning on April 1, 2019, at the state’s regular Medicaid matching rate, not the enhanced ACA matching rate.3 The authority to cover this “Adult Expansion Population” expires on January 1, 2021. The Adult Expansion Population under the waiver includes childless adults ages 19-64 with income from 0 to 100% FPL4 and parent/caretakers ages 19-64 with income from 60% FPL to 100% FPL,5 a more limited coverage expansion than the 138% FPL approved by the voters (Figure 2). The state estimates that approximately 70,000 to 90,000 people will be covered under the waiver with financial eligibility limited to 100% FPL, about 40,000 fewer compared to a full ACA expansion to 138% FPL.6
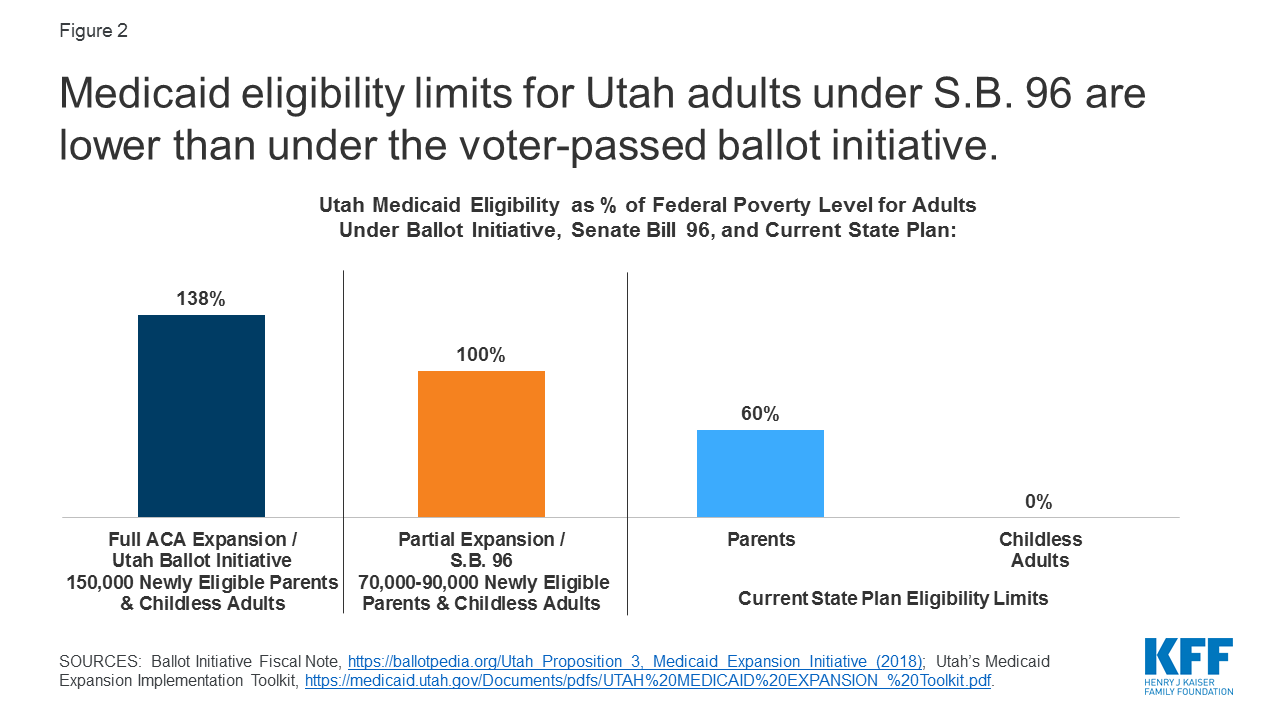
Figure 2: Medicaid eligibility limits for Utah adults under S.B. 96 are lower than under the voter-passed ballot initiative.
Instead of the 90% enhanced federal matching rate tied to newly eligible adults under a full ACA expansion, Utah is receiving its current, traditional federal matching rate of 68%. This lower matching rate will result in higher state costs for expanding coverage to 100% FPL than for a full expansion to 138% FPL (Figure 3).7 Utah refers to the March 2019 waiver amendment as the “Bridge Plan” because the state is seeking further waiver amendments as required by Senate Bill 96 and described in the text below. Utah’s pre-ACA coverage expansion, authorized by its waiver prior to the Bridge Plan amendment, provided limited benefits and preventive care (see Box 1 below).
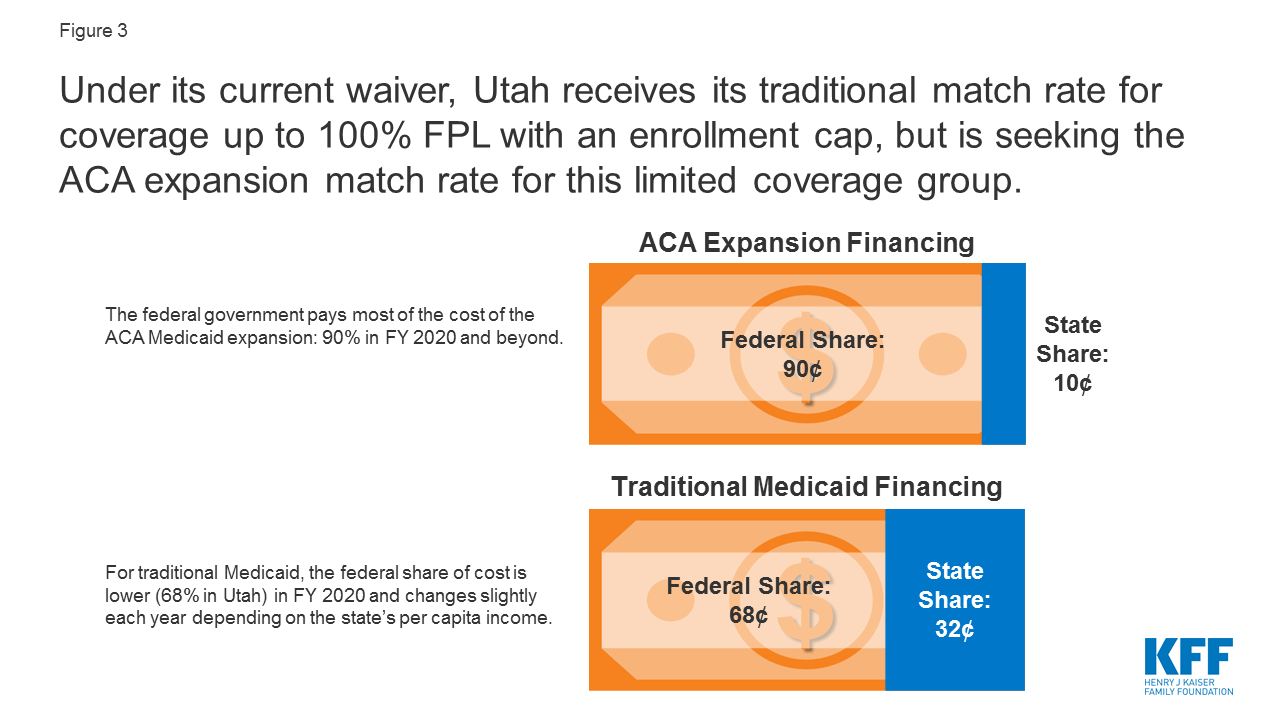
Figure 3: Under its current waiver, Utah receives its traditional match rate for coverage up to 100% FPL with an enrollment cap, but is seeking the ACA expansion match rate for this limited coverage group.
Utah’s amended waiver includes an enrollment cap to be imposed at state option on the Adult Expansion Population, meaning that not all eligible people may be able to enroll in coverage. The waiver allows the state to close enrollment for the Adult Expansion Population, which could limit enrollment further than the coverage estimates noted above. The waiver does not specify a pre-determined maximum number of people to be covered but instead allows the state to stop enrolling eligible people “if projected costs exceed state appropriations.” If the enrollment cap is reached, the state will not maintain a waiting list; instead, eligible individuals will have their applications denied and will have to reapply for coverage when enrollment re-opens. Consequently, individuals who apply at the beginning of a state fiscal year could be more likely to gain coverage than those who apply later in the fiscal year, even though they are otherwise eligible, if the state imposes the enrollment cap. It is possible that individuals with lower incomes or higher needs, compared to those already enrolled, might be barred from enrolling in coverage as a result of the timing of their application due to the enrollment cap.
Utah’s amended waiver also includes a work requirement as a condition of eligibility for the Adult Expansion Population, beginning no sooner than January 1, 2020.8 In Utah, individuals subject to the work requirement must complete certain activities within the first three months of each 12-month eligibility period or qualify for an exemption. Possible exemptions include age of 60 or older, pregnancy, responsibility to care for a dependent under age six in the same household or a disabled person, and physical or mental inability to meet the work requirement as determined by a medical professional, among others. Those who fail to do so will lose coverage for the rest of the year or until they fulfill the requirement. Qualifying activities include registering for work through the state’s online system, completing an online employment training needs assessment, completing online job training modules identified through the assessment, and applying for work with at least 48 potential employers.
Utah’s Per Capita Cap Waiver Submitted July 2019
In accordance with SB 96, Utah submitted its “Per Capita Cap” (PCC) waiver application to CMS on July 31, 2019, which includes a request to receive the 90/10 ACA enhanced matching rate for expansion adult coverage up to 100% FPL; however, CMS guidance states that such a policy would not be approved.9 The waiver would move all expansion adults (parents 60-100% and childless 0-100%, including the Targeted Adult group) and the waiver services provided to these populations from the existing waiver to the new waiver. The Targeted Adult population includes adults ages 19-64 without dependent children with income up to 5% FPL who are chronically homeless or involved in the criminal justice system and in need of substance use or mental health treatment.
Days before Utah’s submission, a CMS statement indicated that it would not approve the 90/10 ACA enhanced matching rate for an expansion population smaller than the full group up to 138% FPL, arguing that such policies would “invite continued reliance on a broken and unsustainable Obamacare system.”10 Therefore, the result of no partial expansion is similar to the prior administration, but for different publicly-stated reasons.11 In its submission letter, the state provided several reasons for submitting the waiver as envisioned in SB 96, including the unknown outcome of the Texas vs U.S. litigation challenging the ACA, value in getting a formal response from CMS, and the state’s hopes for approval of other waiver provisions. CMS also indicated in an August 16, 2019 letter12 to Utah that it would not authorize an enrollment cap with enhanced ACA matching funds for the expansion group as Utah requested; see more on this guidance in the Fallback Plan section below.
The waiver also requests a limit on enhanced federal funding through what the state describes as a “per capita cap” funding mechanism. Under the waiver request, an aggregate annual per capita cap would be calculated based on the weighted total of separate per capita caps for three enrollment groups: targeted adults and enrollees receiving IMD services for substance use disorder (SUD), expansion parents, and expansion adults without children.13 Expenditures in excess of the total per capita cap but within budget neutrality would receive the State’s traditional FMAP rather than the enhanced matching rate.14 The state would establish per enrollee amounts for each group for a base year and apply a trend rate for future demonstration years.
Unlike federal legislative per capita cap proposals, the PCC waiver request would not impose a cap on all federal Medicaid dollars. The state request would apply only to the enhanced matching dollars and not all federal matching dollars, include a mechanism for automatic rebasing, and allow for adjustments for unforeseen events like a public health emergency, natural disaster, major economic event, new federal mandate, or any subsequent waivers approved by CMS that affect the populations under this waiver. The state assumes a “with waiver” per capita cap growth rate of 4.2%, lower than the anticipated “without waiver” per member per month cost growth rate of 5.3%.
Among other provisions, the PCC waiver proposal also includes a lockout period for “Intentional Program Violations” (IPV) committed when documenting Medicaid eligibility. The state seeks waiver authority to impose a six-month coverage lockout period if an individual commits an IPV. Utah defines an IPV as occurring when there is “clear and convincing evidence that the individual knowingly, willingly, or recklessly provided false or misleading information with an intent to receive benefits to which he or she was not eligible to receive” and may find the individual responsible to repay any medical assistance received for which he or she was not eligible. An IPV would include not reporting a change in eligibility within ten days with the intent to obtain benefits to which the enrollee is not entitled. Under Utah’s existing Medicaid policy, the state is currently determining IPVs using this definition and assessing overpayments using an administrative hearing process. The new authority that the PCC waiver seeks is to impose coverage lockouts when an IPV determination is made. Utah also has a separate process where certain cases are referred for potential criminal fraud prosecution in court.
The waiver request includes other eligibility, benefit, and process changes. The PCC waiver’s other new provisions include expenditure authority for housing-related services and supports and authority to provide up to 12-month continuous Medicaid eligibility. The state asks for waiver authority to limit these provisions to certain geographic areas or populations that are not specified in the waiver. The waiver also seeks authority to not allow hospitals to make presumptive eligibility determinations and to allow the state to continue a limited benefit package for expansion parents. Finally, the waiver seeks to waive some managed care rules, including advance CMS approval of actuarially sound rates, managed care contracts, and directed payments.
In addition to the new provisions, the PCC waiver seeks to maintain authority to implement provisions approved in March 2019, including the enrollment cap (currently approved at the regular federal matching rate) and the work requirement for the expansion population. As noted above, CMS has indicated that it would not approve the enhanced federal matching rate for the ACA expansion in the context of enrollment caps. Based on its experience with SNAP work requirements, the state estimates that approximately 70 percent of expansion adults (49,000-63,000 individuals) will meet an exemption to the work requirements. The state further projects that, among individuals who do not meet an exemption or good cause reason, approximately 75-80 percent will comply with the work requirements. Other provisions that were approved in March 2019 include dental benefits for Targeted Adults receiving SUD treatment, SUD treatment in institutions for mental disease (IMD), a targeted SUD residential withdrawal pilot in Salt Lake County, and a waiver of EPSDT for 19- and 20-year-olds.
Utah’s Fallback Plan Waiver Submitted November 2019
As directed by SB 96, Utah submitted its Fallback Plan waiver request on November 4, 2019, seeking authority for a coverage expansion up to 138% FPL with the 90/10 ACA enhanced matching funds and an enrollment cap.15 In its submission letter, Utah says that CMS rejected its PCC waiver request, although the waiver is still listed as pending on CMS’ website as of November 14, 2019. Like the PCC waiver, the Fallback Plan includes coverage lockouts for intentional program violations, elimination of hospital presumptive eligibility, expenditure authority for housing-related services and supports, and modifications for managed care rules; unlike the PCC waiver, it does not request the authority to provide 12-month continuous Medicaid eligibility for the expansion population. The Fallback Plan seeks to continue the work requirement and enrollment cap approved in March 2019 but does not seek a per capita cap on federal funds at the enhanced matching rate.
As noted above, CMS has indicated that it would not authorize an enrollment cap with enhanced ACA matching funds for the expansion group, as Utah requested in both the PCC and Fallback waivers. In addition to expanding coverage to 138% FPL and receiving the 90/10 ACA enhanced match rate, the Fallback Plan requests to continue the enrollment cap approved by CMS in March 2019. In an August 16, 2019, letter16 to Utah following the state’s PCC waiver submission, CMS noted that, if implemented, an enrollment cap would “have the effect of limiting enrollment to less than the full group otherwise eligible for Medicaid, which would be tantamount to ‘partial expansion.’” CMS noted that it would therefore not authorize the enhanced matching rate if the enrollment caps were implemented. In its submission letter, Utah provided two reasons for submitting the Fallback Plan waiver as envisioned in SB 96 despite this CMS guidance: the unknown outcome of the Texas vs U.S. litigation challenging the ACA and the state’s hopes for approval of other waiver provisions. As explained in Box 1, enrollment caps are no longer necessary to ensure federal budget neutrality because the ACA now allows states to access federal Medicaid funds for this coverage directly through the creation of the new adult eligibility pathway and the availability of federal matching funds.
Box 1: Coverage Expansion under Utah’s Waiver Prior to the ACA
In 2014, the ACA for the first time authorized federal Medicaid matching funds for coverage for nearly all nonelderly adults. Prior to 2014, federal Medicaid funds could only be used to cover pregnant women, parent/caretakers, children, seniors, and people with disabilities. Adults without dependent children were ineligible for Medicaid, no matter how poor they were. Before the ACA, some states used Section 1115 waivers to establish coverage expansions beyond the limits of federal law. Because federal Medicaid funds could not be accessed directly to cover these adults, these waivers included provisions to generate savings to fund coverage expansions, such as limited benefit packages, premiums, and/or mandatory managed care enrollment, and sometimes enrollment caps as a way to limit federal spending and ensure federal budget neutrality.17 However, budget neutrality is no longer a consideration for such coverage expansions under waivers now that federal Medicaid law, as amended by the ACA, includes an eligibility pathway and allows states to receive federal Medicaid matching funds to cover nearly all nonelderly adults, including those without dependent children, up to 138% FPL without the need for a waiver.
Utah’s existing Section 1115 waiver was first approved in 2002 and included a pre-ACA coverage expansion (called the Primary Care Network, PCN) to parents with income above the state plan limit (60% FPL) and childless adults (for whom no state plan coverage was available). As of March 2019, the PCN income limit was 100% FPL. The PCN coverage expansion provided a limited benefit package of primary and preventive services18 to a capped number of these adults and was funded by reduced benefits for traditional low-income (categorically and medically needy) parents. The March 2019 waiver amendment suspends authority for Utah’s pre-ACA PCN coverage expansion and moves the 17,500 parents and childless adults in the PCN group as of March 2019 to the new “Adult Expansion Population” (described in the section above on Utah’s Amended Waiver Approved Mach 2019) effective April 1, 2019.19
The Fallback Plan waiver requests to expand the eligibility criteria for the Targeted Adult group and seeks authority to suspend enrollment for sub-populations of Targeted Adult populations. The Targeted Adult group is comprised of three populations and Utah currently has authority to suspend enrollment for the entire Targeted Adult group or separately for any of the three populations. In the Fallback Waiver, Utah seeks to expand the Targeted Adult Medicaid criteria to include three new sub-populations: homeless victims of domestic violence, individuals who are court ordered to receive substance abuse or mental health treatment, and individuals on probation or parole with serious mental illness and/or serious substance use disorder. Utah estimates that an additional 7000 individuals will be eligible for the Targeted Adult group due to the expanded criteria. Any suspension of enrollment of Targeted Adult populations or sub-populations would occur through the state’s administrative rule-making process. If enrollment is suspended for Targeted Adults, individuals could be eligible in the Expansion Adult group (provided that enrollment has not been suspended there); however, unlike the Expansion Adult group, Targeted Adults receive 12-month continuous eligibility and dental benefits (if receiving substance use disorder treatment services).
Under the Fallback Plan waiver, adults with incomes between 100% and 138% of the FPL would pay monthly premiums in order to maintain coverage under Medicaid expansion. Monthly premiums would be $20 for a single individual or $30 for a married couple. Utah requests the authority to raise these premiums to reflect annual increases in the FPL through the state administrative rulemaking process. Beneficiaries who fail to pay their premium in the month prior to the month of eligibility would be dis-enrolled from Medicaid and required to pay all past-due premiums to re-enroll, unless it had been more than six months from when coverage ended. Members of federally recognized tribes and those identified as medically frail would be exempt from paying premiums. The state estimates that 40,000 individuals would be required to pay these monthly premiums and that approximately 3% of these beneficiaries would lose eligibility due to failure to pay.
The Fallback Plan waiver would also add a premium surcharge for non-emergent use of the emergency department. The state seeks to require beneficiaries with incomes between 100% and 138% of the FPL to pay a $10 premium surcharge for any use of the emergency department considered non-emergent, up to a maximum of $30 per quarter. Individuals would receive one warning after the first occurrence of non-emergent emergency department use, and any subsequent non-emergent uses would result in the $10 surcharge to their monthly premium. An individual with five or more occurrences of non-emergent use within the most recent twelve months would be referred to the Medicaid Restriction Program, which could take additional action such as limitations on where the individual may receive services. Members of federally recognized tribes, individuals receiving employer-sponsored insurance reimbursement, and medically frail individuals would be exempt from this provision. The state estimates that between 1500 and 2000 beneficiaries would owe surcharges each month.
In addition to these provisions, the Fallback Plan waiver also seeks authority to make additional changes to the Medicaid expansion through the state administrative rulemaking process without requiring CMS approval. Utah expects that most of these changes, if enacted, would decrease total beneficiary months and demonstration expenditures. The changes include:
- Making enrollment begin on the first of the month after application for beneficiaries with incomes above 100% FPL.
- Eliminating retroactive eligibility for beneficiaries with incomes above 100% FPL.
- Changing the benefit package for expansion beneficiaries and Targeted Adult groups to the state’s non-traditional package. This would restrict all Medicaid beneficiaries to this more limited plan except for those identified as medically frail.
- Exempting certain income groups from the employer-sponsored insurance requirement.
- Suspending housing supports.
- Making enrollment in managed care mandatory or optional for different groups of expansion adults.
- Opening or suspending enrollment for each population group within the Target Adult population.
What is Next?
The Fallback Plan waiver is currently under consideration at CMS. Given CMS guidance about partial expansion, it seems clear that the request for enhanced ACA matching funds with an enrollment cap on the expansion group will not be approved, but CMS says it is reviewing the other requests. In its submission letter, Utah requested that CMS approve the Fallback Plan waiver by December 31, 2019, for implementation on January 1, 2020.
If CMS does not approve the Fallback Plan by July 1, 2020, Utah will adopt the full Medicaid expansion plan with no restrictions as set out by the ACA and approved in the ballot initiative. This plan would include coverage of all eligible adults up to 138% FPL at the ACA enhanced matching rate and would use a state plan amendment instead of waiver authority. It would not include a work requirement, enrollment cap, or other eligibility and enrollment restrictions as proposed in the waiver proposals described above.20