Potential Impacts of New Requirements in Florida and Texas for Hospitals to Request Patient Immigration Status
Recent actions in Florida and Texas newly require hospitals to request immigration status from patients, with the aim of assessing the cost of providing care to undocumented immigrants. In May 2023, Florida Governor Ron DeSantis signed Senate Bill (SB) 1718 into law, which, among other actions, requires hospitals that receive Medicaid or Children’s Health Insurance Program (CHIP) funding to collect information on patient immigration status. In August 2024, Texas Governor Greg Abbott issued an executive order that similarly requires hospitals receiving Medicaid or CHIP funding to collect information on patient immigration status effective November 1, 2024. While these actions require hospitals to request this information, they must also inform patients that, as required by federal law, their response will not affect their care. In Florida, the hospitals must also indicate that the response will not result in a report to immigration authorities. This requirement is not specified in the Texas Executive Order. Under federal law, hospitals are required to provide emergency screening and stabilization services to all patients seeking emergency care. This brief examines the potential implications of these requirements for immigrant families and the states’ workforces and economies.
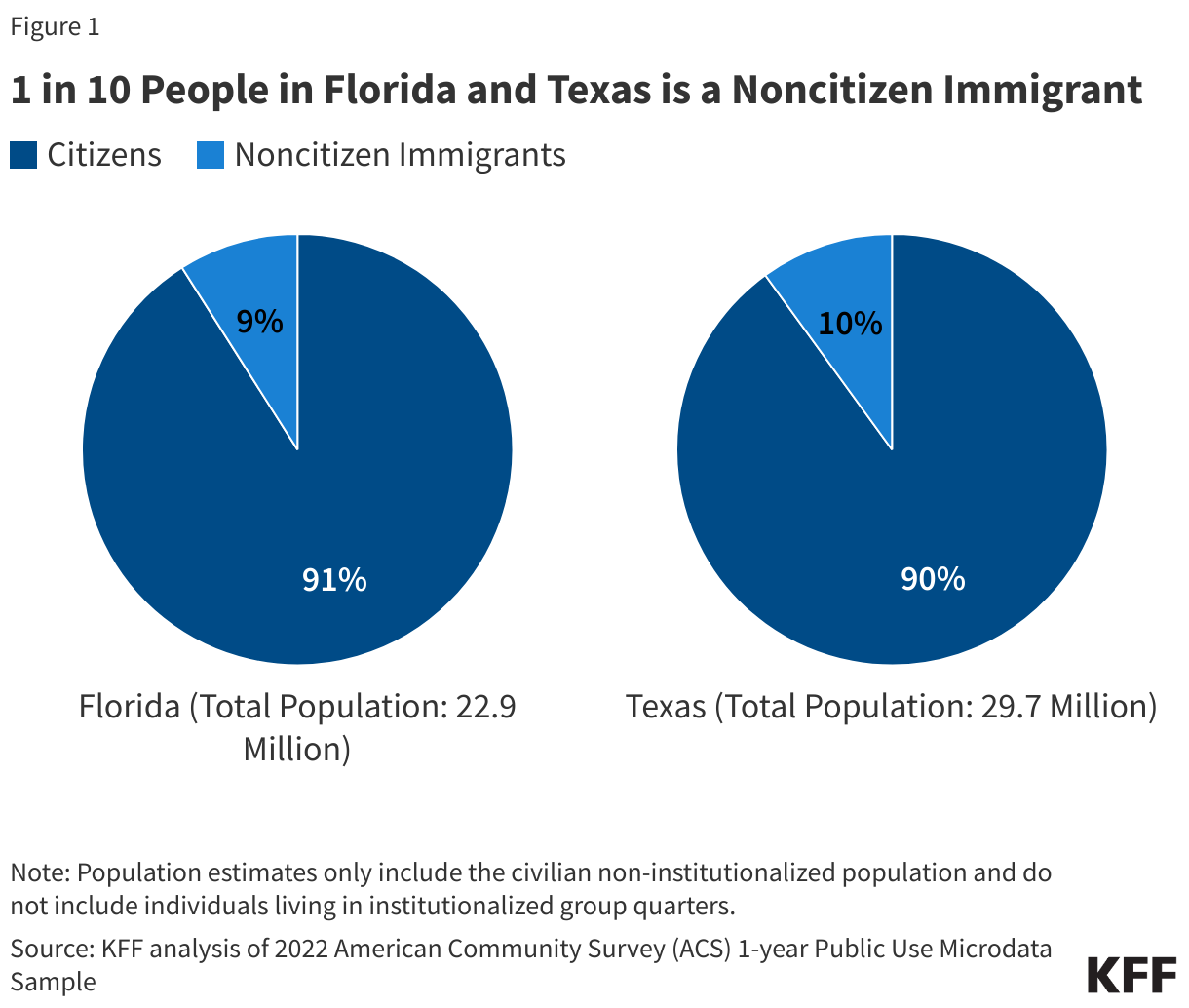
Noncitizen immigrants, including lawfully present and undocumented immigrants, make up about one in ten of residents in Florida and Texas, but larger shares of residents, including many U.S.-born citizen children, live in immigrant families. As of 2022, there were roughly 2 million noncitizen immigrants in Florida, including both lawfully present and undocumented immigrants, who make up 9% of the state’s population, and Texas had about 2.8 million noncitizen immigrants, who make up one in ten of the state’s population (Figure 1). A larger number of residents in both states live in immigrant families, which often include people of mixed immigration statuses, including U.S.-born citizen children. In Florida, 17% or over 740,000 children have at least one noncitizen parent, and in Texas over one in five (22%) or about 1.7 million children are in a family with a noncitizen parent.
Overall, KFF and other research shows that despite having a higher uninsured rate, noncitizen immigrants, particularly those who are undocumented, use less health care and have lower health care spending than those born in the U.S. Undocumented immigrants are less likely than citizens to report using health care, including emergency care. Further, immigrants, including undocumented immigrants, have lower per capita health care expenditures than U.S.-born citizens, and data suggest they subsidize health care for U.S.-born citizens by paying more into the system through health insurance premiums and taxes than they utilize. Lower use of health care among immigrants likely reflects a combination of them being younger and healthier than their U.S.-born counterparts as well as them facing increased barriers to care, including lower rates of coverage due to more limited access to private coverage and Medicaid eligibility restrictions for immigrants. Undocumented immigrants are not eligible to enroll in Medicaid or other federally funded health coverage. Medicaid payments for emergency services may be made directly to hospitals for individuals who are otherwise eligible except for immigration status to help cover the costs incurred for providing this care. Federal funds may not be used to provide Medicaid coverage to undocumented immigrants, though some states have used their own funds to provide such coverage.
Initial data from Florida suggest that less than 1% of hospital emergency room visits and admissions were among undocumented immigrants. Florida released a public dashboard and a separate report submitted to the state legislature based on hospital reporting under the new requirement for June through December 2023. These reports show that less than 1% of inpatient admissions and emergency department visits were among patients who identified themselves as not lawfully present. The 7% to 8% of patients who declined to provide responses may include additional undocumented immigrants. The state extrapolates an estimate that the cost of care provided to undocumented immigrants over this period was $556 million. However, as noted by the state in the legislative report and others, it is unclear how much of that care was uncompensated. Costs of care for undocumented immigrants may be covered via self-pay, private coverage, or, in some cases, Emergency Medicaid (if it is emergency care provided to an individual who would otherwise be eligible except for immigration status). The legislative report further specifies that the state did not identify any correlation between the level of uncompensated care and the level of undocumented immigrants presenting at the hospital, and that high levels of uncompensated care were more associated with rural county status than the share of undocumented immigrant patients. There also did not appear to be a correlation between total profitability and the share of undocumented immigrants.
These new requirements, along with other recent restrictive immigration policies in these states, will likely contribute to increased fears among immigrant families, which may negatively impact their daily lives, physical health, and mental well-being. These new hospital requirements sit against a backdrop of other recent restrictive immigration policies enacted by these states. For example, the Florida law also creates penalties for hiring undocumented immigrants, expands employment verification screening requirements, invalidates out-of-state drivers’ licenses for undocumented immigrants, establishes criminal penalties for transporting undocumented immigrants into the state, increases funding to relocate or bus migrants to other parts of the U.S., and expands state authority to carry out immigration enforcement. Texas passed legislation in November 2023 that enables state and local law enforcement agencies to question and arrest any individual they believe to be an undocumented immigrant at ports of entry, although its implementation is currently on hold due to legal challenges. These types of new restrictions, along with the new hospital requirements, will likely increase fears among immigrant families, which may may make them more reluctant to access health care for themselves and their children. Prior KFF analysis of Trump-era restrictive immigration policies found that such fears and impacts extend beyond undocumented immigrants to those who are lawfully present and children in immigrant families, who often are U.S-born citizens. One news report suggests that Florida’s Emergency Medicaid expenditures fell after implementation of the requirements, which may reflect decreased use of care among undocumented immigrants and could have negative health consequences given that this funding goes toward emergent care, including care for labor and delivery. It is also possible that some undocumented immigrants have migrated out of the state. Given these types of concerns, the American Medical Association suggests avoiding explicit documentation of immigration status of patients and their family members in a health record.
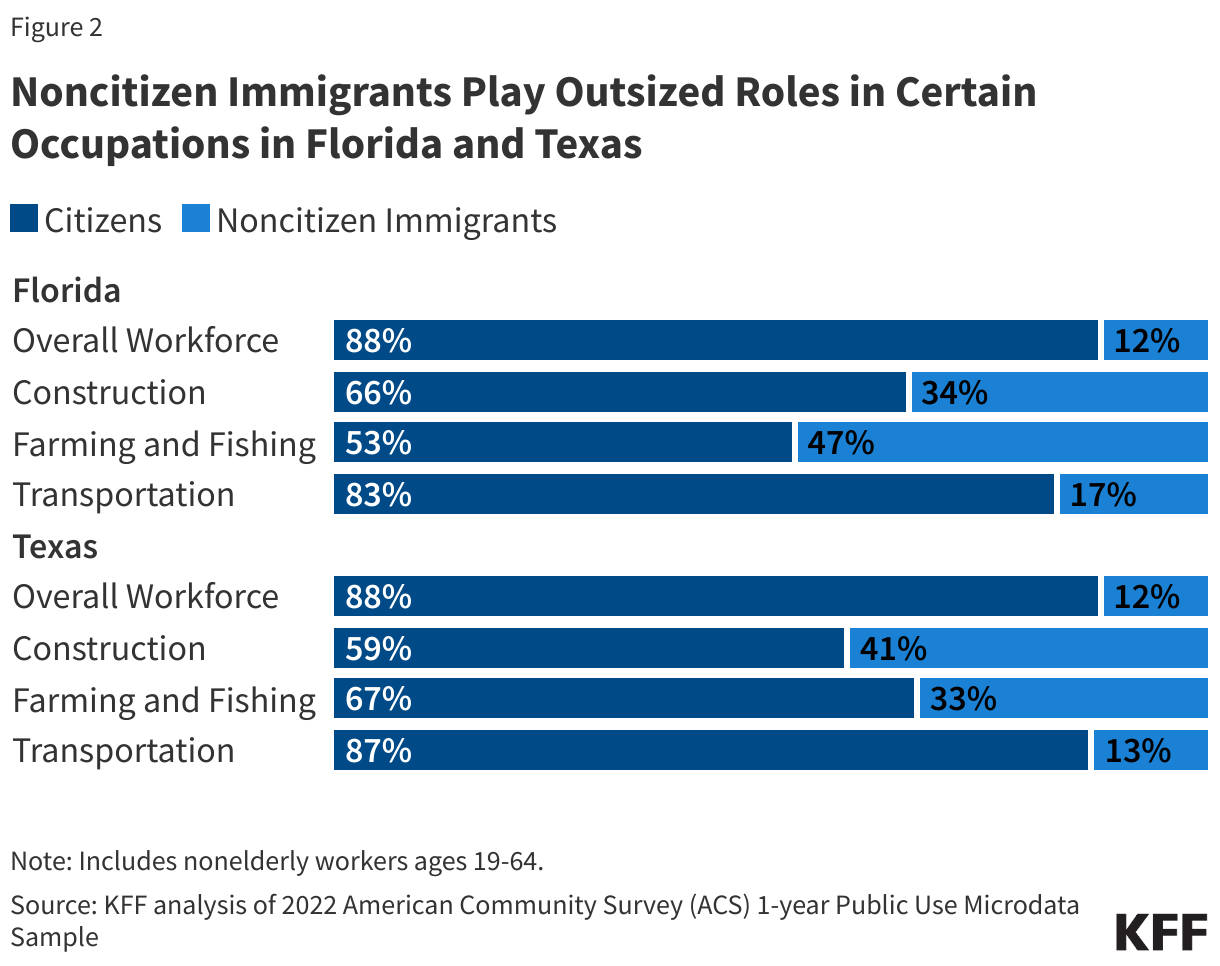
These actions also will likely have implications for the states’ economies and workforces. More limited access to health care can potentially negatively affect worker productivity. Moreover, increased fears among immigrant families may impact their work. Following Florida’s passage of SB 1718, it was reported that food service businesses in the state lost not only long-time employees but also customers who now may be afraid of going to public places. Agriculture and construction industries have also taken a hit, with reports of abandoned construction sites in the state following the passage of SB 1718. It is likely that Texas’ economy and workforce will also be impacted due to the chilling effects of and misinformation around SB 4, even though the law is yet to take effect. These impacts may be especially significant in Florida and Texas due to the outsized role immigrants play in the states’ workforces, particularly in certain occupations. Almost three quarters of nonelderly noncitizen immigrants work, similar to the share of their citizen counterparts. Noncitizen immigrants make up 12% of Florida and Texas’ overall nonelderly adult workforce, but they make up higher shares of workers in certain occupations. In Florida, noncitizen immigrants account for one in three (34%) of the state’s construction workers, almost half (47%) of the state’s farming and fishing workers, and one in six (17%) transportation workers. In Texas, noncitizen immigrants make up four in ten (41%) construction workers, one in three (33%) farming and fishing workers, and about one in eight (13%) transportation workers. The impacts of lost workers in these occupations may have larger ripple effects through the states’ economies and beyond.